You might also like
- Fifa Soccer PDFDocument52 pagesFifa Soccer PDFMahdicheraghiNo ratings yet
- Strength Mahdi Cheraghi 2018Document45 pagesStrength Mahdi Cheraghi 2018Mahdicheraghi100% (1)
- HypertrophyDocument36 pagesHypertrophyMahdicheraghiNo ratings yet
- 45 06 Skill Xfer Cands PDFDocument4 pages45 06 Skill Xfer Cands PDFMahdicheraghiNo ratings yet
- Anterior Cruciate Ligament Injuries in Soccer Players:: Amit Bandyopadhyay and Shazlin ShaharudinDocument15 pagesAnterior Cruciate Ligament Injuries in Soccer Players:: Amit Bandyopadhyay and Shazlin ShaharudinmanhuiyNo ratings yet
- Weightlifting Pulling Derivatives: Rationale For Implementation and ApplicationDocument18 pagesWeightlifting Pulling Derivatives: Rationale For Implementation and ApplicationMahdicheraghiNo ratings yet
- Complex Training Reexamined: Review and Recommendations To Improve Strength and PowerDocument10 pagesComplex Training Reexamined: Review and Recommendations To Improve Strength and PowerMahdicheraghiNo ratings yet
- Changes in The Eccentric Phase Contribute To Improved Stretch-Shorten Cycle Performance After Training"Cormie Et Al. 2010 - Changes in ECC PhaseDocument15 pagesChanges in The Eccentric Phase Contribute To Improved Stretch-Shorten Cycle Performance After Training"Cormie Et Al. 2010 - Changes in ECC PhaseMahdicheraghiNo ratings yet
- Central and Peripheral Fatigue During Resistance Exercise - A Critical ReviewDocument12 pagesCentral and Peripheral Fatigue During Resistance Exercise - A Critical ReviewMahdicheraghiNo ratings yet
- Load Absorption Force-Time Characteristics Following The Second Pull of Weightlifting DerivativesDocument10 pagesLoad Absorption Force-Time Characteristics Following The Second Pull of Weightlifting DerivativesMahdicheraghiNo ratings yet
- Prevention of Injury and Overuse in Sports-2016Document178 pagesPrevention of Injury and Overuse in Sports-2016Mahdicheraghi100% (1)
- The Scoop and Second PullDocument4 pagesThe Scoop and Second Pullapi-79367840No ratings yet
- The Benefits of Vitamin CDocument4 pagesThe Benefits of Vitamin CMahdicheraghiNo ratings yet
- JumpSquat-Power Impact of LoadDocument10 pagesJumpSquat-Power Impact of LoadMahdicheraghiNo ratings yet
- Boxing 3D KinematicsDocument12 pagesBoxing 3D KinematicsMahdicheraghiNo ratings yet
- Youth Training NSCADocument10 pagesYouth Training NSCAJermaine RobertsonNo ratings yet
- Functional Performance Testing of ACL LigamentDocument15 pagesFunctional Performance Testing of ACL LigamentMahdicheraghiNo ratings yet
- Early Acceleration KinematicsDocument7 pagesEarly Acceleration KinematicsMahdicheraghiNo ratings yet
- Overview of Factor AnalysisDocument16 pagesOverview of Factor AnalysisKush GuptaNo ratings yet
- Is Postexercise Muscle Soreness A Valid Indicator.2Document6 pagesIs Postexercise Muscle Soreness A Valid Indicator.2MahdicheraghiNo ratings yet
- Biomechanics in Sports 29Document4 pagesBiomechanics in Sports 29MahdicheraghiNo ratings yet
- ACL Kinematic BasisDocument5 pagesACL Kinematic BasisMahdicheraghiNo ratings yet
- Exploratory Factor Analysis Kootstra 04Document15 pagesExploratory Factor Analysis Kootstra 04Vi KekaNo ratings yet
- Simple Guidelines Development FlexibilityDocument3 pagesSimple Guidelines Development FlexibilityMahdicheraghiNo ratings yet
- Analisis Entre Mov. Comun y Hab Del FutbolDocument8 pagesAnalisis Entre Mov. Comun y Hab Del FutbolRocío Yañez VerdugoNo ratings yet
- Brief Review Maximizing HypertrophyDocument8 pagesBrief Review Maximizing HypertrophyMahdicheraghiNo ratings yet
- Analisis Entre Mov. Comun y Hab Del FutbolDocument8 pagesAnalisis Entre Mov. Comun y Hab Del FutbolRocío Yañez VerdugoNo ratings yet
- Balance TrainingDocument12 pagesBalance TrainingMahdicheraghi100% (1)
- Youth Training NSCADocument10 pagesYouth Training NSCAJermaine RobertsonNo ratings yet
