You might also like
- Sharan C Patil Bangalore Doctor ListDocument12 pagesSharan C Patil Bangalore Doctor ListNasir AhmedNo ratings yet
- Abhi18 PDFDocument8 pagesAbhi18 PDFNasir AhmedNo ratings yet
- Quotation For Light WeightDocument2 pagesQuotation For Light WeightNasir AhmedNo ratings yet
- FMCG ChaneelDocument4 pagesFMCG ChaneelNasir AhmedNo ratings yet
- VCS BrochureDocument13 pagesVCS BrochureNasir AhmedNo ratings yet
- Allen: Neet-2017 Test Paper With Answer & Solutions (Held On Sunday 07 MAY, 2017)Document7 pagesAllen: Neet-2017 Test Paper With Answer & Solutions (Held On Sunday 07 MAY, 2017)Anurag LaddhaNo ratings yet
- Arabian Consultants Pvt. LTDDocument6 pagesArabian Consultants Pvt. LTDNasir AhmedNo ratings yet
- Abhi18 PDFDocument8 pagesAbhi18 PDFNasir AhmedNo ratings yet
- Loan To Non Member BranchID Dump1001Document250 pagesLoan To Non Member BranchID Dump1001Nasir AhmedNo ratings yet
- PhySICS Paper With AnswerDocument5 pagesPhySICS Paper With Answersudhir_narang_3No ratings yet
- Business Models, Business Strategy and InnovationDocument23 pagesBusiness Models, Business Strategy and InnovationTran Quoc Dong100% (3)
- Joel AbrahamDocument5 pagesJoel AbrahamNasir AhmedNo ratings yet
- Neet Code A Question PaperDocument41 pagesNeet Code A Question PaperRohit Kumar JenaNo ratings yet
- Details of Verified Recruiting AgenciesDocument90 pagesDetails of Verified Recruiting AgenciesNasir AhmedNo ratings yet
- Appointment TableDocument6 pagesAppointment TableNasir AhmedNo ratings yet
- AF21417 - Business Development Manager - Open Day Recruitment - Orient - UAEDocument14 pagesAF21417 - Business Development Manager - Open Day Recruitment - Orient - UAENasir AhmedNo ratings yet
- Dam Maya Magar 509 Sumita Tamang: Hamsa Kalathil Valappil Muhammed Kalathil Valappil Siddique MuhammedDocument1 pageDam Maya Magar 509 Sumita Tamang: Hamsa Kalathil Valappil Muhammed Kalathil Valappil Siddique MuhammedNasir AhmedNo ratings yet
- New Microsoft Word 97 - 2003 DocumentDocument1 pageNew Microsoft Word 97 - 2003 DocumentNasir AhmedNo ratings yet
- PracticeDocument12 pagesPracticeNasir AhmedNo ratings yet
- Civil Engineering Grade BentoniteDocument1 pageCivil Engineering Grade BentoniteNasir AhmedNo ratings yet
- Á Àä Æã/ Æ Gádpàä Àiágà Vàazé À Àgád ºàauàgàv, Àaiàä Àäì: - Gzéæåãuà: Àå Àºágà Á: C Àgázà (©) Vá.F. Uàä® Uáð Àiáqàä À Àæ Àiát Àvàæ J ÉazàgéDocument1 pageÁ Àä Æã/ Æ Gádpàä Àiágà Vàazé À Àgád ºàauàgàv, Àaiàä Àäì: - Gzéæåãuà: Àå Àºágà Á: C Àgázà (©) Vá.F. Uàä® Uáð Àiáqàä À Àæ Àiát Àvàæ J ÉazàgéNasir AhmedNo ratings yet
- Shortcut Key For WindowsDocument2 pagesShortcut Key For WindowsNasir AhmedNo ratings yet
- Social Science EngMQP - 2Document4 pagesSocial Science EngMQP - 2Nasir AhmedNo ratings yet
- Back Page 2Document1 pageBack Page 2Nasir AhmedNo ratings yet
- Online Application For Gazetted Probationers Preliminary Examination - 2014Document2 pagesOnline Application For Gazetted Probationers Preliminary Examination - 2014Nasir AhmedNo ratings yet
- Online Application for Gazetted Probationers Preliminary ExamDocument2 pagesOnline Application for Gazetted Probationers Preliminary ExamNasir AhmedNo ratings yet
- API 13A Sec-4 Grade White Bentonite PriceDocument2 pagesAPI 13A Sec-4 Grade White Bentonite PriceNasir AhmedNo ratings yet
- Income and Caste Certificate: Government of Karnataka Revenue Derpartmet Form-F Gulbarga TalukDocument2 pagesIncome and Caste Certificate: Government of Karnataka Revenue Derpartmet Form-F Gulbarga TalukNasir AhmedNo ratings yet
