You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Lesson 14: Functions and Procedures Performeed by A Laboratory Assistant/Aide Assigned To The Testing AreasDocument32 pagesLesson 14: Functions and Procedures Performeed by A Laboratory Assistant/Aide Assigned To The Testing AreasAngel joyce ValenciaNo ratings yet
- Server Room Guidelines SummaryDocument2 pagesServer Room Guidelines SummaryAnimesh23100% (1)
- Server Room Guidelines SummaryDocument2 pagesServer Room Guidelines SummaryAnimesh23100% (1)
- 2 - Principles of Sterilization.Document76 pages2 - Principles of Sterilization.Mitchelle Sauramba0% (1)
- Basics of sterilization methodsDocument9 pagesBasics of sterilization methodsMohammed YousffiNo ratings yet
- EP05-5.1.1. Methods of Preparation of Sterile ProductsDocument3 pagesEP05-5.1.1. Methods of Preparation of Sterile ProductsatinaprijantonoNo ratings yet
- Cara Membuat Kacamata 3DDocument1 pageCara Membuat Kacamata 3DMakhluk PurbaNo ratings yet
- 2nd Floor Layout FinalDocument1 page2nd Floor Layout FinalAnimesh23No ratings yet
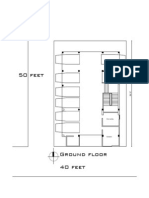
- Ground FloorDocument1 pageGround FloorAnimesh23No ratings yet
- Lift (01) Lift (02) : Detail of Ground Floor Lift Lobby & Reception DetailDocument1 pageLift (01) Lift (02) : Detail of Ground Floor Lift Lobby & Reception DetailAnimesh23No ratings yet
- Ground Floor Presentation Plan: Stair Toilet 6'-1"X3'-11" Toilet 5'-8"X3'-11" Parking ParkingDocument1 pageGround Floor Presentation Plan: Stair Toilet 6'-1"X3'-11" Toilet 5'-8"X3'-11" Parking ParkingAnimesh23No ratings yet
- The Requirements: Means of VentilationDocument6 pagesThe Requirements: Means of VentilationAnimesh23No ratings yet
- The Requirements: Means of VentilationDocument6 pagesThe Requirements: Means of VentilationAnimesh23No ratings yet
- Ad-din Children's Hospital in JessoreDocument4 pagesAd-din Children's Hospital in JessoreAnimesh23No ratings yet
- Remington Chapter 40 SterilizationDocument26 pagesRemington Chapter 40 SterilizationAndhika Bintang Mahardhika50% (2)
- ConMed Looking GlassDocument8 pagesConMed Looking Glasszac rujawitzNo ratings yet
- CSSDDocument16 pagesCSSDuraza.octavoNo ratings yet
- General Information About Chemical Indicators Monitoring Sterilization ProcessesDocument6 pagesGeneral Information About Chemical Indicators Monitoring Sterilization ProcessesVikas DhyaniNo ratings yet
- Residual Formaldehyde On Plastic Materials andDocument4 pagesResidual Formaldehyde On Plastic Materials andsoajaniiNo ratings yet
- Sterilization in DentistryDocument33 pagesSterilization in DentistryShahid HameedNo ratings yet
- Phyto TechniquesDocument13 pagesPhyto TechniquesIsmail JabbarNo ratings yet
- 50HD (220V50HZ) 新款Document14 pages50HD (220V50HZ) 新款thaungmtNo ratings yet
- Setup and User Guide for Steam Quality Test Kit SQ1Document16 pagesSetup and User Guide for Steam Quality Test Kit SQ1schumonNo ratings yet
- Sterilemax ServiceDocument56 pagesSterilemax Servicewmp86110242130% (1)
- 100-Bio - Medical Report 2018 - Final 4Document60 pages100-Bio - Medical Report 2018 - Final 4s k kumarNo ratings yet
- Aptica: Operating ManualDocument32 pagesAptica: Operating ManualAce CanariaNo ratings yet
- SteDis - HospWMDocument68 pagesSteDis - HospWMArvinth Guna SegaranNo ratings yet
- Á1229.1Ñ Steam Sterilization by Direct Contact: 7698 Á1229ñ / General Information USP 41Document4 pagesÁ1229.1Ñ Steam Sterilization by Direct Contact: 7698 Á1229ñ / General Information USP 41Yuli BlandónNo ratings yet
- Akar - AutoclavesDocument8 pagesAkar - AutoclavesprevrtljivacNo ratings yet
- Power Plant Engineering, PK NagDocument18 pagesPower Plant Engineering, PK NagMuket AgmasNo ratings yet
- UG6165 Ibuttom para AutoclaveDocument45 pagesUG6165 Ibuttom para AutoclaveVer OnischNo ratings yet
- Small SterilizerDocument36 pagesSmall Sterilizernotaden1849100% (1)
- 9 - Dental XDocument16 pages9 - Dental XOsama Ben DawNo ratings yet
- Ultradent Gemini User ManualDocument56 pagesUltradent Gemini User Manualpajk fotonaNo ratings yet
- Manual Tanzo TouchDocument55 pagesManual Tanzo TouchEnfant Perdu100% (2)
- Manuais - Autoclave 12L - 300051308 Rev 02Document24 pagesManuais - Autoclave 12L - 300051308 Rev 02Arif HidayatNo ratings yet
- 7.5.9.5.8 Methods of SterilizationDocument3 pages7.5.9.5.8 Methods of SterilizationDedi LihawaNo ratings yet
- Manufacturing FlowDocument12 pagesManufacturing FlowtdeviyanNo ratings yet
- Poleax Plus (N Series) - Catalogue Sturdy Tabletop Autoclave 201807Document6 pagesPoleax Plus (N Series) - Catalogue Sturdy Tabletop Autoclave 201807Xavier MuñozNo ratings yet