You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Scientific Method Worksheets PDFDocument29 pagesScientific Method Worksheets PDFsharmaegayangos83% (6)
- Muscle and Tendon Injuries - Evaluation and Management (2017, Springer-Verlag Berlin Heidelberg)Document440 pagesMuscle and Tendon Injuries - Evaluation and Management (2017, Springer-Verlag Berlin Heidelberg)Joaquin Villagra Jara100% (3)
- Comparative Animal Physiology: A Guide to Thermoregulation and MetabolismDocument7 pagesComparative Animal Physiology: A Guide to Thermoregulation and MetabolismWwwanand111No ratings yet
- What Is HomeoprophylaxisDocument6 pagesWhat Is HomeoprophylaxiswrestlerloverNo ratings yet
- DiscussionDocument16 pagesDiscussionpartha27_pNo ratings yet
- Chapter ParthaDocument8 pagesChapter Parthapartha27_pNo ratings yet
- IntroductionDocument3 pagesIntroductionpartha27_pNo ratings yet
- Breast Cancer and Self AssesmentDocument13 pagesBreast Cancer and Self Assesmentpartha27_pNo ratings yet
- ProverbDocument38 pagesProverbAnkita GoelNo ratings yet
- Environmental Calendar - Special Days - 2023 FinalDocument1 pageEnvironmental Calendar - Special Days - 2023 FinalJohnderek ValenciaNo ratings yet
- Encoded Designs - Hobbs & Friends of The OSR Bonus Issue 1Document20 pagesEncoded Designs - Hobbs & Friends of The OSR Bonus Issue 1Lionel FagoneNo ratings yet
- S9.1 Laboratory Work TextDocument4 pagesS9.1 Laboratory Work TextJennie Jane LobricoNo ratings yet
- Animal Farm / Chapter 8 Reading Organizer Sample AnswersDocument7 pagesAnimal Farm / Chapter 8 Reading Organizer Sample AnswersJacques SnicketNo ratings yet
- Autoimmune ThyroiditisDocument9 pagesAutoimmune ThyroiditisNatarajan NalanthNo ratings yet
- Kids 1 2015 FinalDocument3 pagesKids 1 2015 FinalSilvina HillarNo ratings yet
- Forensic Odontology PDFDocument6 pagesForensic Odontology PDFmoreiraingrid100% (1)
- Active and Passive Voice Exercise: 1. I Did Not Beat HerDocument2 pagesActive and Passive Voice Exercise: 1. I Did Not Beat HerAlex Halliwell67% (3)
- Bali Cattle Breeding SchemeDocument2 pagesBali Cattle Breeding Schemesyaiful48100% (1)
- A Kingdom of Blood and Betrayal - Holly ReneeDocument250 pagesA Kingdom of Blood and Betrayal - Holly ReneeViolet MirzaNo ratings yet
- Test I. Multiple ChoiceDocument3 pagesTest I. Multiple Choicesofieestrada50% (2)
- Science P1 Mid Test 1 & 2Document4 pagesScience P1 Mid Test 1 & 2Stefani PanjaitanNo ratings yet
- I. Multiple Choice. Choose The Letter of The Best AnswerDocument3 pagesI. Multiple Choice. Choose The Letter of The Best AnswerKeannoNo ratings yet
- Perfume SexualDocument286 pagesPerfume Sexualyony100No ratings yet
- Embryology of Urinary SystemDocument4 pagesEmbryology of Urinary SystemZllison Mae Teodoro MangabatNo ratings yet
- Catch PhrasesDocument4 pagesCatch PhrasesVịt PhạmNo ratings yet
- Paket Buffet Umum 2019Document3 pagesPaket Buffet Umum 2019Ikhasul AmalNo ratings yet
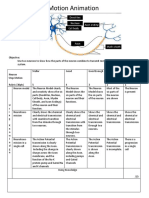
- Neurons Stop Motion AnimationDocument2 pagesNeurons Stop Motion Animationapi-495006167No ratings yet
- Solved CAT 2000 Paper With Solutions PDFDocument80 pagesSolved CAT 2000 Paper With Solutions PDFAravind ShekharNo ratings yet
- Chapter II - Bodies of Fire - The Accupuncture MeridiansDocument41 pagesChapter II - Bodies of Fire - The Accupuncture MeridiansScott Canter100% (1)
- Why We Believe in Creation Not EvolutionDocument242 pagesWhy We Believe in Creation Not EvolutionJoeNo ratings yet
- 0500 - s21 - QP - 13 - May JuneDocument24 pages0500 - s21 - QP - 13 - May Juneelianwar209No ratings yet
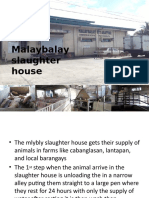
- Ansci 30 Slaughter HouseDocument34 pagesAnsci 30 Slaughter HouseDieanne MaeNo ratings yet
- GanapathyDocument5 pagesGanapathybravindranath5768No ratings yet
- Plane Shift DominariaDocument6 pagesPlane Shift DominariaHercules CosmeNo ratings yet