You might also like
- Basics of How To Read ScansDocument12 pagesBasics of How To Read Scanslexi_2706No ratings yet
- Unit 5 Medical UltrasoundDocument6 pagesUnit 5 Medical Ultrasoundtwy113No ratings yet
- CSF Flowmetry MriDocument5 pagesCSF Flowmetry MribricklaneNo ratings yet
- X-Ray Reveals Skull Lesions in Multiple Myeloma PatientDocument63 pagesX-Ray Reveals Skull Lesions in Multiple Myeloma Patient李建明No ratings yet
- Retrohepatic Gallbladder Masquerading As Hydatid Cyst in ADocument18 pagesRetrohepatic Gallbladder Masquerading As Hydatid Cyst in AMadalina BlagaNo ratings yet
- Liquor CerebrospinalisDocument25 pagesLiquor CerebrospinalisIhda ParidahNo ratings yet
- Clinical Imaging of Liver, Gallbladder, BiliaryDocument93 pagesClinical Imaging of Liver, Gallbladder, Biliaryapi-3856051100% (1)
- Classical Radiological SignsDocument2 pagesClassical Radiological SignsMuntaha JavedNo ratings yet
- Hepatobiliary Disorders: Katrina Saludar Jimenez, R. NDocument42 pagesHepatobiliary Disorders: Katrina Saludar Jimenez, R. NreykatNo ratings yet
- Brain Ventricles AnatomyDocument25 pagesBrain Ventricles AnatomyMiazan SheikhNo ratings yet
- Infertile Couple - Role of Ultrasound FinalDocument31 pagesInfertile Couple - Role of Ultrasound FinalKalpavriksha1974No ratings yet
- The Normal CSFDocument2 pagesThe Normal CSFUm MahmoudNo ratings yet
- DR Kaushal CSF Physiology PresentationDocument39 pagesDR Kaushal CSF Physiology Presentationoddie333No ratings yet
- Fluid CerebrospinalDocument3 pagesFluid CerebrospinalAurelia AlexandraNo ratings yet
- BILIARY TRACT DISEASE: GALLSTONES, CHOLECYSTITIS, CHOLEDOCHOLITHIASIS, AND CHOLANGITISDocument6 pagesBILIARY TRACT DISEASE: GALLSTONES, CHOLECYSTITIS, CHOLEDOCHOLITHIASIS, AND CHOLANGITISRafael KameradNo ratings yet
- CSF and Cerebral Blood FlowDocument58 pagesCSF and Cerebral Blood FlowCindy PrayogoNo ratings yet
- CSFDocument21 pagesCSFjannatin aliya indrinaNo ratings yet
- Cerebrospinal, Pleural and Ascitic Uids: Case 1Document6 pagesCerebrospinal, Pleural and Ascitic Uids: Case 1Amelia PebriantiNo ratings yet
- m2 Bony Anatomy of LegDocument3 pagesm2 Bony Anatomy of LegabidalibpNo ratings yet
- Lower Limb Radiology GuideDocument65 pagesLower Limb Radiology GuideVivien EnriquezNo ratings yet
- Chest X-ray Interpretation Methodical ApproachDocument13 pagesChest X-ray Interpretation Methodical ApproachduncanNo ratings yet
- Molar Pregnancy PDFDocument8 pagesMolar Pregnancy PDFEgaSuharnoNo ratings yet
- 7 PRINCIPLES BREAKTHROUGH THINKINGDocument5 pages7 PRINCIPLES BREAKTHROUGH THINKINGNaysia Kartika100% (1)
- AngiographyDocument17 pagesAngiographyPimsiree MameawNo ratings yet
- Lower Limb: Fig. (1) : A Photoradiograph of A Plain X Ray of The Pelvis (Antero-Posterior View) ShowingDocument8 pagesLower Limb: Fig. (1) : A Photoradiograph of A Plain X Ray of The Pelvis (Antero-Posterior View) ShowingAmany AliNo ratings yet
- Cerebrospinal Fluid: Dr. Anupriya JDocument33 pagesCerebrospinal Fluid: Dr. Anupriya JVivek PatelNo ratings yet
- Ultrasound Și DopplerDocument3 pagesUltrasound Și DopplerAurelia AlexandraNo ratings yet
- Jaundice MasterDocument76 pagesJaundice MasterVinoth KumarNo ratings yet
- Some Techniques of Problem Solving: Work Out The Major Factors InvolvedDocument19 pagesSome Techniques of Problem Solving: Work Out The Major Factors InvolvedRahul M PatilNo ratings yet
- AnatomyDocument94 pagesAnatomypshahNo ratings yet
