You might also like
- Blood Transfusion Basic Concepts Blood Transfusion inDocument103 pagesBlood Transfusion Basic Concepts Blood Transfusion iniahmad9No ratings yet
- RANASINGHE Blood and Blood ProductsDocument63 pagesRANASINGHE Blood and Blood ProductsDagimNo ratings yet
- Blood Component TherapyDocument13 pagesBlood Component TherapyMohamed ElgayarNo ratings yet
- Transfusion Therapy (4!10!2016)Document32 pagesTransfusion Therapy (4!10!2016)vishnuNo ratings yet
- Blood TransfusionDocument28 pagesBlood TransfusionhanibalbalNo ratings yet
- 1 Transfusion1 PDFDocument7 pages1 Transfusion1 PDFVatha NaNo ratings yet
- Transfusion Medicine by Dr. Sharad JohriDocument54 pagesTransfusion Medicine by Dr. Sharad JohriShashwat JohriNo ratings yet
- Blood Transfusion 2Document12 pagesBlood Transfusion 2Helene AlawamiNo ratings yet
- Transfusion TherapyDocument61 pagesTransfusion TherapyAinun Zamira HabieNo ratings yet
- TransfusionDocument19 pagesTransfusionSrishti SrivastavaNo ratings yet
- Blood TransfusionDocument50 pagesBlood TransfusionSerat Rahman100% (2)
- Blood Administration: NRS 108 Essec County CollegeDocument22 pagesBlood Administration: NRS 108 Essec County CollegeDiah Puspita RiniNo ratings yet
- Blood TransfusionDocument59 pagesBlood Transfusionpranalika .................76% (17)
- Blood Transfusion ICUDocument64 pagesBlood Transfusion ICUSherif ElbadrawyNo ratings yet
- Restricting and Avoiding Blood Transfusions: What Options Do We Have?Document41 pagesRestricting and Avoiding Blood Transfusions: What Options Do We Have?Deepak SolankiNo ratings yet
- 4 - Hemorrhage and Blood TransfusionDocument15 pages4 - Hemorrhage and Blood Transfusionnightfury200313No ratings yet
- 11a. Blood TransfusionDocument28 pages11a. Blood TransfusionMuwanga faizoNo ratings yet
- Blood TransfusionDocument74 pagesBlood Transfusiontefesih tube ተፈስሕ ቲዮብNo ratings yet
- ICU Blood Transfusion & Electrolytes DisturbanceDocument26 pagesICU Blood Transfusion & Electrolytes Disturbancef6080683No ratings yet
- Physiology of Transfusion TherapyDocument34 pagesPhysiology of Transfusion Therapyterara0% (1)
- Blood Components - DR. ETU-EFEOTOR T. P.Document40 pagesBlood Components - DR. ETU-EFEOTOR T. P.Princewill Seiyefa100% (1)
- Information Sheet For Candidate: General CommentsDocument4 pagesInformation Sheet For Candidate: General Commentsfire_n_iceNo ratings yet
- Transfusion Medicine: DR Abdullah AnsariDocument53 pagesTransfusion Medicine: DR Abdullah AnsariFabsNo ratings yet
- Pediatric TransfusionDocument82 pagesPediatric TransfusionMia Lesaca-Medina100% (2)
- Blood Administration and Transfusion Reactions QuizDocument5 pagesBlood Administration and Transfusion Reactions Quizremooheshmat100% (1)
- Blood TransfusionDocument32 pagesBlood TransfusionsallaxleyNo ratings yet
- Transfusion TherapyDocument6 pagesTransfusion TherapyMohamad AttiaNo ratings yet
- Blood Transfusion (3) - 123Document44 pagesBlood Transfusion (3) - 123AjeeshNo ratings yet
- MCQs For LaboratoryDocument42 pagesMCQs For Laboratorynarendrakumar94100% (1)
- TransfusionDocument48 pagesTransfusionSandy LavedaNo ratings yet
- Hypovolemic Shock ResuscitationDocument21 pagesHypovolemic Shock ResuscitationM Lutfi FananiNo ratings yet
- Blood Transfusion and Conservation During SurgeryDocument86 pagesBlood Transfusion and Conservation During SurgeryajefolakemijohnNo ratings yet
- Blood Bank 3Document20 pagesBlood Bank 3moonfire2009100% (2)
- 6.blood Transfusion, Hemostasis & Coagulation DisordersDocument42 pages6.blood Transfusion, Hemostasis & Coagulation DisordersEyouel TadesseNo ratings yet
