You might also like
- Acog Practice Bulletin: Thromboembolism in PregnancyDocument17 pagesAcog Practice Bulletin: Thromboembolism in PregnancytriNo ratings yet
- Abortion KuliahDocument38 pagesAbortion KuliahElsa Hasibuan100% (1)
- Gyn & ObsDocument68 pagesGyn & ObsEsraa AlmassriNo ratings yet
- Pop, RevDocument139 pagesPop, RevYusof AndreiNo ratings yet
- Minimally Invasive Versus Abdominal Radical HysterectomyDocument10 pagesMinimally Invasive Versus Abdominal Radical HysterectomyClinton Franda Markus SitanggangNo ratings yet
- Dopplerinpregnancy 130823082426 Phpapp02Document64 pagesDopplerinpregnancy 130823082426 Phpapp02Herry SasukeNo ratings yet
- (Advanced Trauma Life Support) Moderator: Dr. Deepak S: Ganesh Kumar VIII TermDocument20 pages(Advanced Trauma Life Support) Moderator: Dr. Deepak S: Ganesh Kumar VIII Termabhaymalur100% (1)
- Management of Benign Breast Conditions: Part 2 - Breast Lumps and LesionsDocument3 pagesManagement of Benign Breast Conditions: Part 2 - Breast Lumps and Lesionspeter_mrNo ratings yet
- Vaginal Vault ProlapseDocument9 pagesVaginal Vault ProlapseOanaNo ratings yet
- Obs Sakshi Arora, E 9 ReducedDocument536 pagesObs Sakshi Arora, E 9 ReducedAman PareekNo ratings yet
- Difficulties in Vaginal HysterctomyDocument66 pagesDifficulties in Vaginal HysterctomyManamita NiphadkarNo ratings yet
- BronchosDocument17 pagesBronchosravigadaniNo ratings yet
- Evaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusDocument7 pagesEvaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusGabyliz Gonzalez CastilloNo ratings yet
- Toprank Review Pediatric Nursing NotesDocument12 pagesToprank Review Pediatric Nursing NotesCose online shopNo ratings yet
- PA Genitalia WanitaDocument100 pagesPA Genitalia WanitaBNo ratings yet
- Singer and Monaghan's Cervical and Lower Genital Tract Precancer: Diagnosis and TreatmentFrom EverandSinger and Monaghan's Cervical and Lower Genital Tract Precancer: Diagnosis and TreatmentRating: 5 out of 5 stars5/5 (1)
- Ambulatory HysterosDocument8 pagesAmbulatory Hysteroskomlanihou_890233161100% (1)
- Mullarian AnomoliesDocument85 pagesMullarian AnomoliesPrathibha GuruguriNo ratings yet
- C SectionDocument50 pagesC SectionAlano S. LimgasNo ratings yet
- The Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachDocument8 pagesThe Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachqisthiaufaNo ratings yet
- Libro Medicina Reproductiva 2022Document645 pagesLibro Medicina Reproductiva 2022Luisa Moreno100% (1)
- 2019 - Bowel and Bladder Injury Repair and Follow-Up After Gynecologic Surgery - 00006250-201902000-00012Document10 pages2019 - Bowel and Bladder Injury Repair and Follow-Up After Gynecologic Surgery - 00006250-201902000-00012Polyana FloresNo ratings yet
- Clarks Essential Guide To Clinical UltrasoundDocument77 pagesClarks Essential Guide To Clinical Ultrasoundrobertlinon0% (1)
- The Diagnosis and Management of The Acute Abdomen in Pregnancy-Greenspan, Peter, Springer Verlag (2017)Document284 pagesThe Diagnosis and Management of The Acute Abdomen in Pregnancy-Greenspan, Peter, Springer Verlag (2017)AndreaAlexandraNo ratings yet
- Basic Investigation of An Infertile CoupleDocument53 pagesBasic Investigation of An Infertile CoupleRemelou Garchitorena AlfelorNo ratings yet
- CPG - Management of Breast Cancer (2nd Edition)Document100 pagesCPG - Management of Breast Cancer (2nd Edition)umiraihana1No ratings yet
- The Management of Asherman Syndrome: A Review of LiteratureDocument11 pagesThe Management of Asherman Syndrome: A Review of LiteratureEuphra Adellheid100% (1)
