You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Four Common Types of Parenting StylesDocument11 pagesThe Four Common Types of Parenting StylesIka_Dyah_Purwa_1972100% (3)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Power of The Mind 2010 PDFDocument32 pagesPower of The Mind 2010 PDFTijana Morača Aćimović100% (3)
- Mothership Zine Rulebook v5 PDFDocument44 pagesMothership Zine Rulebook v5 PDFAna Luiza FernandesNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 2012 Mirror Therapy For Improving Motor Function After StrokeDocument68 pages2012 Mirror Therapy For Improving Motor Function After StrokeMarcelo Ortiz Valenzuela100% (1)
- Iso 27001 PDFDocument7 pagesIso 27001 PDFMonica MoreiraNo ratings yet
- Business Studies 2012 HSC With AnswerDocument33 pagesBusiness Studies 2012 HSC With AnswerPSiloveyou490% (1)
- Fuji FCR 5000Document435 pagesFuji FCR 5000Lion Micheal OtitolaiyeNo ratings yet
- Article 2194Document9 pagesArticle 2194anhiramdhani100% (1)
- Upstream Marine Standard IBU ChevronDocument52 pagesUpstream Marine Standard IBU ChevronAndrew Hendy Indrakusuma50% (2)
- 02 TBS Lightning Protection System PDFDocument448 pages02 TBS Lightning Protection System PDFgilbertomjcNo ratings yet
- 02 Laboratory Experiment 1Document2 pages02 Laboratory Experiment 1J Paradise100% (1)
- Atlas CopcoDocument58 pagesAtlas CopcoMario Maldonado100% (3)
- Safety Health & Environment MethodologyDocument14 pagesSafety Health & Environment MethodologymusengemNo ratings yet
- Toussaint 2007Document11 pagesToussaint 2007Marcelo Ortiz ValenzuelaNo ratings yet
- 2019 Polución de Aire y Enfermedades No Comunicables Parte 2Document10 pages2019 Polución de Aire y Enfermedades No Comunicables Parte 2Marcelo Ortiz ValenzuelaNo ratings yet
- Nevus BeckerDocument7 pagesNevus BeckerMarcelo Ortiz ValenzuelaNo ratings yet
- United States Patent: (45) Date of Patent: Sep - 8, 2020Document14 pagesUnited States Patent: (45) Date of Patent: Sep - 8, 2020M FNo ratings yet
- Intec Controls SPC31195 DatasheetDocument5 pagesIntec Controls SPC31195 DatasheetEduardo CalvaNo ratings yet
- Horizontal and Vertical Dis AllowanceDocument12 pagesHorizontal and Vertical Dis Allowancesuhaspujari93No ratings yet
- Hcs CatalogueDocument16 pagesHcs CatalogueG MuratiNo ratings yet
- WEEK 4 - Q2 - Earth and LifeDocument16 pagesWEEK 4 - Q2 - Earth and Lifenoreen lubindinoNo ratings yet
- A Strategic Behaviour Guidance Tool in Paediatric Dentistry: 'Reframing' - An ExperienceDocument3 pagesA Strategic Behaviour Guidance Tool in Paediatric Dentistry: 'Reframing' - An Experiencesilky groverNo ratings yet
- Checklist of Eligibility Requirements For Consulting ServicesDocument2 pagesChecklist of Eligibility Requirements For Consulting ServicesAndrea BroccoliNo ratings yet
- Testing and Commissioning Procedure: 2017 EDITIONDocument242 pagesTesting and Commissioning Procedure: 2017 EDITIONvin ssNo ratings yet
- PETRODETAILSDocument2 pagesPETRODETAILSAlexanderNo ratings yet
- Epsom Salt ClassDocument7 pagesEpsom Salt ClassSofia marisa fernandesNo ratings yet
- Sociology Review QuestionsDocument6 pagesSociology Review QuestionsNIYONSHUTI VIATEURNo ratings yet
- CVP MonitoringDocument10 pagesCVP MonitoringRaghu RajanNo ratings yet
- Q2-PPT-PE10-Module1.2 (Running As Exercise)Document30 pagesQ2-PPT-PE10-Module1.2 (Running As Exercise)Gericho MarianoNo ratings yet
- Road To Sustainable SHG-Bank Linkage Programme: Formulating Strategies For Managing Credit Risk With Respect To Rural BengalDocument6 pagesRoad To Sustainable SHG-Bank Linkage Programme: Formulating Strategies For Managing Credit Risk With Respect To Rural BengalAnimesh TiwariNo ratings yet
- Quarterly Test - Q3 English 9Document6 pagesQuarterly Test - Q3 English 9Rodrigl BaiganNo ratings yet
- Bechtel - Use of Startup StrainerDocument17 pagesBechtel - Use of Startup Strainerreach_arindomNo ratings yet
- 3rd Edition 60601 1web VersionDocument44 pages3rd Edition 60601 1web VersionMario H. RodríguezNo ratings yet
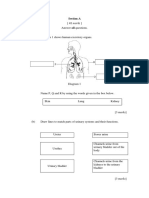
- Section A: Jawab Semua SoalanDocument3 pagesSection A: Jawab Semua SoalanAzreen IzetNo ratings yet