You might also like
- KY Auto Insurance ApplicationDocument7 pagesKY Auto Insurance ApplicationRoll Kings0% (1)
- BDO Credit Card Application Form PDFDocument15 pagesBDO Credit Card Application Form PDFJm TabuyanNo ratings yet
- Marriott Bonvoy World Mastercard Credit Card: Welcome To A World of Unparalleled Travel BenefitsDocument8 pagesMarriott Bonvoy World Mastercard Credit Card: Welcome To A World of Unparalleled Travel BenefitsAdeel ArshadNo ratings yet
- Capital OneDocument6 pagesCapital Oneapi-285064294No ratings yet
- Employee Credit Card Authorization FormDocument2 pagesEmployee Credit Card Authorization FormLiza wongNo ratings yet
- HK GRCC Platinum - Transfer-In App FormDocument1 pageHK GRCC Platinum - Transfer-In App FormpercysmithNo ratings yet
- Credit Card Authorization FormDocument2 pagesCredit Card Authorization FormPutu BudaNo ratings yet
- Make Payment By Credit CardDocument1 pageMake Payment By Credit CardLexuNo ratings yet
- Credit Card 3Document8 pagesCredit Card 3api-285960909No ratings yet
- Including The Long Form Fee Disclosure ("List of All Fees.")Document9 pagesIncluding The Long Form Fee Disclosure ("List of All Fees.")Shamara LoganNo ratings yet
- Application For Recurrent Credit Card Payment / Modification FormDocument1 pageApplication For Recurrent Credit Card Payment / Modification FormasdsadsaNo ratings yet
- Credit CardDocument2 pagesCredit Cardapi-3797361100% (1)
- Application For Schengen Visa: Photo This Application Form Is FreeDocument6 pagesApplication For Schengen Visa: Photo This Application Form Is Freeizal alfarizNo ratings yet
- Etihad Credit Card Authorization FormDocument17 pagesEtihad Credit Card Authorization FormFarha AnsariNo ratings yet
- Visa Classic 3. Rupay Classic 6. Mastercard Gold 8. Rupay Platinum 9. Rupay Select CardDocument4 pagesVisa Classic 3. Rupay Classic 6. Mastercard Gold 8. Rupay Platinum 9. Rupay Select CardVikramjeet SinghNo ratings yet
- AUB Credit CardDocument18 pagesAUB Credit CardLovely Jennifer Torremonia IINo ratings yet
- Online Student Identity CardDocument1 pageOnline Student Identity CardEsha Anil JagtapNo ratings yet
- AMERICAN EXPRESS CardNetDocument1 pageAMERICAN EXPRESS CardNetChandan SinghaNo ratings yet
- Receipt for $10 Roblox Gift Card PurchaseDocument2 pagesReceipt for $10 Roblox Gift Card PurchaseCristhian SalazarNo ratings yet
- Credit Card Authorization for Insurance Premium PaymentDocument1 pageCredit Card Authorization for Insurance Premium PaymentShiela EllahNo ratings yet
- PromoSMG Credit Card FormDocument1 pagePromoSMG Credit Card Formmike@promosmg.com100% (3)
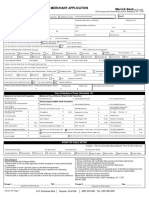
- Merchant Application Merrick Bank: Your Schedule of Fees (Schedule 'A')Document11 pagesMerchant Application Merrick Bank: Your Schedule of Fees (Schedule 'A')Alejandro DuinNo ratings yet
- Payments Can Be Made Using Visa, Mastercard and Discover: Credit Card Payment FormDocument1 pagePayments Can Be Made Using Visa, Mastercard and Discover: Credit Card Payment FormLionel BoopathiNo ratings yet
- Corporation Bank Credit CardsDocument7 pagesCorporation Bank Credit CardsSuriya KJ100% (1)
- Data2 Dapimage 16013003181 CreditCardApplication16013003181Document4 pagesData2 Dapimage 16013003181 CreditCardApplication16013003181yeateshwarriorNo ratings yet
- Document Checklist For MCB Visa Credit Card (Roshan Digital Accountholders)Document16 pagesDocument Checklist For MCB Visa Credit Card (Roshan Digital Accountholders)Abdul AhadNo ratings yet
- StatementDocument3 pagesStatementStephen SnowdenNo ratings yet
- 3584 CS MyAccess ALL 8 2013Document2 pages3584 CS MyAccess ALL 8 2013rasheed-aliNo ratings yet
- Credit Card Transaction Using Face Recognition AuthenticationDocument7 pagesCredit Card Transaction Using Face Recognition AuthenticationRanjan BangeraNo ratings yet