- Healthcare StatisticsDocument20 pagesHealthcare StatisticsAnonymous ibmeej9No ratings yet
- Laparoscopic Gynecologist Surgeon in HSR Layout BangaloreDocument8 pagesLaparoscopic Gynecologist Surgeon in HSR Layout BangaloreDr.Beena JeysinghNo ratings yet
- WeBSurg Winners 42 1Document129 pagesWeBSurg Winners 42 1Ana Adam100% (1)
- TOG Vaginal HysterectomyDocument6 pagesTOG Vaginal HysterectomyYasmin AlkhatibNo ratings yet
- MRCOG Module SummaryDocument4 pagesMRCOG Module SummaryAmadeus KQNo ratings yet
- Training in Obstetrics and Gynaecology - Ippokratis SarrisDocument4 pagesTraining in Obstetrics and Gynaecology - Ippokratis Sarriszuxifoho0% (1)
- 62 Colposcopy StandardsDocument73 pages62 Colposcopy Standardsrijal mahdiy pNo ratings yet
- 8surgical Management of Dysfunctional Uterine Bleeding - KabilanDocument14 pages8surgical Management of Dysfunctional Uterine Bleeding - KabilanNavani TharanNo ratings yet
- 2015 Oncology CREOG Review PDFDocument76 pages2015 Oncology CREOG Review PDFRima HajjarNo ratings yet
- Ruptur OASISDocument41 pagesRuptur OASISHen DriNo ratings yet
- Acog Practice Bulletin Summary: Pregestational Diabetes MellitusDocument3 pagesAcog Practice Bulletin Summary: Pregestational Diabetes MellitusMaría Fernanda Palma AcostaNo ratings yet
- Handbook of Obstetric MedicineDocument15 pagesHandbook of Obstetric MedicineSara Zoi Lu50% (2)
- Craniofacial AbnormalitiesDocument12 pagesCraniofacial Abnormalitiesnpr00No ratings yet
- Dystocia and Augmentation of LAbor PDFDocument10 pagesDystocia and Augmentation of LAbor PDFKathleenNo ratings yet
- E-Poster Rcog 2018Document1 pageE-Poster Rcog 2018Ana MarianaNo ratings yet
- ACOG On CA EndometriumDocument14 pagesACOG On CA EndometriumzoviNo ratings yet
- E. Prior Phenotypically Normal Infant Delivered at 34 Weeks Due To Spontaneous Preterm LaborDocument10 pagesE. Prior Phenotypically Normal Infant Delivered at 34 Weeks Due To Spontaneous Preterm LaborSK ASIF ALINo ratings yet
- Tuberculosis in Obstetrics and GynecologyDocument42 pagesTuberculosis in Obstetrics and GynecologyameenNo ratings yet
- O&G - Abnormal PresentationDocument32 pagesO&G - Abnormal PresentationAnironOrionNo ratings yet
- Idea of OSCE in Obstetric.4012829.Powerpoint 1Document19 pagesIdea of OSCE in Obstetric.4012829.Powerpoint 1Aitzaz AhmedNo ratings yet
- 2023 OB/GYN Coding Manual: Components of Correct CodingFrom Everand2023 OB/GYN Coding Manual: Components of Correct CodingNo ratings yet
- Obstetrics and Gynecology Sixth Edition Obstetrics and Gynecology Beckman Chapter 36Document8 pagesObstetrics and Gynecology Sixth Edition Obstetrics and Gynecology Beckman Chapter 363hondoNo ratings yet
- Ultrasound - A GuideDocument9 pagesUltrasound - A GuideDebasish KunduNo ratings yet
- Pop QDocument45 pagesPop QObgyn Maret2016No ratings yet
- Ad en Om Yo SisDocument6 pagesAd en Om Yo SisMariaa EndahhNo ratings yet
- FIGO Clasificación HUA 2011Document11 pagesFIGO Clasificación HUA 2011dickenskevinNo ratings yet
- Presented by DR - Shahbaz Ahmad Professor of Community MedicineDocument76 pagesPresented by DR - Shahbaz Ahmad Professor of Community MedicinePriya bhattiNo ratings yet
- ACOG Practice Bulletin No 99 Management of 39 PDFDocument26 pagesACOG Practice Bulletin No 99 Management of 39 PDFhkdawnwongNo ratings yet
- Stats For CreogDocument1 pageStats For CreogzareeneyNo ratings yet
- 2022 Mendoza Eligibility CriteriaDocument21 pages2022 Mendoza Eligibility CriteriaТатьяна ТутченкоNo ratings yet
- IUGA Scoring SystemDocument40 pagesIUGA Scoring SystemBudi Iman SantosoNo ratings yet
