You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Satisfactory VoucherDocument1 pageSatisfactory Vouchervrevatienterprises100% (2)
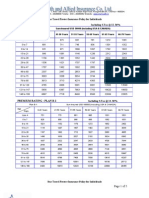
- Individual Travel Protect Premium Chart ST 12.36%Document5 pagesIndividual Travel Protect Premium Chart ST 12.36%vrevatienterprisesNo ratings yet
- Shriram Claim FormDocument2 pagesShriram Claim FormvrevatienterprisesNo ratings yet
- Sbi Claim FormDocument4 pagesSbi Claim FormvrevatienterprisesNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 3.1 - Sequences and SeriesxbxhhdDocument92 pages3.1 - Sequences and SeriesxbxhhdHelloNo ratings yet
- Solid Modeling Techniques: Constructive Solid Geometry (CSG)Document22 pagesSolid Modeling Techniques: Constructive Solid Geometry (CSG)amolNo ratings yet
- Ni Elvis ManualDocument98 pagesNi Elvis ManualZhi YiNo ratings yet
- How To Eat WellDocument68 pagesHow To Eat WelleledidiNo ratings yet
- Salem RPGDocument16 pagesSalem RPGabstockingNo ratings yet
- Earth Science (Metamorphic Rocks)Document8 pagesEarth Science (Metamorphic Rocks)MA. ALEXIS LAURENNo ratings yet
- Genie GS-1930 Parts ManualDocument194 pagesGenie GS-1930 Parts ManualNestor Matos GarcíaNo ratings yet
- Sci NB Mod 2 LSN 3Document4 pagesSci NB Mod 2 LSN 3Ramses octavio Rodriguez ocanasNo ratings yet
- Hot Topic 02 Good Light Magazine 56smDocument24 pagesHot Topic 02 Good Light Magazine 56smForos IscNo ratings yet
- Chemical Bonds WorksheetDocument2 pagesChemical Bonds WorksheetJewel Mae MercadoNo ratings yet
- Differential Geometry of Curves and Surfaces 3. Regular SurfacesDocument16 pagesDifferential Geometry of Curves and Surfaces 3. Regular SurfacesyrodroNo ratings yet
- SPM 1449 2006 Mathematics p2 BerjawapanDocument18 pagesSPM 1449 2006 Mathematics p2 Berjawapanpss smk selandar71% (7)
- Method Statement For Cable Trays & Cable Ladders InstallationDocument7 pagesMethod Statement For Cable Trays & Cable Ladders InstallationJamal Budeiri0% (1)
- History of Flash Part - 2Document7 pagesHistory of Flash Part - 2YOGESHWER NATH SINGHNo ratings yet
- Armor MagazineDocument32 pagesArmor Magazine"Rufus"100% (1)
- QuantAssay Software Manual 11-Mar-2019Document51 pagesQuantAssay Software Manual 11-Mar-2019LykasNo ratings yet
- Upaam 1135891 202105060749199700Document18 pagesUpaam 1135891 202105060749199700Kartik KapoorNo ratings yet
- RhythmDocument10 pagesRhythmSalcedo NoelNo ratings yet
- Trawl Master Present A TieDocument19 pagesTrawl Master Present A Tieapi-3719203No ratings yet
- (Eng) Zx890lch 5a Ks En316Document13 pages(Eng) Zx890lch 5a Ks En316MC TAK LEENo ratings yet
- American University of BeirutDocument21 pagesAmerican University of BeirutWomens Program AssosciationNo ratings yet
- SP 73Document105 pagesSP 73Rodrigo Vilanova100% (3)
- Binet Kamat Test For General Mental AbilitiesDocument54 pagesBinet Kamat Test For General Mental AbilitiesSana Siddiq100% (14)
- Dizziness - Vertigo and HomoeopathyDocument38 pagesDizziness - Vertigo and HomoeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- Paranoia XP - Gamemaster Screen Booklet - Mandatory Fun Enforcement PackDocument24 pagesParanoia XP - Gamemaster Screen Booklet - Mandatory Fun Enforcement PackStBash100% (3)
- Illuminati TruthsDocument27 pagesIlluminati TruthsDonnaveo ShermanNo ratings yet
- BTK Implant Guide SurgeryDocument48 pagesBTK Implant Guide SurgeryMaria VolvinaNo ratings yet
- MioPocket ReadmeDocument30 pagesMioPocket Readmelion78No ratings yet
- A Presentation On-: Dr. Nikhil Oza Intern BvdumcDocument43 pagesA Presentation On-: Dr. Nikhil Oza Intern BvdumcMaheboob GanjalNo ratings yet
- Furuno CA 400Document345 pagesFuruno CA 400Димон100% (3)