- Mitc For Amazon Pay Credit CardDocument7 pagesMitc For Amazon Pay Credit Cardsomeonestupid19690% (1)
- Duncan, ClaudetteDocument4 pagesDuncan, ClaudetteClaudette DuncanNo ratings yet
- PSU184581461 Auth LetterDocument3 pagesPSU184581461 Auth Letterzihang yanNo ratings yet
- CC Auth Form-CompletedDocument1 pageCC Auth Form-CompletedakshayNo ratings yet
- Pay INZ, VAC Fees & Courier FeeDocument3 pagesPay INZ, VAC Fees & Courier FeeLiano GuerraNo ratings yet
- E Statement 230202100341923391820Document8 pagesE Statement 230202100341923391820Anna HoNo ratings yet
- Your Card Is Approved PDFDocument4 pagesYour Card Is Approved PDFTara ParascandoNo ratings yet
- Secured Card ApplicationDocument1 pageSecured Card Applicationahren gabrielNo ratings yet
- New Balance $4,142.72 Payment Due Date 01/06/17: Platinum Card®Document7 pagesNew Balance $4,142.72 Payment Due Date 01/06/17: Platinum Card®Den JellNo ratings yet
- Credit Card ReconciliationDocument8 pagesCredit Card Reconciliationapi-456055243No ratings yet
- Credit - Report ZMDocument3 pagesCredit - Report ZMEric CartmanNo ratings yet
- Remote Desktop Redirected PrinterDocument2 pagesRemote Desktop Redirected PrinterHARVEY HALPERINNo ratings yet
- Victorias Secret Angel Credit CardDocument21 pagesVictorias Secret Angel Credit Cardapi-285771275No ratings yet
- Colombian Student Visa Application for US StudyDocument3 pagesColombian Student Visa Application for US StudyJose Antonio Valero AtuestaNo ratings yet
- Cardholder AgreementDocument10 pagesCardholder Agreementkaplanallen57No ratings yet
- Renew2 20230902 233754 1750841 201847Document2 pagesRenew2 20230902 233754 1750841 201847peter sismanisNo ratings yet
- Program Choice: International BusinessDocument2 pagesProgram Choice: International BusinessArun GargNo ratings yet
- Business Loan - Application Form & Document ListDocument5 pagesBusiness Loan - Application Form & Document ListsamaadhuNo ratings yet
- CC Charge ReceiptDocument1 pageCC Charge Receiptahmed8056No ratings yet
- American Express Credit Card Features GuideDocument4 pagesAmerican Express Credit Card Features Guidebokamanush100% (1)
- Insurance Team Sent You An Amazon Pay Gift Card! UpdatedDocument3 pagesInsurance Team Sent You An Amazon Pay Gift Card! UpdateddeepakkumaarrNo ratings yet
- Credit Card Application FormDocument4 pagesCredit Card Application FormKrishna Kiran VyasNo ratings yet
- Rewarding Excellence Visa Prepaid Card FaqsDocument4 pagesRewarding Excellence Visa Prepaid Card FaqsjudahNo ratings yet
- Ideposit Merchant ApplicationDocument4 pagesIdeposit Merchant Applicationcris4455No ratings yet
- DuplicateDocument3 pagesDuplicateRamesh KNo ratings yet
- New American ExpressDocument27 pagesNew American Expressamitliarliar100% (2)
- Industry Report On Credit Card Issuing - NrinconDocument7 pagesIndustry Report On Credit Card Issuing - NrinconNick RinconNo ratings yet
- Brac Bank Credit Card ChargeDocument1 pageBrac Bank Credit Card ChargeMehedi HasanNo ratings yet
- HDFC Bank Credit Card ChargesDocument12 pagesHDFC Bank Credit Card ChargesKumar RockyNo ratings yet
- Methods to Overcome the Financial and Money Transfer Blockade against Palestine and any Country Suffering from Financial BlockadeFrom EverandMethods to Overcome the Financial and Money Transfer Blockade against Palestine and any Country Suffering from Financial BlockadeNo ratings yet
- Chris Loomis Private Investigator 626.230.3137Document1 pageChris Loomis Private Investigator 626.230.3137Chris Loomis PINo ratings yet
- The Attorneys Private InvestigatorDocument2 pagesThe Attorneys Private InvestigatorChris Loomis PINo ratings yet
- Warning Signs of A Cheating Spouse and How To Catch ThemDocument5 pagesWarning Signs of A Cheating Spouse and How To Catch ThemChris Loomis PI100% (2)