- Blood Products and Their UsesDocument28 pagesBlood Products and Their UsesJeevitha Vanitha100% (1)
- Blood & Blood Products OnlyDocument54 pagesBlood & Blood Products OnlydrprasadingleyNo ratings yet
- Transfusion Medicine QuestionsDocument32 pagesTransfusion Medicine QuestionsMahmoud RamlawiNo ratings yet
- HPB Adverse Transfusion ReactionDocument26 pagesHPB Adverse Transfusion ReactionFransiscus RivaldyNo ratings yet
- Blood Component TherapyDocument8 pagesBlood Component TherapyquerokeropiNo ratings yet
- Blood Transfusion TherapyDocument5 pagesBlood Transfusion TherapyDots DyNo ratings yet
- Surgery Slide 6 - Blood TransfusionsDocument54 pagesSurgery Slide 6 - Blood TransfusionsEman NazzalNo ratings yet
- 4 Blood ProductsDocument11 pages4 Blood ProductsGampa VijaykumarNo ratings yet
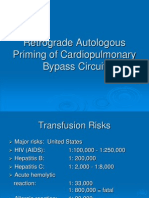
- Retrograde Autologous Priming of Cardiopulmonary Bypass CircuitDocument18 pagesRetrograde Autologous Priming of Cardiopulmonary Bypass CircuitMuhammad Badrushshalih100% (2)
- Blood and Its ProductsDocument23 pagesBlood and Its Productsمحمد عماد عليNo ratings yet
- Transfusi 1Document22 pagesTransfusi 1Andre Christian SopacuaNo ratings yet
- David Harford Hematology/OncologyDocument42 pagesDavid Harford Hematology/OncologychrisNo ratings yet
- Blood Transfusion TherapyDocument5 pagesBlood Transfusion TherapyHayes CloverNo ratings yet
- Overview of Blood Transfusion For Management of Complicated CasesDocument31 pagesOverview of Blood Transfusion For Management of Complicated CasesVivek NairNo ratings yet
- Blood and Its ComponentsDocument30 pagesBlood and Its ComponentskushalNo ratings yet
- Hemostasis and Transfusion MedicineDocument83 pagesHemostasis and Transfusion MedicineJesserene Mangulad SorianoNo ratings yet
- 2-Transfusion of Blood and Blood ProductsDocument47 pages2-Transfusion of Blood and Blood ProductsAiden JosephatNo ratings yet
- Blood ComponentsDocument51 pagesBlood ComponentsMandy A. Delfin100% (1)
- MCQs For LaboratoryDocument42 pagesMCQs For LaboratorySami Khan87% (68)
- Blood Transfusion SeminarDocument58 pagesBlood Transfusion SeminarsharewdelelegnNo ratings yet
- Bleeding Complications Aw C BypassDocument18 pagesBleeding Complications Aw C BypassPruthvi RajNo ratings yet
- Blood TransfusionDocument35 pagesBlood TransfusionMarvin Dela Cruz100% (1)
- Lab Technologist 11Document43 pagesLab Technologist 11AHAMED SHIFAANNo ratings yet
- Homologous Blood Trasfusion Practice ShortsDocument23 pagesHomologous Blood Trasfusion Practice ShortsdrprasadingleyNo ratings yet
- Adverse Effects of Blood TransfusionsDocument3 pagesAdverse Effects of Blood Transfusionsay254No ratings yet
- Toxicology ICU PDFDocument49 pagesToxicology ICU PDFAhmed Shihab AhmedNo ratings yet
- Respiratory ICU PDFDocument130 pagesRespiratory ICU PDFAhmed Shihab AhmedNo ratings yet
- Cardiovascular Pharmacology PDFDocument85 pagesCardiovascular Pharmacology PDFAhmed Shihab AhmedNo ratings yet
- Cardiovascular ICU PDFDocument170 pagesCardiovascular ICU PDFAhmed Shihab AhmedNo ratings yet
- MCQ Anaesthesia AnswersDocument4 pagesMCQ Anaesthesia Answersapi-26291651100% (3)
- Europe Heatwave: Why Are Temperatures On The Continent Soaring?Document3 pagesEurope Heatwave: Why Are Temperatures On The Continent Soaring?Alec LoaiNo ratings yet
- DarwinDocument118 pagesDarwinmrthumb100% (2)
- Performing Chest PhysiotherapyDocument14 pagesPerforming Chest PhysiotherapyDivya Chauhan100% (1)
- Domiciliary Midwifery RDocument16 pagesDomiciliary Midwifery Rswillymadhu83% (6)
- PEMF Therapy Controls Physical Effects of StressDocument2 pagesPEMF Therapy Controls Physical Effects of StressAndreas LooseNo ratings yet