- IEC OnlineDocument37 pagesIEC OnlinespotdealNo ratings yet
- House For RentDocument1 pageHouse For RentNasir AhmedNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Dissolvine 100-S MSDSDocument8 pagesDissolvine 100-S MSDSMichaelNo ratings yet
- 2018-06-21 Calvert County TimesDocument24 pages2018-06-21 Calvert County TimesSouthern Maryland OnlineNo ratings yet
- Astm C 125-03 PDFDocument4 pagesAstm C 125-03 PDFArnold EspinozaNo ratings yet
- Lesson 5 Investigate Conditions Needed For GerminationDocument12 pagesLesson 5 Investigate Conditions Needed For GerminationJohany Gaona CruzNo ratings yet
- 2219 & 2219 Clad PDFDocument22 pages2219 & 2219 Clad PDF孙俊磊No ratings yet
- UntitledDocument10 pagesUntitledGuia Charish SalvadorNo ratings yet
- 7 Mineral and Soil ResourcesDocument21 pages7 Mineral and Soil ResourcesShardy Lyn RuizNo ratings yet
- Radio WavesDocument17 pagesRadio WavesStuart Yong100% (1)
- ODI AmE L1 ExtraGrammarWkshtDocument30 pagesODI AmE L1 ExtraGrammarWkshtJuan Carlos FlorezNo ratings yet
- Esea Elementary and Secondary Education Act Outline CampionDocument9 pagesEsea Elementary and Secondary Education Act Outline Campionapi-340155293No ratings yet
- Liveability Index 2022Document13 pagesLiveability Index 2022Jigga mannNo ratings yet
- Nursing Management of Patients With DementiaDocument9 pagesNursing Management of Patients With DementiaSabita Paudel60% (5)
- Composite Fish Culture PDFDocument2 pagesComposite Fish Culture PDFHanumant JagtapNo ratings yet
- A Safety Alert Maintenance 1 IADCDocument10 pagesA Safety Alert Maintenance 1 IADCVeeramuthu SundararajuNo ratings yet
- Death Certificate: Shaheed Monsur Ali Medical College HospitalDocument3 pagesDeath Certificate: Shaheed Monsur Ali Medical College HospitalBokul80% (5)
- KeirseyDocument28 pagesKeirseyapi-525703700No ratings yet
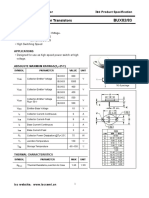
- Isc BUX82/83: Isc Silicon NPN Power TransistorsDocument2 pagesIsc BUX82/83: Isc Silicon NPN Power TransistorsCarlos HCNo ratings yet
- TV Commercials Depicting MothersDocument2 pagesTV Commercials Depicting MothersClarence TumabiaoNo ratings yet
- Engineering Design Guidelines Crude Oil Properties Rev1.2webDocument23 pagesEngineering Design Guidelines Crude Oil Properties Rev1.2webmarco antonioNo ratings yet
- Selected Answer:: 2 Out of 2 PointsDocument15 pagesSelected Answer:: 2 Out of 2 PointsAkansha dwivediNo ratings yet
- Case StudyDocument15 pagesCase StudyGaurav Kumar0% (1)
- Term Paper Envl 4300 Ac 1Document18 pagesTerm Paper Envl 4300 Ac 1api-693796798No ratings yet
- Online Shopping ProjectDocument8 pagesOnline Shopping Projectsrilakshmi itham100% (1)
- Abolish SlaveryDocument1 pageAbolish SlaverySiyeon (Sean) LeeNo ratings yet
- Type I Diabetes Mellitus Management in The Athletic PopulationDocument22 pagesType I Diabetes Mellitus Management in The Athletic PopulationRitesh NetamNo ratings yet
- Mini ProjectDocument16 pagesMini ProjectMr. Y. RajeshNo ratings yet
- Rotex Brochure PDFDocument4 pagesRotex Brochure PDFestramilsolutionNo ratings yet
- Rare Case of Fanconi's Anemia in NewbornDocument3 pagesRare Case of Fanconi's Anemia in NewbornDrJk SinghNo ratings yet
- 10-600000-4200000031-SAM-MEC-CRS-000003 - 01 BEC-WTRAN-270769 WF-114807 Code CDocument4 pages10-600000-4200000031-SAM-MEC-CRS-000003 - 01 BEC-WTRAN-270769 WF-114807 Code Cmohammed rinshinNo ratings yet
- Multi-Criteria Fire / CO Detector Data SheetDocument6 pagesMulti-Criteria Fire / CO Detector Data SheetMazenabs AbsNo ratings yet