You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- CH 49 MedsurgDocument18 pagesCH 49 MedsurgJiezl Abellano AfinidadNo ratings yet
- Liver Function Tests and How To Relate ThemDocument82 pagesLiver Function Tests and How To Relate ThemG VenkateshNo ratings yet
- Chronic Liver Diseases & PLCCDocument56 pagesChronic Liver Diseases & PLCCibnbasheer100% (5)
- Biliary StrictureDocument27 pagesBiliary StrictureMohammad Nazar100% (2)
- Hepatobiliary System-Anatomy & PhysiologyDocument49 pagesHepatobiliary System-Anatomy & PhysiologyDeshi SportsNo ratings yet
- Gallstone DiseaseDocument104 pagesGallstone DiseaseTan DanNo ratings yet
- 2.3 - LIVER Patho - ARBDocument73 pages2.3 - LIVER Patho - ARBCRUZ Jill EraNo ratings yet
- Chole Lithia Sis Path oDocument6 pagesChole Lithia Sis Path ogeloNo ratings yet
- Cholecystitis With CholecystolithiasisDocument33 pagesCholecystitis With CholecystolithiasisDino V EscalonaNo ratings yet
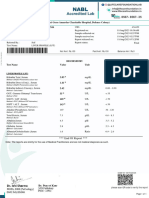
- Lab Report NewDocument2 pagesLab Report Newmohitsharma.jalNo ratings yet
- Liver Fibrosis ProgressDocument9 pagesLiver Fibrosis ProgressTaufik Rizkian AsirNo ratings yet
- Liver Function TestsDocument26 pagesLiver Function TestsSadeq TalibNo ratings yet
- Metabolisme Bilirubin: - Biosintesis Heme Dan Porphyrias - Metabolisme Bilirubin: Ikterus: JaundiceDocument32 pagesMetabolisme Bilirubin: - Biosintesis Heme Dan Porphyrias - Metabolisme Bilirubin: Ikterus: JaundiceTutde SedanaNo ratings yet
- Jaundice: From Superstition To ScienceDocument93 pagesJaundice: From Superstition To ScienceDr Muhammad ShoyabNo ratings yet
- Tratamiento Médico de Los Pólipos Vesiculares. Estudio PilotoDocument3 pagesTratamiento Médico de Los Pólipos Vesiculares. Estudio Pilotomeche1989No ratings yet
- OSCE Case Practice 1: Pathology Station Marking Schemes: Well Done Partially Done Not DoneDocument5 pagesOSCE Case Practice 1: Pathology Station Marking Schemes: Well Done Partially Done Not DoneIsaac OngNo ratings yet
- Cat Aliza Mehbin BioDocument1 pageCat Aliza Mehbin BioKirti DoshiNo ratings yet
- A Case Presentation On CholedocholithiasisDocument11 pagesA Case Presentation On CholedocholithiasisPaul Vincent EspereNo ratings yet
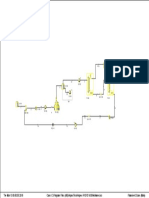
- PFD VCM (Vinyl Chloride Monomer)Document1 pagePFD VCM (Vinyl Chloride Monomer)Muhammad Hadi SaputraNo ratings yet
- Liver Transplantation: Diseases Suitable For TransplantationDocument2 pagesLiver Transplantation: Diseases Suitable For TransplantationgeorgedejeuNo ratings yet
- Clinicalmanifestationsand Treatmentofdrug-Induced HepatotoxicityDocument9 pagesClinicalmanifestationsand Treatmentofdrug-Induced HepatotoxicityChâu Khắc ToànNo ratings yet
- Surgical JaundiceDocument35 pagesSurgical JaundiceIbsa ShumaNo ratings yet
- 2 PBDocument7 pages2 PBAnggraeni Indri SilviantiNo ratings yet
- Team Pedro LanderlanDocument3 pagesTeam Pedro Landerlanapi-307594401No ratings yet
- Curs 15v-2018hDocument96 pagesCurs 15v-2018hMirceaDraghiciNo ratings yet
- Viral Hepatitis Tests PDFDocument7 pagesViral Hepatitis Tests PDFHussein N. FarhatNo ratings yet
- Grading and Staging Systems For Inflammation and Fibrosis in Chronic Liver DiseasesDocument10 pagesGrading and Staging Systems For Inflammation and Fibrosis in Chronic Liver DiseasesPD18No ratings yet
- Liver Funection TestDocument33 pagesLiver Funection TestDjdjjd SiisusNo ratings yet
- Obs JauDocument22 pagesObs JauRavi GuptaNo ratings yet
- Choledocal CystDocument11 pagesCholedocal CystBilly JonatanNo ratings yet