- Warning Signs of A Cheating Spouse and How To Catch ThemDocument5 pagesWarning Signs of A Cheating Spouse and How To Catch ThemChris Loomis PI100% (2)
- Investigation Request FormDocument2 pagesInvestigation Request FormChris Loomis PINo ratings yet
- Alarm MonitoringDocument430 pagesAlarm Monitoringnnava5051No ratings yet
- Resume Chapter 4: TRANSACTIONAL PROCESSING AND INTERNAL CONTROL PROCESSDocument4 pagesResume Chapter 4: TRANSACTIONAL PROCESSING AND INTERNAL CONTROL PROCESSaryantiyessyNo ratings yet
- Vendor Attestation Policy PDFDocument9 pagesVendor Attestation Policy PDFdinehmetkariNo ratings yet
- ISC CS Practical Specimen PaperDocument2 pagesISC CS Practical Specimen PaperSayak KolayNo ratings yet
- Praveen Sir Hall Ticket 2018Document1 pagePraveen Sir Hall Ticket 2018Rajesh KannaNo ratings yet
- Week8 HomeworkDocument3 pagesWeek8 Homeworkyashar2500No ratings yet
- 2.4.3.6 Lab - The Cybersecurity Cube Scatter QuizletDocument2 pages2.4.3.6 Lab - The Cybersecurity Cube Scatter Quizletluis enrique morel hernadezNo ratings yet
- CYBERCRIME SampangDocument25 pagesCYBERCRIME SampangCyril-J BalboaNo ratings yet
- Caterpillar Sis 2011 Install ManualDocument3 pagesCaterpillar Sis 2011 Install Manualhenotharenas100% (1)
- Mach3 V3.x Programmer Reference Draft v0.11Document141 pagesMach3 V3.x Programmer Reference Draft v0.11Alexandre OliveiraNo ratings yet
- CH 06 I CDocument105 pagesCH 06 I Cbalajinaik07No ratings yet
- RSA Encryption and Decryption ExamplesDocument4 pagesRSA Encryption and Decryption ExamplesRia RoyNo ratings yet
- Calero DecDocument64 pagesCalero DecAngelika CalingasanNo ratings yet
- Wacko Files and PR Response To Judy Stone From Justin Paquette, Brian Lucas, General Counsel OfficeDocument10 pagesWacko Files and PR Response To Judy Stone From Justin Paquette, Brian Lucas, General Counsel OfficeMarkingsonCaseNo ratings yet
- Tune SQL for Oracle PerformanceDocument16 pagesTune SQL for Oracle PerformanceSriram Balasubramanian100% (1)
- ISPS AuditDocument8 pagesISPS AuditIbnu SanusiNo ratings yet
- Tarlac 2019 elections candidates listDocument30 pagesTarlac 2019 elections candidates listJaysonNo ratings yet
- GameTM 003Document170 pagesGameTM 003Gabriel CamposNo ratings yet
- GATE Admit CardDocument1 pageGATE Admit CardRavi Kumar PerimidiNo ratings yet
- Advantages and Disadvantages of Various Graphical Methods: - DotplotsDocument28 pagesAdvantages and Disadvantages of Various Graphical Methods: - DotplotsImran ArshadNo ratings yet
- Manual IOL Master EN PDFDocument8 pagesManual IOL Master EN PDFMirela MarinescuNo ratings yet
- Macete tb6560Document9 pagesMacete tb6560junioratnNo ratings yet
- SOP for E-ProcurementDocument20 pagesSOP for E-Procurementdillipsh123No ratings yet
- Ibm Full Day AgendaDocument1 pageIbm Full Day AgendavbsreddyNo ratings yet
- Crime Hot Spot Prediction-1Document7 pagesCrime Hot Spot Prediction-1Nageswararao NallamothuNo ratings yet
- SoTel CPNIStatement 2012Document2 pagesSoTel CPNIStatement 2012Federal Communications Commission (FCC)No ratings yet
- CPNI Policy CT Communications 2015Document4 pagesCPNI Policy CT Communications 2015Federal Communications Commission (FCC)No ratings yet
- Anne Canteaut Prof. Auth., Henk PDFDocument1,457 pagesAnne Canteaut Prof. Auth., Henk PDFVanroNo ratings yet
- Top 50 Questions of Basic C Programming Asked in InterviewsDocument2 pagesTop 50 Questions of Basic C Programming Asked in InterviewsChaitanya Kumar JinkaNo ratings yet
- ADC0831/ADC0832/ADC0834/ADC0838 8-Bit Serial I/O A/D Converters With Multiplexer OptionsDocument41 pagesADC0831/ADC0832/ADC0834/ADC0838 8-Bit Serial I/O A/D Converters With Multiplexer OptionsSathiya KumarNo ratings yet