You might also like
- Soft Tissue TumorsDocument38 pagesSoft Tissue TumorsRah Ma GhassanNo ratings yet
- 23 Soft Tissue TumorsDocument115 pages23 Soft Tissue TumorsorliandoNo ratings yet
- Benign Oral Tumors of Mesenchymal Tissue OriginDocument55 pagesBenign Oral Tumors of Mesenchymal Tissue Originfilyouth4lifeNo ratings yet
- I.T.S Dental College, Greater NoidaDocument48 pagesI.T.S Dental College, Greater NoidaAMIT GUPTANo ratings yet
- Non Odontogenic Tumor of Vascular Tissue: Asanuo Yiese Roll Number:12Document40 pagesNon Odontogenic Tumor of Vascular Tissue: Asanuo Yiese Roll Number:12Rajat NangiaNo ratings yet
- FibromaDocument4 pagesFibromaAhmed AbdelrazekNo ratings yet
- Bone and Soft Tissue PathologyDocument74 pagesBone and Soft Tissue PathologyBayan HamedNo ratings yet
- Salivary Glands: Dr. Tanuj Paul BhatiaDocument83 pagesSalivary Glands: Dr. Tanuj Paul BhatiaNgnNo ratings yet
- Idiopathic Non Neoplastic Salivary Gland DiseasesDocument33 pagesIdiopathic Non Neoplastic Salivary Gland Diseasesgud4nothingNo ratings yet
- Non-Odontogenic Benign and Malignant Tumours of Fibrous Tissue OriginDocument52 pagesNon-Odontogenic Benign and Malignant Tumours of Fibrous Tissue OriginRajat NangiaNo ratings yet
- BenignDocument63 pagesBenignAFREEN SADAFNo ratings yet
- BDS10012 Oral HyperplasiaDocument50 pagesBDS10012 Oral Hyperplasiahabibahafez282No ratings yet
- Oral Cavity Malignancy-SurgeryDocument62 pagesOral Cavity Malignancy-SurgeryAsif AbbasNo ratings yet
- Systemic Diseases That Cause Gingival Enlargement: LeukemiaDocument7 pagesSystemic Diseases That Cause Gingival Enlargement: LeukemiaCristinaNo ratings yet
- Oral Pathology I Final ReviewDocument373 pagesOral Pathology I Final ReviewAlex ChangNo ratings yet
- Physical and Chemical Injuries: Oral Complications of H and N Radiation TherapyDocument5 pagesPhysical and Chemical Injuries: Oral Complications of H and N Radiation TherapynewmexicoomfsNo ratings yet
- Benign and Malignant Tumor of The Oral CavityDocument82 pagesBenign and Malignant Tumor of The Oral CavitymelNo ratings yet
- Precancerous Conditions of Oral CavityDocument80 pagesPrecancerous Conditions of Oral Cavitylarisabrinza12No ratings yet
- Diseases of SkinDocument12 pagesDiseases of SkinpayalpachiNo ratings yet
- Oral Pathology Hereditary Conditions: Group IDocument74 pagesOral Pathology Hereditary Conditions: Group IFatima CarlosNo ratings yet
- Gingival Enlargement: by Hamza AJALDocument22 pagesGingival Enlargement: by Hamza AJALajal hamzaNo ratings yet
- Vascular Tumors: Pgi Pauline BaluisDocument114 pagesVascular Tumors: Pgi Pauline BaluisPahw BaluisNo ratings yet
- Periapical Pathologies: Namrata Sengupta Mds (Ii) Guided By: Dr. Sachin Sarode Presented On: 28 May, 2021Document73 pagesPeriapical Pathologies: Namrata Sengupta Mds (Ii) Guided By: Dr. Sachin Sarode Presented On: 28 May, 2021Madhura ShekatkarNo ratings yet
- 12-Giant Cell LesionDocument78 pages12-Giant Cell Lesionفراس الموسويNo ratings yet
- Oral Diagnosis and Treatment Planning IIDocument19 pagesOral Diagnosis and Treatment Planning IIAIME WILFRIED BEASSO FOZOCKNo ratings yet
- Oral & Maxillofacial Pathology II: Topic: Soft Tissue TumorsDocument123 pagesOral & Maxillofacial Pathology II: Topic: Soft Tissue TumorsDorina MalanceaNo ratings yet
- Lec. 13 &14 Epithelial DisordersDocument10 pagesLec. 13 &14 Epithelial DisordersZainab AlshamaryNo ratings yet
