You might also like
- Hypoxic-Ischemic Encephalopathy A Review For The ClinicianDocument7 pagesHypoxic-Ischemic Encephalopathy A Review For The ClinicianKaren Carpio100% (1)
- HydrocephalusDocument39 pagesHydrocephalusAjeng Aristiany Rahawarin100% (1)
- Hydrocephalus: I Dewa Ketut Gede Herry Oka Pembimbing: Dr. Dr. I Wayan Niryana, Sp. BS (K)Document40 pagesHydrocephalus: I Dewa Ketut Gede Herry Oka Pembimbing: Dr. Dr. I Wayan Niryana, Sp. BS (K)Dewa Oka100% (1)
- Pediatric Clinical ExaminationDocument3 pagesPediatric Clinical ExaminationAlexander EnnesNo ratings yet
- Convulsions (Seizures) : Prof. Dr. Shahenaz M. HusseinDocument26 pagesConvulsions (Seizures) : Prof. Dr. Shahenaz M. HusseinAriefSuryoWidodo100% (1)
- Notes On History Taking in The Cardiovascular SystemDocument10 pagesNotes On History Taking in The Cardiovascular Systemmdjohar72No ratings yet
- 01 - Normal Newborn and Neurologic ExamDocument4 pages01 - Normal Newborn and Neurologic ExamLuis Elijah De Castro100% (1)
- Alternate History of The WorldDocument2 pagesAlternate History of The WorldCamille Ann Faigao FamisanNo ratings yet
- A Summer Training Project Report OnDocument79 pagesA Summer Training Project Report OnAnkshit Singhal100% (2)
- Febrile Seizure Case FileDocument4 pagesFebrile Seizure Case Filehttps://medical-phd.blogspot.comNo ratings yet
- Endocrine Emergencies in PicuDocument10 pagesEndocrine Emergencies in PicuDr.MohanNo ratings yet
- Epilepsy and Seizure DisordersDocument38 pagesEpilepsy and Seizure DisordersMalueth AnguiNo ratings yet
- Febrile SeizuresDocument11 pagesFebrile SeizuresLita Al AmudiNo ratings yet
- Reye SyndromeDocument10 pagesReye SyndromeDanil KhairulNo ratings yet
- Pain in Children: Advances & Ongoing ChallengesDocument26 pagesPain in Children: Advances & Ongoing ChallengesDeepak SolankiNo ratings yet
- Hydranencephaly ManagementDocument20 pagesHydranencephaly ManagementJohn Christopher LucesNo ratings yet
- Increased Intracranial PressureDocument13 pagesIncreased Intracranial PressureStephanie Talbot100% (1)
- 2016 Pediatric HydrocephalusDocument15 pages2016 Pediatric HydrocephalusYudit Arenita100% (1)
- Approach in Children With SeizuresDocument26 pagesApproach in Children With SeizuresMD Luthfy LubisNo ratings yet
- 10 EpilepsyDocument42 pages10 EpilepsyAhmed aljumailiNo ratings yet
- Bacterial Meningitis in ChildrenDocument10 pagesBacterial Meningitis in ChildrenAnny AryanyNo ratings yet
- Febrile SeizuresDocument23 pagesFebrile SeizuresHafiz FadhliNo ratings yet
- Oral Cases Study Guide - PediatricsDocument68 pagesOral Cases Study Guide - PediatricsJohn100% (1)
- Breath Holding SpellDocument3 pagesBreath Holding SpellDimas Alphiano100% (1)
- Cerebrovascular AccidentDocument6 pagesCerebrovascular AccidentRodel CamposoNo ratings yet
- Hypo ToniaDocument56 pagesHypo ToniaKRITHIKA A/P PALANNY MoeNo ratings yet
- Seizures and Epilepsy: Haining Li General Hospital of Ningxia Medical UniversityDocument50 pagesSeizures and Epilepsy: Haining Li General Hospital of Ningxia Medical UniversityArvindhanNo ratings yet
- Seizures and EpilepsyDocument76 pagesSeizures and EpilepsyManoj GhimireNo ratings yet
- Cyclic VomitingDocument19 pagesCyclic VomitingEmily EresumaNo ratings yet
- SyncopeDocument3 pagesSyncopeanishdNo ratings yet
- Epilepsy and Status EpilepticusDocument112 pagesEpilepsy and Status EpilepticusChingHuaNo ratings yet
- Peads NotesDocument18 pagesPeads Notesechofox11No ratings yet
- Acute Rheumatic Heart DiseaseDocument25 pagesAcute Rheumatic Heart DiseaseArun GeorgeNo ratings yet
- Pediatrics CLIPP From QuizletDocument9 pagesPediatrics CLIPP From QuizletJoe ConeNo ratings yet