- Septum Formation in The VentriclesDocument43 pagesSeptum Formation in The VentriclesAhsan IslamNo ratings yet
- Figures Liver and GallbladderDocument32 pagesFigures Liver and GallbladdermarkNo ratings yet
- Liver: Presented by Dr. Tahmina Islam MD Third PartDocument121 pagesLiver: Presented by Dr. Tahmina Islam MD Third PartNajib JamilNo ratings yet
- Bls (Basic Life Support) & Acls (Advanced Care Life Support) : PresenterDocument135 pagesBls (Basic Life Support) & Acls (Advanced Care Life Support) : PresenterbernarduswidodoNo ratings yet
- Ultrasonography of The Hepatobiliary TractDocument9 pagesUltrasonography of The Hepatobiliary TractPaola Méndez NeciosupNo ratings yet
- Cardiovascular Diseases and LiverDocument20 pagesCardiovascular Diseases and LiverKrishna KumarNo ratings yet
- Abdominal US in Hepatobiliary DiseasesDocument76 pagesAbdominal US in Hepatobiliary DiseasesSyafari D. MangopoNo ratings yet
- EVOLUTIONARY BLUNDERSDocument3 pagesEVOLUTIONARY BLUNDERSeustoque2668No ratings yet
- Interventional Radiology & AngiographyDocument45 pagesInterventional Radiology & AngiographyRyBone95No ratings yet
- Cerebrospinal CSFDocument31 pagesCerebrospinal CSFRashid MohamedNo ratings yet
- CXR Interpretation Guide: ABCDE ApproachDocument1 pageCXR Interpretation Guide: ABCDE ApproachValentina SepúlvedaNo ratings yet
- Wave Propogation EffectDocument4 pagesWave Propogation EffectPrashanth ChikkannanavarNo ratings yet
- LiverultrasoundDocument62 pagesLiverultrasoundiuliia94No ratings yet
- Pediatric Echocardiography: Understanding Congenital Heart DefectsDocument159 pagesPediatric Echocardiography: Understanding Congenital Heart DefectsSergiu NiculitaNo ratings yet
- Carotid Stenosis CriteriaDocument50 pagesCarotid Stenosis CriteriafiuliaNo ratings yet
- Classic Radiology SignsDocument9 pagesClassic Radiology SignsJui DirDapNo ratings yet
- Embryology Respiratory System: Formation of Lung BudsDocument1 pageEmbryology Respiratory System: Formation of Lung Budsrezairfan221No ratings yet
- Scrotum Protocol 14Document2 pagesScrotum Protocol 14api-349402240No ratings yet
- Neurovascular SonographyDocument539 pagesNeurovascular SonographyAlexandra MoraesNo ratings yet
- Foldings of Embryo Foetal Period 1Document22 pagesFoldings of Embryo Foetal Period 1Riya SinghNo ratings yet
- High-Resolution Ultrasound in The Assessment of Soft Tissue Tumors and Tumor-Like LesionsDocument41 pagesHigh-Resolution Ultrasound in The Assessment of Soft Tissue Tumors and Tumor-Like LesionsAlvin JulianNo ratings yet
- Normal Variant in Abdominal UltrasounDocument20 pagesNormal Variant in Abdominal Ultrasounshanks spearsonNo ratings yet
- Liver Imaging: MRI with CT CorrelationFrom EverandLiver Imaging: MRI with CT CorrelationErsan AltunNo ratings yet
- Women's Imaging: MRI with Multimodality CorrelationFrom EverandWomen's Imaging: MRI with Multimodality CorrelationMichele A. BrownRating: 5 out of 5 stars5/5 (1)
- P1Document12 pagesP1Roykedona Lisa TrixieNo ratings yet
- Reading A Head CT, What Every EP Should Know PDFDocument62 pagesReading A Head CT, What Every EP Should Know PDFAdistya Sari100% (1)
- CT ScanDocument12 pagesCT ScanNita ThrenitatiaNo ratings yet
- Interpretasi CT ScanDocument19 pagesInterpretasi CT ScanAB KristiadiNo ratings yet
- San 12193Document6 pagesSan 12193Karla BFNo ratings yet
- Wereldleiders Op TwitterDocument24 pagesWereldleiders Op TwitterHerman CouwenberghNo ratings yet
- TRAI Data Till 31st March, 2014Document19 pagesTRAI Data Till 31st March, 2014Tamanna Bavishi ShahNo ratings yet