- Effects of Plyometrics Before SquatDocument4 pagesEffects of Plyometrics Before SquatMahdicheraghiNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 18-02-4 Farmacologie MG 3RO AfisatDocument11 pages18-02-4 Farmacologie MG 3RO AfisatElena IftimiNo ratings yet
- Brochure PDFDocument6 pagesBrochure PDFMotortrade Tayug SalesNo ratings yet
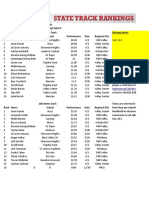
- 5A Boys Track Rankings: April 7, 2021Document44 pages5A Boys Track Rankings: April 7, 2021Catch it KansasNo ratings yet
- Project Cosco KirthiDocument64 pagesProject Cosco KirthiAnonymous ar6Upyf8No ratings yet
- Hilton Head Relocation GuideDocument50 pagesHilton Head Relocation GuidebernardhhiNo ratings yet
- Pico Corporate BrochureDocument55 pagesPico Corporate BrochureDaniel BarrenecheaNo ratings yet
- The Pershing Cable (Feb 1981)Document2 pagesThe Pershing Cable (Feb 1981)Ed PalmerNo ratings yet
- Wendler 5/3/1 SpreadsheetDocument38 pagesWendler 5/3/1 SpreadsheetkanoxNo ratings yet
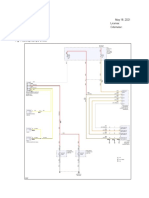
- Exterior Lights: Ymms: May 18, 2021 Engine: 3.3L Eng License: Vin: Odometer: 2017 Kia Sorento SXDocument4 pagesExterior Lights: Ymms: May 18, 2021 Engine: 3.3L Eng License: Vin: Odometer: 2017 Kia Sorento SXAndre VPNo ratings yet
- CBSE Syllabus For Class 11 Physical Education 2022-23 (Revised) PDF DownloadDocument4 pagesCBSE Syllabus For Class 11 Physical Education 2022-23 (Revised) PDF Downloadavik mukherjee100% (1)
- Group 3 Lab Report - Muscle 2Document33 pagesGroup 3 Lab Report - Muscle 2Chippy RabeNo ratings yet
- A4 Detailed Lesson Plan ChessDocument8 pagesA4 Detailed Lesson Plan ChessMark Dhen Sarmiento IINo ratings yet
- Latihan JedaDocument9 pagesLatihan JedaRizal MaslahNo ratings yet
- Google Doc Explains Linear Weights Stat for Baseball WARDocument27 pagesGoogle Doc Explains Linear Weights Stat for Baseball WARAndres AlvaradoNo ratings yet
- Tips For Riding A Successful Dressage TestDocument4 pagesTips For Riding A Successful Dressage TestJorn DoeNo ratings yet
- NO Nama Nopol Type No - TLP Srvs Sblmnya: Daftar Reminder Bulan April 2013Document10 pagesNO Nama Nopol Type No - TLP Srvs Sblmnya: Daftar Reminder Bulan April 2013Anton YuliNo ratings yet
- Effect of Social Media On Interactivity Between English Premier League Football Clubs and Fans in EnglandDocument17 pagesEffect of Social Media On Interactivity Between English Premier League Football Clubs and Fans in EnglandJonah nyachaeNo ratings yet
- Harken Catalog 2012Document229 pagesHarken Catalog 2012Renato FonsecaNo ratings yet
- The Boxer and The Blonde Are TogetherDocument81 pagesThe Boxer and The Blonde Are TogetherThảoUyênNo ratings yet
- McDonald - SO. 1 E4 A Reliable Repertoire For The Improving Player (2006)Document201 pagesMcDonald - SO. 1 E4 A Reliable Repertoire For The Improving Player (2006)bani100100% (8)
- Physical Education XiDocument59 pagesPhysical Education XiAkshitNo ratings yet
- Ferrari 458 ItaliaDocument13 pagesFerrari 458 ItaliaBikram PrajapatiNo ratings yet
- Cor Van Wijgerden - Learning Chess - Manual Step 6 (2011)Document198 pagesCor Van Wijgerden - Learning Chess - Manual Step 6 (2011)Red Rex 2015No ratings yet
- Deadly Hung Gar Techniques RevealedDocument22 pagesDeadly Hung Gar Techniques Revealedbrendan lanzaNo ratings yet
- Press Kit Norway-SpainDocument18 pagesPress Kit Norway-Spainjannep17No ratings yet
- 4th ICA All India Open FIDE Rating Rapid Chess TournamentDocument3 pages4th ICA All India Open FIDE Rating Rapid Chess TournamentARJUN NARAYANAN 21BAS10008No ratings yet
- California Dreaming: Arranged by Michael ChapdelaineDocument5 pagesCalifornia Dreaming: Arranged by Michael ChapdelaineJoss Armand0% (1)
- HISTORY OF BADMINTONDocument18 pagesHISTORY OF BADMINTONAngeline SumaoyNo ratings yet
- A Guide To Chess EndingsDocument252 pagesA Guide To Chess EndingsSamuel DabinNo ratings yet
- 16-Week Powerlifting Block Periodization ProgramDocument6 pages16-Week Powerlifting Block Periodization ProgramAgustin GregorettiNo ratings yet