You might also like
- AnalgesicDocument62 pagesAnalgesicAnjum IslamNo ratings yet
- Mnemonic SDocument4 pagesMnemonic S1a2b3c4aNo ratings yet
- Mnemonic SDocument41 pagesMnemonic SJane CobicoNo ratings yet
- Megaloblastic AnemiaDocument34 pagesMegaloblastic AnemiaAmir MuhrizNo ratings yet
- Physician Licensure Exam Feb 2010 Top Performing SchoolsDocument2 pagesPhysician Licensure Exam Feb 2010 Top Performing SchoolsSandy Chiong MaganitoNo ratings yet
- PSM Prep LadderDocument43 pagesPSM Prep LadderMayanka SaxenaNo ratings yet
- Jarvis 12 Skin Hair NailsDocument11 pagesJarvis 12 Skin Hair NailsSarah C. SnooksNo ratings yet
- Hematology Oncology Notes Syrian StudentDocument2 pagesHematology Oncology Notes Syrian StudentLoyla RoseNo ratings yet
- Recall QuestionsDocument2 pagesRecall QuestionsAymen BekirNo ratings yet
- High-Impact Outline: Source: Classroom To Clinic Study System by Sedrak and MasseyDocument14 pagesHigh-Impact Outline: Source: Classroom To Clinic Study System by Sedrak and MasseyHannah JosephNo ratings yet
- Benign Paroxysmal Positional VertigoDocument8 pagesBenign Paroxysmal Positional VertigoSubynk RidwanNo ratings yet
- Bhupendra Panchal Lecturer in MSNDocument26 pagesBhupendra Panchal Lecturer in MSNRachel JohnNo ratings yet
- CNS Seizures in ChildhoodDocument42 pagesCNS Seizures in ChildhoodDr.P.NatarajanNo ratings yet
- 1семестр Екзамен на місу іноз нове PDFDocument9 pages1семестр Екзамен на місу іноз нове PDFHart ElettNo ratings yet
- Comprehensive ExaminationDocument36 pagesComprehensive ExaminationZuhair Al Alim AhmedNo ratings yet
- Nclex ReviewDocument5 pagesNclex ReviewOncologynNo ratings yet
- Impactednurse Nurses Reference PackDocument2 pagesImpactednurse Nurses Reference PackRaenell CurryNo ratings yet
- ARISE MEDICAL ACADEMY STUDENTS RECALL RECENT FMGE EXAM QUESTIONSDocument75 pagesARISE MEDICAL ACADEMY STUDENTS RECALL RECENT FMGE EXAM QUESTIONSshimailNo ratings yet
- CTT InsertionDocument18 pagesCTT InsertionRen-Ren NazarenoNo ratings yet
- Principles of BiopsyDocument4 pagesPrinciples of BiopsyTohin TurjoNo ratings yet
- Step 12sem 4Document438 pagesStep 12sem 4opeyemi daramolaNo ratings yet
- Coagulation Disorders-First Aid Book: SS DX TXDocument6 pagesCoagulation Disorders-First Aid Book: SS DX TXMAINo ratings yet
- Skin Pathology Lab Diagnoses and HistologyDocument54 pagesSkin Pathology Lab Diagnoses and HistologyMJO79No ratings yet
- NCLEX MnemonicDocument2 pagesNCLEX MnemonicJem BondocNo ratings yet
- PharmacologyDocument120 pagesPharmacologyFluffy_iceNo ratings yet
- Dermatology - LoveDocument433 pagesDermatology - LoveAntonio EscobarNo ratings yet
- Heart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesDocument3 pagesHeart Failure - Notes From "Cardiology" (Timmis Et Al) : Main CausesPrarthana Thiagarajan100% (3)
- Applications of Leukocyte - and Platelet-Rich Plasma (L-PRP) in TraumaDocument12 pagesApplications of Leukocyte - and Platelet-Rich Plasma (L-PRP) in TraumaEdgar PantojaNo ratings yet
- SplitPDFFile 801 To 1000Document200 pagesSplitPDFFile 801 To 1000Shafan ShajahanNo ratings yet
- Question 1 of 13 on pityriasis rosea diagnosisDocument23 pagesQuestion 1 of 13 on pityriasis rosea diagnosisjonyNo ratings yet
- Fmge De'C. 2017Document21 pagesFmge De'C. 2017Subhodeep MondalNo ratings yet
- By DR - Mohammad Z. Abu Sheikha@: +pigmented Stones (Black Stone - Non Infected) (Brown Stone - Infected)Document11 pagesBy DR - Mohammad Z. Abu Sheikha@: +pigmented Stones (Black Stone - Non Infected) (Brown Stone - Infected)Nisreen Al-shareNo ratings yet
- Clinical Pearls DermatologíamatologyDocument4 pagesClinical Pearls DermatologíamatologyMaritza24No ratings yet