- Nightingales - Philips Healthcare Tie UpDocument3 pagesNightingales - Philips Healthcare Tie UpSumit RoyNo ratings yet
- The State of Airline Marketing Airlinetrends Simpliflying April2013Document21 pagesThe State of Airline Marketing Airlinetrends Simpliflying April2013Sumit RoyNo ratings yet
- Mobile Advertising Research Trends and InsightsDocument15 pagesMobile Advertising Research Trends and InsightsSumit RoyNo ratings yet
- World Health Days 2014: JanuaryDocument2 pagesWorld Health Days 2014: JanuaryIvy Jorene Roman RodriguezNo ratings yet
- Risk Factors From Hepatitis BCDDocument1 pageRisk Factors From Hepatitis BCDSumit RoyNo ratings yet
- Calendário de Jogos Do Mundial de Futebol-Brasil 2014Document0 pagesCalendário de Jogos Do Mundial de Futebol-Brasil 2014Miguel RodriguesNo ratings yet
- Hepatitis A eDocument1 pageHepatitis A eSumit RoyNo ratings yet
- Hepatitis A eDocument1 pageHepatitis A eSumit RoyNo ratings yet
- NokiaDocument1 pageNokiaSumit RoyNo ratings yet
- The State of Mobile Advertising in Emerging Countries TLS EmergingMarketsDocument8 pagesThe State of Mobile Advertising in Emerging Countries TLS EmergingMarketsSumit RoyNo ratings yet
- MGI China E-Tailing Executive Summary March 2013Document18 pagesMGI China E-Tailing Executive Summary March 2013Sumit RoyNo ratings yet
- Mediamind Comscore Research Dwelling On EntertainmentDocument20 pagesMediamind Comscore Research Dwelling On EntertainmentSumit RoyNo ratings yet
- Global Top 100 Most Valueable Brands Brandz2014 - Infographic PDFDocument1 pageGlobal Top 100 Most Valueable Brands Brandz2014 - Infographic PDFSumit RoyNo ratings yet
- Gender and Social Networking Activity :facebook Vs OthersDocument18 pagesGender and Social Networking Activity :facebook Vs OthersSumit RoyNo ratings yet
- FINAL - Mobile Advertising DeckDocument73 pagesFINAL - Mobile Advertising DecksumitkroyNo ratings yet
- World Health Statisitics FullDocument180 pagesWorld Health Statisitics FullClarice SalidoNo ratings yet
- CEO Survey On Hiring, Profitability and PeopleDocument36 pagesCEO Survey On Hiring, Profitability and PeopleSumit RoyNo ratings yet
- Calendar 14Document57 pagesCalendar 14Hanan AhmedNo ratings yet
- The 5 Free Alternatives To Microsoft WordDocument60 pagesThe 5 Free Alternatives To Microsoft WordSumit RoyNo ratings yet
- The State of Maternal Health, D Nutrition in Asia " World Vision DataDocument4 pagesThe State of Maternal Health, D Nutrition in Asia " World Vision DataSumit RoyNo ratings yet
- 2014 Bill and Melinda Gates Foundation Report On Global PovertyDocument28 pages2014 Bill and Melinda Gates Foundation Report On Global PovertySumit RoyNo ratings yet
- The 5 Free Alternatives To Microsoft WordDocument60 pagesThe 5 Free Alternatives To Microsoft WordSumit RoyNo ratings yet
- CVD Atlas 16 Death From Stroke PDFDocument1 pageCVD Atlas 16 Death From Stroke PDFRisti KhafidahNo ratings yet
- 10 Historical Speeches Nobody Ever HeardDocument20 pages10 Historical Speeches Nobody Ever HeardSumit Roy100% (1)
- India InfographicsDocument3 pagesIndia InfographicsSumit RoyNo ratings yet
- The Evolution of Digital Advertising 3.0: Adobe Research InsightsDocument1 pageThe Evolution of Digital Advertising 3.0: Adobe Research InsightsSumit RoyNo ratings yet
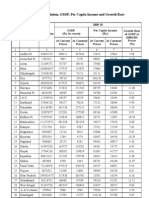
- Statewise GSDP PCI and G.RDocument3 pagesStatewise GSDP PCI and G.RArchit SingalNo ratings yet