You might also like
- Material SelectionDocument1 pageMaterial SelectionmuhammadsaliNo ratings yet
- Prolapsed DiscDocument10 pagesProlapsed DiscmuhammadsaliNo ratings yet
- Material SelectionDocument1 pageMaterial SelectionmuhammadsaliNo ratings yet
- Cold Drawn Seamless For Heat Exchangers and BoilersDocument12 pagesCold Drawn Seamless For Heat Exchangers and BoilersmuhammadsaliNo ratings yet
- Base Plate and Anchor Bolt DesignDocument7 pagesBase Plate and Anchor Bolt DesignmuhammadsaliNo ratings yet
- Transformation of StressesDocument13 pagesTransformation of StressesmuhammadsaliNo ratings yet
- ASMESectionVIIIDivision1 WeldNeckFlangeCalcDocument15 pagesASMESectionVIIIDivision1 WeldNeckFlangeCalcmuhammadsaliNo ratings yet
- Structural Design Loads CalculationDocument6 pagesStructural Design Loads Calculationfaris11No ratings yet
- How To Extract PetroleumDocument16 pagesHow To Extract PetroleummuhammadsaliNo ratings yet
- Piping Stress BendingDocument5 pagesPiping Stress BendingGeorgeNo ratings yet
- Uplift With Moment CalculationDocument4 pagesUplift With Moment CalculationdennykvgNo ratings yet
- ASCE 7-2010 LoadCombsDocument1 pageASCE 7-2010 LoadCombsmuhammadsaliNo ratings yet
- Mumps FactsDocument8 pagesMumps FactsmuhammadsaliNo ratings yet
- Electrical Equipment in Hazardous AreasDocument19 pagesElectrical Equipment in Hazardous AreasmuhammadsaliNo ratings yet
- Quality Assurance in Banking ServicesDocument2 pagesQuality Assurance in Banking ServicesmuhammadsaliNo ratings yet
- Shell and Tube Heat ExchangerDocument1 pageShell and Tube Heat ExchangermuhammadsaliNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Acute Bronchitis Care Study 202Document25 pagesAcute Bronchitis Care Study 202Kara Kathrina FuentesNo ratings yet
- Causes of Mortality and MorbidityDocument8 pagesCauses of Mortality and MorbiditypurletpunkNo ratings yet
- Case Study: Acute BronchitisDocument34 pagesCase Study: Acute BronchitisJeffany Anne Rabaya Retirado0% (1)
- Bronchitis Home RemediesDocument2 pagesBronchitis Home RemediesTimar2100% (1)
- Nursing InterventionsDocument10 pagesNursing Interventionspaulinian_nurseNo ratings yet
- COPD and Asthma: Causes, Symptoms, Diagnosis and TreatmentDocument138 pagesCOPD and Asthma: Causes, Symptoms, Diagnosis and TreatmentMonique Reyes0% (1)
- Meaning of Different Types of SputumDocument10 pagesMeaning of Different Types of SputumCharlotte's WebNo ratings yet
- Pharma - M1L1 - Rational Drug PrescribingDocument6 pagesPharma - M1L1 - Rational Drug PrescribingEric Meynard SanchezNo ratings yet
- Efficacy and Tolerability of A Fluid Extract Combination of Thyme Herb and Ivy Leaves and Matched Placebo in Adults Suffering From Acute Bronchitis With Productive Cough PDFDocument9 pagesEfficacy and Tolerability of A Fluid Extract Combination of Thyme Herb and Ivy Leaves and Matched Placebo in Adults Suffering From Acute Bronchitis With Productive Cough PDFvitor_chenNo ratings yet
- Comprehensive Case StudyDocument8 pagesComprehensive Case Studyapi-634419348No ratings yet
- Treatment of Acute BronchitisDocument3 pagesTreatment of Acute Bronchitisrisma panjaitanNo ratings yet
- 12 STEM C - CASIÑO - Assignment 2.3.1Document5 pages12 STEM C - CASIÑO - Assignment 2.3.1CASIÑO SHANE VAST ANDREINo ratings yet
- Clinical Case Study Presentation - MJDocument37 pagesClinical Case Study Presentation - MJapi-365372933No ratings yet
- Respiratory Disorder Note BSC 3rd YearDocument41 pagesRespiratory Disorder Note BSC 3rd YearNancyNo ratings yet
- Duijvestijn Et Al-2009-Cochrane Database of Systematic ReviewsDocument37 pagesDuijvestijn Et Al-2009-Cochrane Database of Systematic ReviewsNeerajNo ratings yet
- TestBank Lewis Medical Surgical Nursing 11th 2020.pdf-282-305Document24 pagesTestBank Lewis Medical Surgical Nursing 11th 2020.pdf-282-305هدوء النسمةNo ratings yet
- Pneumonia Bronkitis Buat CoassDocument14 pagesPneumonia Bronkitis Buat CoassdrakeironquistNo ratings yet
- Case Study: Acute BronchitisDocument28 pagesCase Study: Acute BronchitisMarco AlabanzaNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleReyhan AdityaaNo ratings yet
- Respiratory System: D) Dullness With A Tympanic ShadeDocument31 pagesRespiratory System: D) Dullness With A Tympanic Shademohammad farooque razaaNo ratings yet
- Pediatrics-Case Presentation: - Sumanga, Juan Cheska Eunice ADocument62 pagesPediatrics-Case Presentation: - Sumanga, Juan Cheska Eunice ALhio Tuguegarao PcbNo ratings yet
- What Is EmphysemaDocument8 pagesWhat Is EmphysemaHadibah MokhtarNo ratings yet
- Referral to Orthopaedic Surgeon for Knee Cartilage SurgeryDocument18 pagesReferral to Orthopaedic Surgeon for Knee Cartilage SurgeryTINU THOMAS THOMASNo ratings yet
- BronchitisDocument11 pagesBronchitisRenuka Sivaram100% (2)
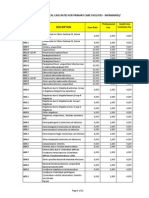
- PhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesDocument22 pagesPhilHealth Circular No. 0035, s.2013 Annex 5 List of Medical Case Rates For Primary Care FacilitiesChrysanthus HerreraNo ratings yet
- Treatment of Acute BronchitisDocument3 pagesTreatment of Acute BronchitissemaraNo ratings yet
- Case Study 5 Year Boy With CoughDocument3 pagesCase Study 5 Year Boy With CoughAryl Eduarte100% (1)
- Acute Bronchitis: Clinical PearlDocument9 pagesAcute Bronchitis: Clinical PearlLauraNo ratings yet
- Wheezing, Bronchiolitis, and BronchitisDocument12 pagesWheezing, Bronchiolitis, and BronchitisMuhd AzamNo ratings yet
- Bronchitis Vs BronchiolitisDocument52 pagesBronchitis Vs BronchiolitisUngku Hajar Nur AthirahNo ratings yet