- Haematologic EmergenciesDocument33 pagesHaematologic Emergenciessalmamaged7619No ratings yet
- Marrow Medicine Notes 1 3 6nbsped CompressDocument2 pagesMarrow Medicine Notes 1 3 6nbsped CompressRaam NaikNo ratings yet
- CH 01Document3 pagesCH 01JamieNo ratings yet
- Bipolar Disorder Background: Hypomania Has The Same Symptoms of Mania Without Psychotic SymptomsDocument2 pagesBipolar Disorder Background: Hypomania Has The Same Symptoms of Mania Without Psychotic SymptomshumdingerNo ratings yet
- KNH 413 - Case Study - Type 1 DMDocument14 pagesKNH 413 - Case Study - Type 1 DMapi-301118772No ratings yet
- FMGE June 2019 questions and answersDocument20 pagesFMGE June 2019 questions and answersSugithaTamilarasanNo ratings yet
- AIIMS StrategyDocument12 pagesAIIMS StrategyMahi Reddy100% (1)
- SARP (Skin Anesthesia Radiology Psychiatry) Review 2010Document4 pagesSARP (Skin Anesthesia Radiology Psychiatry) Review 2010QworldNo ratings yet
- Not Mine Survival GuideDocument21 pagesNot Mine Survival GuideJestin AquinoNo ratings yet
- 1 4927329208029413644 PDFDocument578 pages1 4927329208029413644 PDFWaseem UllahNo ratings yet
- Last Hour Review 2020 by Mci Gurukul DR Bhuoendra Armaan Chourasiya PDFDocument49 pagesLast Hour Review 2020 by Mci Gurukul DR Bhuoendra Armaan Chourasiya PDFadiNo ratings yet
- Review of Dermatology Ebook Ebook Alikhan, Ali, Hocker, Thomas L. H Kindle StoreDocument1 pageReview of Dermatology Ebook Ebook Alikhan, Ali, Hocker, Thomas L. H Kindle StoreSally dossNo ratings yet
- GlabellaDocument18 pagesGlabellaghinaNo ratings yet
- EmergencyDocument86 pagesEmergencyyazzNo ratings yet
- Dermatology Review NotesDocument8 pagesDermatology Review Notesnmb1986No ratings yet
- Pulmonary First Aid GuideDocument6 pagesPulmonary First Aid GuideMAINo ratings yet
- PDFDocument570 pagesPDFEshaal FatimaNo ratings yet
- Acute Purulent Diseases of Fingers and HandDocument9 pagesAcute Purulent Diseases of Fingers and Handvem_nikhil4uNo ratings yet
- Anat Recall Que - Dr. AzamDocument24 pagesAnat Recall Que - Dr. AzamSurya VummadisettyNo ratings yet
- Skin Module McqsDocument5 pagesSkin Module McqsSyed Usama Rashid100% (1)
- Treatment of Hemostasis DisordersDocument17 pagesTreatment of Hemostasis DisordersDiana HyltonNo ratings yet
- Aiims PG May 2019Document108 pagesAiims PG May 2019MarcelNo ratings yet
- Mnemonics in DermatologyDocument2 pagesMnemonics in DermatologyShree ShresthaNo ratings yet
- Pharmacology QuestionsDocument20 pagesPharmacology Questionsdelluismanuel100% (2)
- Applied Anatomy - Trigeminal NerveDocument8 pagesApplied Anatomy - Trigeminal NervefrabziNo ratings yet
- MCQsDocument95 pagesMCQsMarcus GrisomNo ratings yet
- Nursing MnemonicsDocument11 pagesNursing MnemonicsMarco CalvaraNo ratings yet
- PRC Form Cmo 14 IrishDocument6 pagesPRC Form Cmo 14 IrishJonathan ObañaNo ratings yet
- Hirschprung DiseaseDocument9 pagesHirschprung DiseaseJonathan ObañaNo ratings yet
- Assessing pedal pulses in patients with hip fracturesDocument5 pagesAssessing pedal pulses in patients with hip fracturesJonathan ObañaNo ratings yet
- Plan of ActivityDocument2 pagesPlan of ActivityJonathan ObañaNo ratings yet
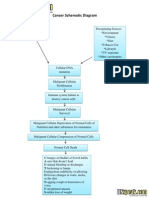
- Cancer Schematic DiagramDocument1 pageCancer Schematic DiagramJonathan ObañaNo ratings yet
- Alkylating AgentsDocument3 pagesAlkylating AgentsJonathan ObañaNo ratings yet
- Statistics and its role in data analysis, interpretation and decision makingDocument1 pageStatistics and its role in data analysis, interpretation and decision makingJonathan ObañaNo ratings yet
- Herniated Nucleus PulposusDocument4 pagesHerniated Nucleus PulposusJonathan ObañaNo ratings yet
- In IvfusionDocument5 pagesIn IvfusionJonathan ObañaNo ratings yet