- Non-Odontogenic Tumors of Nerve Tissue Origin: Submitted by - Anjali Tomar Roll No. 10Document37 pagesNon-Odontogenic Tumors of Nerve Tissue Origin: Submitted by - Anjali Tomar Roll No. 10Rajat NangiaNo ratings yet
- Intraoral Benign TumorsDocument4 pagesIntraoral Benign TumorsSaman SadeghiNo ratings yet
- امراض الفم سنة ثالثة المحاضرات 5 8Document64 pagesامراض الفم سنة ثالثة المحاضرات 5 8f.aljaremNo ratings yet
- Test 4 Study GuideDocument22 pagesTest 4 Study GuideSagal NurNo ratings yet
- Skin LesionDocument23 pagesSkin Lesion5alifa55No ratings yet
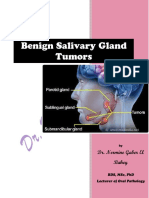
- Benign Salivary Gland Tumors - Dr. Nermine El Bahey (2019-2020)Document13 pagesBenign Salivary Gland Tumors - Dr. Nermine El Bahey (2019-2020)MOHAMED AMINNo ratings yet
- Benign Vulvar Lesions: DR Sally Sayed El-Tawab Lecturer of Gyne-Oncology Alexandria UniversityDocument34 pagesBenign Vulvar Lesions: DR Sally Sayed El-Tawab Lecturer of Gyne-Oncology Alexandria Universitysalah subbahNo ratings yet
- Developmental Disturbances of The Oral Mucosa, Gingiva and TongueDocument51 pagesDevelopmental Disturbances of The Oral Mucosa, Gingiva and Tonguekavin_sandhu100% (1)
- Traumatic FibromaDocument17 pagesTraumatic FibromaGeorgie TagataNo ratings yet
- Necrotizing SialometaplasiaDocument33 pagesNecrotizing SialometaplasiaJessica GreenNo ratings yet
- Oral Pathology NotesDocument162 pagesOral Pathology NotesDaniel Atieh100% (1)
- Eyelids Diseases Lacrimal System DiseasesDocument45 pagesEyelids Diseases Lacrimal System DiseasesMAMA LALANo ratings yet
- Papillary Lesions: See PictureDocument6 pagesPapillary Lesions: See Pictureasas asadNo ratings yet
- Nasal TumorDocument20 pagesNasal TumorMahmoud ElsherbenyNo ratings yet
- Slide 1 +2 CT Hyperplasia Slide 1 2Document115 pagesSlide 1 +2 CT Hyperplasia Slide 1 2CWT2010No ratings yet
- Oral Patho Lecture Shlav BDocument65 pagesOral Patho Lecture Shlav Bشبيبةالروم الملكيين الكاثوليكNo ratings yet
- Red Blue LesinDocument77 pagesRed Blue LesinWeam FarounNo ratings yet
- Dermal and Subcutaneous TumorsDocument76 pagesDermal and Subcutaneous Tumorsreeves_coolNo ratings yet
- FimosisDocument9 pagesFimosiselsa relandaNo ratings yet
- Lipoma & Kista AtheromaDocument24 pagesLipoma & Kista AtheromaAgnes NiyNo ratings yet
- Immune Mediated DisordersDocument153 pagesImmune Mediated DisordersHaroon ButtNo ratings yet
- Benign Neoplasms and HyperplasiasDocument19 pagesBenign Neoplasms and HyperplasiasimperiouxxNo ratings yet
- DERMADocument141 pagesDERMAKenneth NuñezNo ratings yet
- Ilovepdf MergedDocument22 pagesIlovepdf MergedSRO oONo ratings yet
- Salivarg Gland DisorderDocument26 pagesSalivarg Gland DisorderLaraib KanwalNo ratings yet
- Fibrous Tumors: Pgi Pauline BaluisDocument69 pagesFibrous Tumors: Pgi Pauline BaluisPahw BaluisNo ratings yet
- Benign and Premalignant LesionsDocument25 pagesBenign and Premalignant LesionsAyush PaudelNo ratings yet
- Oral Medicin White &red LesionsDocument12 pagesOral Medicin White &red LesionsQueen LiveNo ratings yet
- Hpe Final 110529Document98 pagesHpe Final 110529deeps.u.97No ratings yet
- Disease of Lids and Lacrim Al Apparatus: The First Affiliated Hospital of Zhengzhou UniversityDocument46 pagesDisease of Lids and Lacrim Al Apparatus: The First Affiliated Hospital of Zhengzhou Universityapi-19916399No ratings yet
- Sebaceous Cyst, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandSebaceous Cyst, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Dermatology Notes for Medical StudentsFrom EverandDermatology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (5)
