You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Laampiran ADocument5 pagesLaampiran AMonica Lauretta SembiringNo ratings yet
- GERD Pathophysiology Cleveland ClinicDocument16 pagesGERD Pathophysiology Cleveland ClinicMonica Lauretta SembiringNo ratings yet
- Da PusDocument3 pagesDa PusMonica Lauretta SembiringNo ratings yet
- Epidemiologi Perforasi GasterDocument8 pagesEpidemiologi Perforasi GasterAfiani JannahNo ratings yet
- Peptic UlcerDocument7 pagesPeptic UlcerMonica Lauretta Sembiring0% (1)
- Ev 05 2013 03 1714Document7 pagesEv 05 2013 03 1714Monica Lauretta SembiringNo ratings yet
- Abstrak EnglishDocument2 pagesAbstrak EnglishMonica Lauretta SembiringNo ratings yet
- FoodPoisoning HealthsafetyDocument4 pagesFoodPoisoning HealthsafetyMerlinda Juwita SimanjuntakNo ratings yet
- Comparing Efficacy and Tolerability of Ibuprofen Paracetamol FeverDocument4 pagesComparing Efficacy and Tolerability of Ibuprofen Paracetamol FeverMonica Lauretta SembiringNo ratings yet
- Treating Food Poisoning: Contaminant Onset of Symptoms Foods Affected and Means of TransmissionDocument2 pagesTreating Food Poisoning: Contaminant Onset of Symptoms Foods Affected and Means of TransmissionMonica Lauretta SembiringNo ratings yet
- POA30284Document6 pagesPOA30284Monica Lauretta SembiringNo ratings yet
- LampiranDocument1 pageLampiranGindi Cinintia AsmarantakaNo ratings yet
- Problem Based LearningDocument31 pagesProblem Based LearningMonica Lauretta Sembiring100% (1)
- 1471 2458 12 11Document12 pages1471 2458 12 11Monica Lauretta SembiringNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Animal Experimentation ViewpointsDocument80 pagesAnimal Experimentation ViewpointschristianbarrigaNo ratings yet
- TonsillitisDocument3 pagesTonsillitisVina MuspitaNo ratings yet
- Blake VegliaDocument4 pagesBlake Vegliaapi-400338931No ratings yet
- Annatomy Notes For Bpe StudDocument14 pagesAnnatomy Notes For Bpe StudYoga KalyanamNo ratings yet
- Ccypi 3.0Document76 pagesCcypi 3.0GirishNo ratings yet
- CT Mbbs by DR ShamolDocument197 pagesCT Mbbs by DR ShamolSiva Sandeep Chennimalai50% (2)
- Public Health Implications of Indiscriminate Urination and DefeacationDocument6 pagesPublic Health Implications of Indiscriminate Urination and Defeacationoludoyinmola5ojifinnNo ratings yet
- OpenTexas Checklist Barber Shop CustomersDocument1 pageOpenTexas Checklist Barber Shop CustomersDavid IbanezNo ratings yet
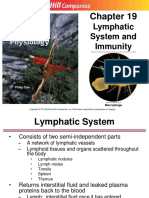
- Chapter 19 - Lymphatic System and ImmunityDocument68 pagesChapter 19 - Lymphatic System and ImmunityAurea Nazaire100% (2)
- Key Points in Obstetrics and Gynecologic Nursing A: Ssessment Formulas !Document6 pagesKey Points in Obstetrics and Gynecologic Nursing A: Ssessment Formulas !June DumdumayaNo ratings yet
- Tutorial Dr. SaugiDocument33 pagesTutorial Dr. SaugifemmytaniaNo ratings yet
- Abnormal Uterine ActionDocument64 pagesAbnormal Uterine ActionKanimozhi Kasinathan100% (1)
- Jaundice Natural RemediesDocument12 pagesJaundice Natural RemediesprkshshrNo ratings yet
- VSR PDFDocument12 pagesVSR PDFDrkrunal badaniNo ratings yet
- KyphosisDocument32 pagesKyphosisBeniamin CostinașNo ratings yet
- Cardiovascular SystemDocument8 pagesCardiovascular SystemHannah Grace CorveraNo ratings yet
- EsquistocitosDocument10 pagesEsquistocitoswillmedNo ratings yet
- Breast Care in BreastfeedingDocument11 pagesBreast Care in BreastfeedingBella Cy LopezNo ratings yet
- D 5 LRDocument2 pagesD 5 LRDianelie BacenaNo ratings yet
- Cestode Parasites: Medical Parasitology, 2009 University of Palangkaraya Agus HaryonoDocument45 pagesCestode Parasites: Medical Parasitology, 2009 University of Palangkaraya Agus HaryonoMeylisa Gerson BayanNo ratings yet
- Hypotonic Hypertonic Isotonic Solutions UsesDocument9 pagesHypotonic Hypertonic Isotonic Solutions UsesImtiaz AhmedNo ratings yet
- Data Interpretation Questions - Temperature RegulationDocument4 pagesData Interpretation Questions - Temperature Regulationtristan reidNo ratings yet
- Reams-RBTI Alphabetical Reference Manual by Stanley & Gertrude Gardner Reams Seminars 1975-1977Document144 pagesReams-RBTI Alphabetical Reference Manual by Stanley & Gertrude Gardner Reams Seminars 1975-1977Steve DiverNo ratings yet
- Are You Kidding MeDocument10 pagesAre You Kidding MeChelsea RoseNo ratings yet
- OrDocument56 pagesOrRosalyn YuNo ratings yet
- Đề 4. Đề Thi Thử TN THPT Môn Tiếng Anh Theo Cấu Trúc Đề Minh Họa 2021 - Cô Oanh - Có Lời GiảiDocument15 pagesĐề 4. Đề Thi Thử TN THPT Môn Tiếng Anh Theo Cấu Trúc Đề Minh Họa 2021 - Cô Oanh - Có Lời GiảiBình Bùi thanhNo ratings yet
- Cardiac MonitorDocument3 pagesCardiac MonitorShameera M. KamlianNo ratings yet
- Cs Breast EngorgementDocument14 pagesCs Breast Engorgementamit85% (13)
- MATERNALDocument32 pagesMATERNALsean blaze100% (1)
- Blood Pressure RegulationDocument11 pagesBlood Pressure RegulationPaulShaneHerreraZorrillaNo ratings yet