- Treatment of Acute Endometritis. Medication and DosesDocument3 pagesTreatment of Acute Endometritis. Medication and DosesTitoun LettounNo ratings yet
- Creog Urogyn ReviewDocument97 pagesCreog Urogyn ReviewAlexandriah AlasNo ratings yet
- Abdul Malik Hassim Lecturer DMA Management & Science UniversityDocument21 pagesAbdul Malik Hassim Lecturer DMA Management & Science UniversitykimmgizelleNo ratings yet
- Fetal Medicine - Bidyut KumarDocument4 pagesFetal Medicine - Bidyut KumarpatoxyzuNo ratings yet
- Handbook of Current and Novel Protocols for the Treatment of InfertilityFrom EverandHandbook of Current and Novel Protocols for the Treatment of InfertilityMichael H. DahanNo ratings yet
- Clinical Impact and Biomaterial Evaluation of Platelet Gel in Cardiac Surgery Gunaydin 2008Document8 pagesClinical Impact and Biomaterial Evaluation of Platelet Gel in Cardiac Surgery Gunaydin 2008api-222634056No ratings yet
- Dhillon PRP Knee OsteoarthritisDocument9 pagesDhillon PRP Knee Osteoarthritisapi-222634056No ratings yet
- Orthopedic PRPDocument27 pagesOrthopedic PRPapi-222634056No ratings yet
- Tang - Antimicrobial Peptides From Human Platelets - 2002Document11 pagesTang - Antimicrobial Peptides From Human Platelets - 2002api-222634056No ratings yet
- J Orthopaedic Research Involvement of Platelets in StimulatDocument9 pagesJ Orthopaedic Research Involvement of Platelets in Stimulatapi-222634056No ratings yet
- Platelet Gel As An Intraoperative Procured Platelet Based AlDocument2 pagesPlatelet Gel As An Intraoperative Procured Platelet Based Alapi-222634056No ratings yet
- PRP For Dental Implants and Soft Tissue Grafting - GargDocument8 pagesPRP For Dental Implants and Soft Tissue Grafting - Gargapi-222634056No ratings yet
- Case Series - Use of PRP in Bariatric Surgery - BradyDocument4 pagesCase Series - Use of PRP in Bariatric Surgery - Bradyapi-222634056No ratings yet
- PRP in Coronary Artery Bypass Grafting-Effects On Surgical Wound Healing - VangDocument8 pagesPRP in Coronary Artery Bypass Grafting-Effects On Surgical Wound Healing - Vangapi-222634056No ratings yet
- Use of PRP in Cosmetic Surgery - ManDocument11 pagesUse of PRP in Cosmetic Surgery - Manapi-222634056No ratings yet
- PRP To Promote Healing in Abdominoplasty - JacksonDocument10 pagesPRP To Promote Healing in Abdominoplasty - Jacksonapi-222634056No ratings yet
- Ehancing Wound Healing With Growth Factors - AdlerDocument18 pagesEhancing Wound Healing With Growth Factors - Adlerapi-222634056No ratings yet
- PRP To Promote Healing in Abdominoplasty - JacksonDocument10 pagesPRP To Promote Healing in Abdominoplasty - Jacksonapi-222634056No ratings yet
- Pilot Study - Use of Platelet Gel To Treat Nonhelaing WoundDocument6 pagesPilot Study - Use of Platelet Gel To Treat Nonhelaing Woundapi-222634056No ratings yet
- Platelet Gel For Endoscopic Sinus Surgery - PomerantzDocument7 pagesPlatelet Gel For Endoscopic Sinus Surgery - Pomerantzapi-222634056No ratings yet
- Cost Effectiveness of PRP For Diabetic Foot Ulcers Dougherty 2008Document8 pagesCost Effectiveness of PRP For Diabetic Foot Ulcers Dougherty 2008api-222634056No ratings yet
- Use of PRP and Its Effects On Infection in Cardiac Surgery - StammersDocument6 pagesUse of PRP and Its Effects On Infection in Cardiac Surgery - Stammersapi-222634056No ratings yet
- Platelet Gel Final Protocol BWHDocument7 pagesPlatelet Gel Final Protocol BWHapi-222634056No ratings yet
- Osu Paper 120005Document2 pagesOsu Paper 120005api-222634056No ratings yet