- Oral Medicine & Pathology from A-ZFrom EverandOral Medicine & Pathology from A-ZRating: 5 out of 5 stars5/5 (9)
- HIV AIDS PPT (Compatibility Mode)Document20 pagesHIV AIDS PPT (Compatibility Mode)Champak PaulNo ratings yet
- Diseases of Gall Bladder & Bile DuctsDocument24 pagesDiseases of Gall Bladder & Bile DuctsChampak PaulNo ratings yet
- Soft Tissue Tumors (Chapter 12) : FibromaDocument12 pagesSoft Tissue Tumors (Chapter 12) : FibromaChampak PaulNo ratings yet
- Dent A EquipmDocument70 pagesDent A EquipmChampak PaulNo ratings yet
- CANINE Impaction Oral SurgeryDocument64 pagesCANINE Impaction Oral SurgeryChampak PaulNo ratings yet
- Extensive Hypertrophic Lichen Planus in An... (Dermatol Online JDocument1 pageExtensive Hypertrophic Lichen Planus in An... (Dermatol Online JChampak PaulNo ratings yet
- A Melo Blast OmaDocument10 pagesA Melo Blast OmaChampak PaulNo ratings yet
- Disorders: J = ( (Pc − Pi) − σ (πc − πi) )Document113 pagesDisorders: J = ( (Pc − Pi) − σ (πc − πi) )Champak PaulNo ratings yet
- AIDS Picture (Hardin MD Super Site Sample)Document2 pagesAIDS Picture (Hardin MD Super Site Sample)Champak PaulNo ratings yet
- Chapter 12 Powerpoint LDocument50 pagesChapter 12 Powerpoint LDennis Nabor Muñoz, RN,RMNo ratings yet
- Oral Lichen PlannusDocument1 pageOral Lichen PlannusChampak PaulNo ratings yet
- Head IV Cranial NervesDocument18 pagesHead IV Cranial NervesChampak PaulNo ratings yet
- Developmental Disturbances ofDocument93 pagesDevelopmental Disturbances ofChampak PaulNo ratings yet
- Pathogenesis of PemphigusDocument47 pagesPathogenesis of PemphigusChampak PaulNo ratings yet
- HIV AIDS PPT (Compatibility Mode)Document20 pagesHIV AIDS PPT (Compatibility Mode)Champak PaulNo ratings yet
- Respiratory System IntroductionDocument63 pagesRespiratory System IntroductionChampak PaulNo ratings yet
- 2.2. Oral PrecancerDocument20 pages2.2. Oral PrecancerChampak PaulNo ratings yet
- Peripheral Ossifying FibromaDocument7 pagesPeripheral Ossifying FibromaChampak Paul100% (1)
- Examination of The Oral Cavity2Document63 pagesExamination of The Oral Cavity2Champak PaulNo ratings yet
- 8d46the Oral CavityDocument33 pages8d46the Oral CavityChampak PaulNo ratings yet
- Blood Coagulation DisordersDocument65 pagesBlood Coagulation DisordersChampak PaulNo ratings yet
- Fibroosseous LesionsDocument17 pagesFibroosseous LesionsChampak PaulNo ratings yet
- 2.2. Oral PrecancerDocument20 pages2.2. Oral PrecancerChampak PaulNo ratings yet
- Odontogenic CystDocument5 pagesOdontogenic CystChampak PaulNo ratings yet
- Enamel HypoplasiaDocument2 pagesEnamel Hypoplasiakonda_siri83100% (1)
- Orthodontic AppliancesDocument38 pagesOrthodontic AppliancesChampak PaulNo ratings yet
- Orthodontic AppliancesDocument38 pagesOrthodontic AppliancesChampak PaulNo ratings yet
- Benjamin Franklin - The Indian Treaties (1938)Document450 pagesBenjamin Franklin - The Indian Treaties (1938)Spiritu SanctoNo ratings yet
- Java Complete Collection FrameworkDocument28 pagesJava Complete Collection FrameworkkhushivanshNo ratings yet
- DN102-R0-GPJ-Design of Substructure & Foundation 28m+28m Span, 19.6m Width, 22m Height PDFDocument64 pagesDN102-R0-GPJ-Design of Substructure & Foundation 28m+28m Span, 19.6m Width, 22m Height PDFravichandraNo ratings yet
