You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Quick Kingdom 5 e GeneratorDocument8 pagesQuick Kingdom 5 e GeneratorTedTschoppNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- U2 - Boy (Deluxe Edition) Digital BookletDocument11 pagesU2 - Boy (Deluxe Edition) Digital BookletMehmet Akif Delibaş0% (3)
- Tips To Improve Your Freestyle BreathingDocument6 pagesTips To Improve Your Freestyle BreathingreacharunkNo ratings yet
- The Guitar Magazine - April 2019 PDFDocument148 pagesThe Guitar Magazine - April 2019 PDFWassimNo ratings yet
- Grimlite: We Live in A Forgotten World. The Company Brought Peace, Then Left. Only The Doomed and The Lost RemainDocument56 pagesGrimlite: We Live in A Forgotten World. The Company Brought Peace, Then Left. Only The Doomed and The Lost RemainBryan RuheNo ratings yet
- Philippine Folk Dances by Francisca Reyes Aquino PDFDocument2 pagesPhilippine Folk Dances by Francisca Reyes Aquino PDFJoyce EugenioNo ratings yet
- Restaurant Service: Prostart Chapter 4Document14 pagesRestaurant Service: Prostart Chapter 4MALOU ELEVERANo ratings yet
- Funny Sayings Jokes From Funny Sayings CartoonsDocument6 pagesFunny Sayings Jokes From Funny Sayings CartoonsCiuxy_Pink_5530No ratings yet
- Traveller Grammar Beginners KEYDocument6 pagesTraveller Grammar Beginners KEYchuantilly100% (1)
- Bill Statement: Previous Charges Amount (RM) Current Charges Amount (RM)Document11 pagesBill Statement: Previous Charges Amount (RM) Current Charges Amount (RM)Vaishnavi ManoharanNo ratings yet
- Heesu in Class 2 Icons - Google SearchDocument1 pageHeesu in Class 2 Icons - Google SearchNeilisha MaraghNo ratings yet
- Star Magazine USA - February 2023Document52 pagesStar Magazine USA - February 2023Candy EmongNo ratings yet
- Msi b450m Bazooka v2 DatasheetDocument1 pageMsi b450m Bazooka v2 DatasheetPaolo Antonio Díaz AcevedoNo ratings yet
- Genealogy of Major Gods and Goddesses in Greek Mythology Guided Notes Quiz KEYDocument2 pagesGenealogy of Major Gods and Goddesses in Greek Mythology Guided Notes Quiz KEYJE QUESTNo ratings yet
- Nothing Is Impossible SongDocument22 pagesNothing Is Impossible SongPhilip MercadoNo ratings yet
- Retail Institutions by Ownership: Retail Management: A Strategic ApproachDocument18 pagesRetail Institutions by Ownership: Retail Management: A Strategic ApproachVishakhNo ratings yet
- The Story of Us Song AnalysisDocument1 pageThe Story of Us Song AnalysisIgnacio II GarzonNo ratings yet
- Christmas 2014Document1 pageChristmas 2014Roberto PérezNo ratings yet
- Ronelbase 3Document19 pagesRonelbase 3Rafael BernasNo ratings yet
- Cartoon QuizDocument8 pagesCartoon QuizmsaravaNo ratings yet
- OdalDocument1 pageOdaltopurializa02No ratings yet
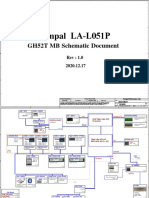
- Compal GH52T LA-L051P Rev 1.0Document121 pagesCompal GH52T LA-L051P Rev 1.0Павел В. (Bis Nival - IrBis Snow)No ratings yet
- Mobility ManagementDocument19 pagesMobility ManagementtanyapahwaNo ratings yet
- Week 11 - Script - Comparative AdjectivesDocument3 pagesWeek 11 - Script - Comparative Adjectivesvaleria marmolejoNo ratings yet
- APUNG GUIDANG MAPEH Daily Lesson LogDocument4 pagesAPUNG GUIDANG MAPEH Daily Lesson LogJeinel Catahan GuiaoNo ratings yet
- Seven Day Meal Plan For A Client With CHFDocument2 pagesSeven Day Meal Plan For A Client With CHFCamille PinedaNo ratings yet
- Academic Reading Test 2Document8 pagesAcademic Reading Test 2Nahoo Asteraye TsigeNo ratings yet
- Bandpass Signals and Complex RepresentationDocument23 pagesBandpass Signals and Complex Representationamitranjan_77No ratings yet
- Concierge Services Booking Form - Airport TransferDocument1 pageConcierge Services Booking Form - Airport TransferAmit DudhaiyaNo ratings yet