- Acute Ataxia in Children: Practice GapsDocument14 pagesAcute Ataxia in Children: Practice Gapsalain reyes100% (1)
- Atresia, Akalasia, EsophaealrefluxDocument3 pagesAtresia, Akalasia, Esophaealrefluxalmira valmaiNo ratings yet
- Rosalina Q. de Sagun, M.D. Maria Antonia Aurora Moral - Valencia, M.DDocument52 pagesRosalina Q. de Sagun, M.D. Maria Antonia Aurora Moral - Valencia, M.DDaphne Jo ValmonteNo ratings yet
- Approach To Cyanotic Heart Disease Christopher Cheung Santokh Dhillon PDFDocument13 pagesApproach To Cyanotic Heart Disease Christopher Cheung Santokh Dhillon PDFsuckeydluffyNo ratings yet
- PAEDIATRICS Notes 3 Update PDFDocument69 pagesPAEDIATRICS Notes 3 Update PDFMateen ShukriNo ratings yet
- Medscape Status EpilepticusDocument10 pagesMedscape Status EpilepticusEllen Siska SusantiNo ratings yet
- CHD ModuleDocument204 pagesCHD ModuleKellie RollinsNo ratings yet
- Case 1Document28 pagesCase 1John Joshua Lacson Medicine100% (1)
- Pyogenic MeningitisDocument46 pagesPyogenic MeningitisShahnaaz ShahNo ratings yet
- Approach To ComaDocument33 pagesApproach To ComaDương Đình ThuậnNo ratings yet
- Meningitis-Malaria E PDFDocument44 pagesMeningitis-Malaria E PDFSana ShafeeqNo ratings yet
- Limping 12.10.2018Document32 pagesLimping 12.10.2018Emily Eresuma100% (1)
- Febrile SeizuresDocument21 pagesFebrile SeizuresIrfan FauziNo ratings yet
- Catatonia Kaplan PDFDocument3 pagesCatatonia Kaplan PDFJuan Sebastian LozanoNo ratings yet
- Cerebrovascular AccidentDocument62 pagesCerebrovascular AccidentJaydee DalayNo ratings yet
- Congenital Heart DiseaseDocument106 pagesCongenital Heart DiseaseHarold DiasanaNo ratings yet
- Tbi Case PresentationDocument22 pagesTbi Case PresentationNinaNo ratings yet
- Hypoxic Ischemic EncephalopathyDocument33 pagesHypoxic Ischemic EncephalopathyDr.P.NatarajanNo ratings yet
- Personal Statement - FinalDocument2 pagesPersonal Statement - Finalapi-383932502No ratings yet
- CPAPDocument53 pagesCPAPvibhurocksNo ratings yet
- Cardiac MurmursDocument28 pagesCardiac MurmursAlvin BlackwellNo ratings yet
- EpilepsyDocument48 pagesEpilepsyvelsyasukriaNo ratings yet
- Simple Febrile Seizures:: Perform A Lumbar Puncture?Document18 pagesSimple Febrile Seizures:: Perform A Lumbar Puncture?smileyginaaNo ratings yet
- Huntington'S Disease: Dhakal, Gerbabuena, Jittwatanatakool, Jordan, KarnDocument25 pagesHuntington'S Disease: Dhakal, Gerbabuena, Jittwatanatakool, Jordan, KarnIrene JordanNo ratings yet
- Meconium AspirationDocument23 pagesMeconium AspirationWitneyGraceNo ratings yet
- Transplantation: Presented by Santhiya K II M.SC Biotechnology 18PBT014Document54 pagesTransplantation: Presented by Santhiya K II M.SC Biotechnology 18PBT014AbiNo ratings yet
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- INFOCUS MANUAL CATARACT SCREENINGF Primary-Eye-Care-Manual-Summary1Document21 pagesINFOCUS MANUAL CATARACT SCREENINGF Primary-Eye-Care-Manual-Summary1Si PuputNo ratings yet
- Risk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriDocument14 pagesRisk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriSi PuputNo ratings yet
- Eye Health in The Commonwealth - Progress Report 2018 To 2020Document30 pagesEye Health in The Commonwealth - Progress Report 2018 To 2020Si PuputNo ratings yet
- Current Management of Vitreous Hemorrhage Due To Proliferative Diabetic RetinopathyDocument11 pagesCurrent Management of Vitreous Hemorrhage Due To Proliferative Diabetic RetinopathySi PuputNo ratings yet
- Towards Universal Eye Health Western PacificDocument28 pagesTowards Universal Eye Health Western PacificSi PuputNo ratings yet
- Normal Postnatal Ocular DevelopmentDocument23 pagesNormal Postnatal Ocular DevelopmentSi PuputNo ratings yet