- Liquitex Soft Body BookletDocument12 pagesLiquitex Soft Body Booklethello belloNo ratings yet
- Contemporary Philippine Arts From The Regions: Quarter 1Document11 pagesContemporary Philippine Arts From The Regions: Quarter 1JUN GERONANo ratings yet
- Marketing Micro and Macro EnvironmentDocument8 pagesMarketing Micro and Macro EnvironmentSumit Acharya100% (1)
- Aribah Ahmed CertificateDocument2 pagesAribah Ahmed CertificateBahadur AliNo ratings yet
- Republic of The Philippines Division of Bohol Department of Education Region VII, Central VisayasDocument6 pagesRepublic of The Philippines Division of Bohol Department of Education Region VII, Central VisayasJOHN MC RAE RACINESNo ratings yet
- Gastroesophagea L of Reflux Disease (GERD)Document34 pagesGastroesophagea L of Reflux Disease (GERD)Alyda Choirunnissa SudiratnaNo ratings yet
- DS Important QuestionsDocument15 pagesDS Important QuestionsLavanya JNo ratings yet
- CTS2 HMU Indonesia - Training - 09103016Document45 pagesCTS2 HMU Indonesia - Training - 09103016Resort1.7 Mri100% (1)
- BÀI TẬP LESSON 7. CÂU BỊ ĐỘNG 1Document4 pagesBÀI TẬP LESSON 7. CÂU BỊ ĐỘNG 1Yến Vy TrầnNo ratings yet
- Case 3 SectionC Group 1 (Repaired)Document3 pagesCase 3 SectionC Group 1 (Repaired)SANDEEP AGRAWALNo ratings yet
- Positive Psychology in The WorkplaceDocument12 pagesPositive Psychology in The Workplacemlenita264No ratings yet
- Measurement and Scaling Techniques1Document42 pagesMeasurement and Scaling Techniques1Ankush ChaudharyNo ratings yet
- Reflection in Sexually Transmitted DiseaseDocument1 pageReflection in Sexually Transmitted Diseasewenna janeNo ratings yet
- Reflection On The PoorDocument5 pagesReflection On The Poorapi-347831792No ratings yet
- FINAL BÁO-CÁO-THỰC-TẬP.editedDocument38 pagesFINAL BÁO-CÁO-THỰC-TẬP.editedngocthaongothi4No ratings yet
- Possessive Determiners: A. 1. A) B) C) 2. A) B) C) 3. A) B) C) 4. A) B) C) 5. A) B) C) 6. A) B) C) 7. A) B) C)Document1 pagePossessive Determiners: A. 1. A) B) C) 2. A) B) C) 3. A) B) C) 4. A) B) C) 5. A) B) C) 6. A) B) C) 7. A) B) C)Manuela Marques100% (1)
- UFO Yukon Spring 2010Document8 pagesUFO Yukon Spring 2010Joy SimsNo ratings yet
- KMKT Pra PSPM ANS SCHEMEDocument16 pagesKMKT Pra PSPM ANS SCHEMEElda AldaNo ratings yet
- Bench-Scale Decomposition of Aluminum Chloride Hexahydrate To Produce Poly (Aluminum Chloride)Document5 pagesBench-Scale Decomposition of Aluminum Chloride Hexahydrate To Produce Poly (Aluminum Chloride)varadjoshi41No ratings yet
- Final MS Access Project Class-10Document17 pagesFinal MS Access Project Class-10aaas44% (9)
- GCP Vol 2 PDF (2022 Edition)Document548 pagesGCP Vol 2 PDF (2022 Edition)Sergio AlvaradoNo ratings yet
- Generalized Class of Sakaguchi Functions in Conic Region: Saritha. G. P, Fuad. S. Al Sarari, S. LathaDocument5 pagesGeneralized Class of Sakaguchi Functions in Conic Region: Saritha. G. P, Fuad. S. Al Sarari, S. LathaerpublicationNo ratings yet
- 2023 Teacher Email ListDocument5 pages2023 Teacher Email ListmunazamfbsNo ratings yet
- Spectacle Blinds - Closed Blinds Open Blinds (Ring Spacer)Document2 pagesSpectacle Blinds - Closed Blinds Open Blinds (Ring Spacer)Widiyanto WiwidNo ratings yet
- 35 Electrical Safety SamanDocument32 pages35 Electrical Safety SamanSaman Sri Ananda RajapaksaNo ratings yet
- Low Speed Aerators PDFDocument13 pagesLow Speed Aerators PDFDgk RajuNo ratings yet
- Pelayo PathopyhsiologyDocument13 pagesPelayo PathopyhsiologyE.J. PelayoNo ratings yet