- Method of Preparation and Systematic Examination of A Direct Fecal SmearDocument3 pagesMethod of Preparation and Systematic Examination of A Direct Fecal SmearCelne CentinoNo ratings yet
- Comparative Study On Hospitality Management Instructors' Teaching Competence and Students' Performance in The Hospitality IndusrtyDocument7 pagesComparative Study On Hospitality Management Instructors' Teaching Competence and Students' Performance in The Hospitality IndusrtyIOER International Multidisciplinary Research Journal ( IIMRJ)No ratings yet
- LKPD ApplicationLetterDocument5 pagesLKPD ApplicationLetterDheaNo ratings yet
- Party Event Planner Services ProposalDocument7 pagesParty Event Planner Services ProposalAnton KenshuseiNo ratings yet
- Prospects and Challenges of Tourism in NepalDocument12 pagesProspects and Challenges of Tourism in NepalShrestha MilanNo ratings yet
- Sp1u C0Document4 pagesSp1u C0Драган РодићNo ratings yet
- Digital Art Syllabus 2015Document3 pagesDigital Art Syllabus 2015api-245305578No ratings yet
- Sample Paper - 2012 Class - XII Subject - Computer Science: InstructionsDocument9 pagesSample Paper - 2012 Class - XII Subject - Computer Science: InstructionsAtif ImamNo ratings yet
- Separation Techniques Virtual LabDocument3 pagesSeparation Techniques Virtual LabRj ReyesNo ratings yet
- Department of Labor: Form WH-516 EnglishDocument1 pageDepartment of Labor: Form WH-516 EnglishUSA_DepartmentOfLabor100% (1)
- KPSC Assistant Professor in CS Question PaperDocument22 pagesKPSC Assistant Professor in CS Question PaperBabaNo ratings yet
- REIT Industry OutlookDocument49 pagesREIT Industry OutlookNicholas FrenchNo ratings yet
- Linear Panel FeaturesDocument12 pagesLinear Panel FeaturesJj ForoNo ratings yet
- OTTO - SMART ROBOT ARCHITECTUREDocument1 pageOTTO - SMART ROBOT ARCHITECTURESuscripcion BelaundeNo ratings yet
- Internship Guidelines MEDocument8 pagesInternship Guidelines MESrinivas SreekantanNo ratings yet
- Batangas CATV Vs CADocument10 pagesBatangas CATV Vs CAMary Joyce Lacambra AquinoNo ratings yet
- Miracle Morning For Writers PDFDocument203 pagesMiracle Morning For Writers PDFIgnacio Bermúdez RothschildNo ratings yet
- Leybold SV40-65BI-FC 1Document29 pagesLeybold SV40-65BI-FC 1Luis LagunaNo ratings yet
- Adhi Wardana 405120042: Blok PenginderaanDocument51 pagesAdhi Wardana 405120042: Blok PenginderaanErwin DiprajaNo ratings yet
- Global FSBDocument68 pagesGlobal FSBJoannaNo ratings yet
- Control Choke Valve 9000Document8 pagesControl Choke Valve 9000sabi_shi100% (2)
- English Learning Kit: Senior High SchoolDocument19 pagesEnglish Learning Kit: Senior High SchoolKare CaspeNo ratings yet
- Vitamins, Minerals Plus Iron, Iodine, Taurine, and Zinc: Nutrition InformationDocument1 pageVitamins, Minerals Plus Iron, Iodine, Taurine, and Zinc: Nutrition InformationWonder PsychNo ratings yet
- MAX3-ONE THERMO-SVC Manual RT43ENSW5 XPEDocument65 pagesMAX3-ONE THERMO-SVC Manual RT43ENSW5 XPECesar Calderon Gr100% (2)
- Dist Relay Test ProcedureDocument7 pagesDist Relay Test ProcedureTamilventhan S100% (1)
- Oliveboard Seaports Airports of India Banking Government Exam Ebook 2017Document8 pagesOliveboard Seaports Airports of India Banking Government Exam Ebook 2017samarjeetNo ratings yet
- Case Study On Barriers To CommunicationDocument3 pagesCase Study On Barriers To CommunicationDivya Gill100% (1)
- 09GMK 6250 - Hydraulikanlage - EnglDocument8 pages09GMK 6250 - Hydraulikanlage - EnglВиталий РогожинскийNo ratings yet
- User Manual Xiaomi Redmi Note 11S (English - 59 Pages)Document3 pagesUser Manual Xiaomi Redmi Note 11S (English - 59 Pages)Abdallah AbdallahNo ratings yet
- WJ9 JDTMFController V5Document41 pagesWJ9 JDTMFController V5commit_to_truthNo ratings yet