- Duty Report 18 Januari 2020Document13 pagesDuty Report 18 Januari 2020Si PuputNo ratings yet
- Rapid Sequence InductionDocument2 pagesRapid Sequence InductionSi PuputNo ratings yet
- New Doc 2018-05-04Document2 pagesNew Doc 2018-05-04Si PuputNo ratings yet
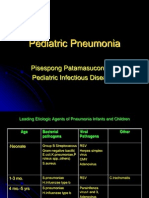
- Pediatric Pneumonia: Pisespong Patamasucon, M.D Pediatric Infectious DiseasesDocument39 pagesPediatric Pneumonia: Pisespong Patamasucon, M.D Pediatric Infectious DiseasesSi PuputNo ratings yet
- General Request Form Graduate School, Chulalongkorn University (Only Use For Educational and Research Scholarship, Graduate School)Document2 pagesGeneral Request Form Graduate School, Chulalongkorn University (Only Use For Educational and Research Scholarship, Graduate School)Kyaw Zin PhyoNo ratings yet
- Lord of The Flies AnalysisDocument10 pagesLord of The Flies AnalysisMuhammad AsifNo ratings yet
- Chenrezi Sadhana A4Document42 pagesChenrezi Sadhana A4kamma100% (7)
- Proiect La EnglezăDocument5 pagesProiect La EnglezăAlexandraNo ratings yet
- Probet DocxuDocument12 pagesProbet DocxuAbuuAwadhNo ratings yet
- Flokulan Air Limbah PDFDocument21 pagesFlokulan Air Limbah PDFanggunNo ratings yet
- The Spartacus Workout 2Document13 pagesThe Spartacus Workout 2PaulFM2100% (1)
- Written Test 4-Book 3Document2 pagesWritten Test 4-Book 3Vinícius MoreiraNo ratings yet
- A Descriptive-Comparative StudyDocument32 pagesA Descriptive-Comparative StudyJanelle DionisioNo ratings yet
- Jurczyk Et Al-2015-Journal of Agronomy and Crop ScienceDocument8 pagesJurczyk Et Al-2015-Journal of Agronomy and Crop ScienceAzhari RizalNo ratings yet
- Revalida ResearchDocument3 pagesRevalida ResearchJakie UbinaNo ratings yet
- Chemical and Biological Weapons Chair ReportDocument9 pagesChemical and Biological Weapons Chair ReportHong Kong MUN 2013100% (1)
- Amazon PrimeDocument27 pagesAmazon PrimeMohamedNo ratings yet
- Indus River Valley Civilization ObjectivesDocument4 pagesIndus River Valley Civilization ObjectivesArslan AsifNo ratings yet
- G.R. No. 178511 - Supreme Court of The PhilippinesDocument4 pagesG.R. No. 178511 - Supreme Court of The PhilippinesJackie Z. RaquelNo ratings yet
- RightShip Inspections Ship Questionaire RISQ 3.0Document207 pagesRightShip Inspections Ship Questionaire RISQ 3.0Philic Rohit100% (1)
- Bond - Chemical Bond (10th-11th Grade)Document42 pagesBond - Chemical Bond (10th-11th Grade)jv peridoNo ratings yet
- 1ST Periodical Test in English 10Document3 pages1ST Periodical Test in English 10kira buenoNo ratings yet
- Battle RoyaleDocument4 pagesBattle RoyalerwNo ratings yet
- Budget Anaplan Training DocumentsDocument30 pagesBudget Anaplan Training DocumentsYudi IfanNo ratings yet
- Safety Management in Coromandel FertilizerDocument7 pagesSafety Management in Coromandel FertilizerS Bharadwaj ReddyNo ratings yet
- Jurnal Arang AktifDocument7 pagesJurnal Arang AktifSurya KrisNo ratings yet
- Resonant Excitation of Coherent Cerenkov Radiation in Dielectric Lined WaveguidesDocument3 pagesResonant Excitation of Coherent Cerenkov Radiation in Dielectric Lined WaveguidesParticle Beam Physics LabNo ratings yet
- Mercury and The WoodmanDocument1 pageMercury and The WoodmanLum Mei YeuanNo ratings yet
- Bomba Watson Marlow PDFDocument13 pagesBomba Watson Marlow PDFRonald SalasNo ratings yet
- Em Swedenborg THE WORD EXPLAINED Volume IX INDICES Academy of The New Church Bryn Athyn PA 1951Document236 pagesEm Swedenborg THE WORD EXPLAINED Volume IX INDICES Academy of The New Church Bryn Athyn PA 1951francis batt100% (2)
- Proximity Principle of DesignDocument6 pagesProximity Principle of DesignSukhdeepNo ratings yet
- 06 - Wreak Bodily HavokDocument40 pages06 - Wreak Bodily HavokJivoNo ratings yet