- Efficacy of PRP in Pain Control and Blood Loss in Tka - GardnerDocument5 pagesEfficacy of PRP in Pain Control and Blood Loss in Tka - Gardnerapi-222634056No ratings yet
- Platelet Gel Final Protocol BWHDocument7 pagesPlatelet Gel Final Protocol BWHapi-222634056No ratings yet
- Laparoscopic SurgeryDocument4 pagesLaparoscopic SurgerycaioaccorsiNo ratings yet
- Phinma Cagayan de Oro CollegeDocument14 pagesPhinma Cagayan de Oro CollegeYasmin MagsaysayNo ratings yet
- Diagnosis and Managment of Gaynecologic CancersDocument1,067 pagesDiagnosis and Managment of Gaynecologic CancersarisNo ratings yet
- Lasers and Lights e Book Procedures in Cosmetic Dermatology Series 4th Edition Ebook PDFDocument58 pagesLasers and Lights e Book Procedures in Cosmetic Dermatology Series 4th Edition Ebook PDFlouis.starks790100% (46)
- Normal Tissue Tolerance Master 11-2016Document15 pagesNormal Tissue Tolerance Master 11-2016Virgilio Rafael Tovar VasquezNo ratings yet
- Evd Evd Evd Evd Accudrain Accudrain Accudrain Accudrain: External Ventricular DeviceDocument1 pageEvd Evd Evd Evd Accudrain Accudrain Accudrain Accudrain: External Ventricular DeviceQueenNo ratings yet
- A Global TextBook of Radiology IIDocument705 pagesA Global TextBook of Radiology IIannatabashidzeNo ratings yet
- BronchosDocument3 pagesBronchosNAENAENo ratings yet
- Renal FailureDocument60 pagesRenal Failuredr_shamimrNo ratings yet
- Label The Circulatory SystemDocument2 pagesLabel The Circulatory SystemIzzu PenielNo ratings yet
- Erich Arch Bar Versus Hanger Plate Technique For Intermaxillary Fixation in Fracture MandibleDocument6 pagesErich Arch Bar Versus Hanger Plate Technique For Intermaxillary Fixation in Fracture MandibleAndrés Faúndez TeránNo ratings yet
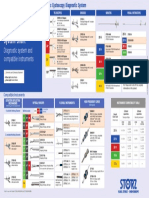
- Karl Storz Cystoscope System Chart: Diagnostic System and Compatible InstrumentsDocument1 pageKarl Storz Cystoscope System Chart: Diagnostic System and Compatible InstrumentsRaydoon SadeqNo ratings yet
- RicaDocument9 pagesRicarica mae narbaizNo ratings yet
- Ophthalmic Viscosurgical Devices: DR A Debata DrsrpatiDocument48 pagesOphthalmic Viscosurgical Devices: DR A Debata Drsrpatidrsrp84No ratings yet
- SCAI SHOCK Bedside Checklist 2022Document1 pageSCAI SHOCK Bedside Checklist 2022Katherine AzocarNo ratings yet
- Medical BookletDocument35 pagesMedical BookletNesanNo ratings yet
- An Ovarian Granulosa Cell Tumor in A Patient With Polycystic Ovarian Syndrome: A Case ReportDocument5 pagesAn Ovarian Granulosa Cell Tumor in A Patient With Polycystic Ovarian Syndrome: A Case ReportIJAR JOURNALNo ratings yet
- Knee Next Generation in Repair and Reconstruction 2022Document118 pagesKnee Next Generation in Repair and Reconstruction 2022Jose SantiagoNo ratings yet
- Epi Zone Articles 1Document8 pagesEpi Zone Articles 1kai xinNo ratings yet
- Preparation For Children and Their Families: Voiding Cystourethrogram (VCUG)Document2 pagesPreparation For Children and Their Families: Voiding Cystourethrogram (VCUG)NataliaMaedyNo ratings yet
- Wound Healing: Healing by First Intention (Primary Union)Document31 pagesWound Healing: Healing by First Intention (Primary Union)Muhammad Masoom AkhtarNo ratings yet
- PDD Instrument Set Brochure 001 V1-En 20000101Document16 pagesPDD Instrument Set Brochure 001 V1-En 20000101javixojdnNo ratings yet
- ANPH M3 CU11. Urinary SystemDocument13 pagesANPH M3 CU11. Urinary Systemmia LoremiaNo ratings yet
- CAOS Final ExamDocument34 pagesCAOS Final ExamNaimenur KorkmazNo ratings yet
- What Is A Retained Placenta?Document4 pagesWhat Is A Retained Placenta?Baharudin Yusuf Ramadhani0% (1)