- Journal of Clinical and Diagnostic ResearchDocument5 pagesJournal of Clinical and Diagnostic ResearchBoedyNo ratings yet
- Chapter 7. CirculationDocument54 pagesChapter 7. CirculationankurbiologyNo ratings yet
- IAPHD Hand Book On Palliative Care PDFDocument37 pagesIAPHD Hand Book On Palliative Care PDFMohammed ArshadNo ratings yet
- Ludwig's AnginaDocument22 pagesLudwig's AnginaDevavrat SinghNo ratings yet
- Maintenance Fluid Therapy in ChildrenDocument4 pagesMaintenance Fluid Therapy in ChildrenNicole_0No ratings yet
- Binomial 2 Distribution ProblemsDocument1 pageBinomial 2 Distribution ProblemsAnonymous 105zV1No ratings yet
- Introduction of CKDDocument7 pagesIntroduction of CKDAndrelyn Balangui LumingisNo ratings yet
- Autoimmune Hemolytic Anemia in Adults 2019 PDFDocument22 pagesAutoimmune Hemolytic Anemia in Adults 2019 PDFKevin Mora BañosNo ratings yet
- TLE10 - 2nd Quarter Module 1Document5 pagesTLE10 - 2nd Quarter Module 1VernaNo ratings yet
- Active Transport by ATP-Powered Pumps - Molecular Cell Biology - NCBI BookshelfDocument10 pagesActive Transport by ATP-Powered Pumps - Molecular Cell Biology - NCBI BookshelfMuhammad KhanNo ratings yet
- (Dental Discussion 1) - Hesy ReDocument32 pages(Dental Discussion 1) - Hesy ReethanNo ratings yet
- COVID Jab Spike Remains in Body, Affects DNA - 1 Holistic Way To Repair DNA and Reduce Spike DamageDocument15 pagesCOVID Jab Spike Remains in Body, Affects DNA - 1 Holistic Way To Repair DNA and Reduce Spike DamageTUTO TUTONo ratings yet
- Pharmacology of Drugs For PPHDocument55 pagesPharmacology of Drugs For PPHFaye CagayanNo ratings yet
- RLE Module 2M - Chest Physiotherapy, Postural Drainage, Nebulization, Chest Tube Drainage Systems, Blood TransfusionDocument57 pagesRLE Module 2M - Chest Physiotherapy, Postural Drainage, Nebulization, Chest Tube Drainage Systems, Blood TransfusionAlexa GoteraNo ratings yet
- Impact of COVID-19 On Marketing AmityDocument59 pagesImpact of COVID-19 On Marketing AmitySudha RaniNo ratings yet
- Recommendations For Rescue of A Submerged Unresponsive Compressed-Gas DiverDocument10 pagesRecommendations For Rescue of A Submerged Unresponsive Compressed-Gas Diverwyma01No ratings yet
- Australian Biology Olympiad 2009Document41 pagesAustralian Biology Olympiad 2009Science Olympiad Blog100% (1)
- RPH - The Importance of Balanced DietDocument7 pagesRPH - The Importance of Balanced DietHafizah RamllyNo ratings yet
- 2009 Fee ScheduleDocument1,123 pages2009 Fee ScheduleNicole HillNo ratings yet
- Scientific Book Jicccim 2018Document171 pagesScientific Book Jicccim 2018ngwinda90No ratings yet
- Chorti DictionaryDocument285 pagesChorti DictionaryLuis Bedoya100% (1)
- Application Form: Tata Aia Life Insurance Company LimitedDocument6 pagesApplication Form: Tata Aia Life Insurance Company LimitedpritamNo ratings yet
- Tens Vitalcontrol PDFDocument20 pagesTens Vitalcontrol PDFOscar BravoNo ratings yet
- P.E EssayDocument2 pagesP.E EssayMia LucinaNo ratings yet
- 2024 04 04 SSCP Oversight EC Letter To Daszak 6c867682d6Document12 pages2024 04 04 SSCP Oversight EC Letter To Daszak 6c867682d6Jennifer Van LaarNo ratings yet
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (31)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (60)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (5)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Empath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainFrom EverandEmpath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainRating: 4 out of 5 stars4/5 (95)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)