You might also like
- Coagulase Test Guide: Detecting S. aureusDocument2 pagesCoagulase Test Guide: Detecting S. aureusilyas9558No ratings yet
- UnivResJDent33108-2026554 053745Document5 pagesUnivResJDent33108-2026554 053745ilyas9558No ratings yet
- Understanding IVF and the Ethical Questions it RaisesDocument4 pagesUnderstanding IVF and the Ethical Questions it Raisesilyas9558No ratings yet
- Future of Industrial MicrobiologyDocument7 pagesFuture of Industrial Microbiologyilyas9558No ratings yet
- Embryo Transfer CattleDocument3 pagesEmbryo Transfer Cattleilyas9558No ratings yet
- Monoclonal AntibodiesDocument6 pagesMonoclonal Antibodiesilyas9558No ratings yet
- Cri du chat Syndrome Signs, Causes & ResearchDocument1 pageCri du chat Syndrome Signs, Causes & Researchilyas9558No ratings yet
- Virus Classification: Retroviridae LentivirusDocument12 pagesVirus Classification: Retroviridae Lentivirusilyas9558No ratings yet
- Cri Du ChatDocument5 pagesCri Du ChatIlyas Khan AurakzaiNo ratings yet
- AbadiDocument14 pagesAbadiilyas9558No ratings yet
- RSVDocument8 pagesRSVilyas9558No ratings yet
- Jerusalemsyn HTMLDocument14 pagesJerusalemsyn HTMLilyas9558No ratings yet
- Embryo Transfer CattleDocument3 pagesEmbryo Transfer Cattleilyas9558No ratings yet
- BandingDocument3 pagesBandingilyas9558No ratings yet
- Acute Coronary Syndromes: Robert Smith August 4, 2003Document37 pagesAcute Coronary Syndromes: Robert Smith August 4, 2003ilyas9558No ratings yet
- How To Install and Use A Whole House FanDocument4 pagesHow To Install and Use A Whole House Fanilyas9558No ratings yet
- Charcot-Marie-Tooth DiseaseDocument9 pagesCharcot-Marie-Tooth Diseaseilyas9558No ratings yet
- 1145 FullDocument6 pages1145 Fullilyas9558No ratings yet
- X XXXXXXXXXXXXXXDocument22 pagesX XXXXXXXXXXXXXXilyas9558No ratings yet
- Acute Coronary Syndromes: Robert Smith August 4, 2003Document37 pagesAcute Coronary Syndromes: Robert Smith August 4, 2003ilyas9558No ratings yet
- J. Biol. Chem.-2001-Gampala-9855-60Document6 pagesJ. Biol. Chem.-2001-Gampala-9855-60ilyas9558No ratings yet
- New Microsoft Word DocumentDocument4 pagesNew Microsoft Word Documentilyas9558No ratings yet
- PCRDocument1 pagePCRIlyas Khan AurakzaiNo ratings yet
- AbadiDocument14 pagesAbadiilyas9558No ratings yet
- DNA SequencingDocument3 pagesDNA SequencingIlyas Khan AurakzaiNo ratings yet
- Fan Source BookDocument92 pagesFan Source Bookapi-3808778100% (10)
- Green TeaDocument60 pagesGreen Teailyas9558No ratings yet
- Tentative Date Sheet For BA-BSc Composite 1st Annual Examination 2013Document3 pagesTentative Date Sheet For BA-BSc Composite 1st Annual Examination 2013ilyas9558No ratings yet
- How To Install and Use A Whole House FanDocument4 pagesHow To Install and Use A Whole House Fanilyas9558No ratings yet
- BABScDocument2 pagesBABScSyed Jawad AliNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
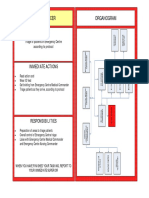
- Triage Officer Organogram: MissionDocument14 pagesTriage Officer Organogram: Missionsnow fazliNo ratings yet
- STELLA Edited 4-1Document41 pagesSTELLA Edited 4-1Okwany JimmyNo ratings yet
- Pharmaceutical reference booksDocument25 pagesPharmaceutical reference booksSubhan RullyansyahNo ratings yet
- Legal Aspects of Perioperative NursingDocument9 pagesLegal Aspects of Perioperative NursingZerrie lei Hart100% (2)
- PDAG BDocument20 pagesPDAG Bskyweb 888No ratings yet
- Hmis Monitoring and Evaluation: Emil Gatus Student Number Name of SchoolDocument20 pagesHmis Monitoring and Evaluation: Emil Gatus Student Number Name of SchoolNowair TuanNo ratings yet
- Start - Jump START Triage PDFDocument2 pagesStart - Jump START Triage PDF081381246529100% (1)
- Plan 2 ND YearODocument8 pagesPlan 2 ND YearOSamuel InbarajaNo ratings yet
- Asanthe Case WorkingsDocument9 pagesAsanthe Case Workingsazhar hussainNo ratings yet
- RPRH Accomplishment Report 1stsem2022Document9 pagesRPRH Accomplishment Report 1stsem2022Rose Martinez BayNo ratings yet
- Open Letter To ICE From Medical Professionals Re COVID-19Document68 pagesOpen Letter To ICE From Medical Professionals Re COVID-19Jesus Garcia0% (1)
- Three Years After My Complaint, Kelly Fink Brogan MD Surrenders Her New York State Medical LicenseDocument16 pagesThree Years After My Complaint, Kelly Fink Brogan MD Surrenders Her New York State Medical LicensePeter M. HeimlichNo ratings yet
- RubyDocument13 pagesRubyNamoAmitofouNo ratings yet
- Guidelines For Case Report IPDDocument3 pagesGuidelines For Case Report IPDMohd TempahanNo ratings yet
- Artigo Remoção Cirúrgica de Neoplasa em PeixeDocument7 pagesArtigo Remoção Cirúrgica de Neoplasa em Peixecursotplo2021No ratings yet
- D Pharm RegulationsDocument11 pagesD Pharm Regulations16_dev5038No ratings yet
- Dental Career PathsDocument4 pagesDental Career Pathsrd8No ratings yet
- Adj 12563Document5 pagesAdj 12563anushiNo ratings yet
- Small But Intriguing The Unfolding Story of Homeopathic Medicine PDFDocument7 pagesSmall But Intriguing The Unfolding Story of Homeopathic Medicine PDFweb3351No ratings yet
- PHARMA Sep 08 1-15Document8 pagesPHARMA Sep 08 1-15medigistNo ratings yet
- Introduction To SOAP NotesDocument23 pagesIntroduction To SOAP Notestsaokw83% (6)
- Marketing PresentationDocument13 pagesMarketing PresentationMamun Rashid0% (1)
- Abc BSN 4y1-1 Week 9 Course TaskDocument1 pageAbc BSN 4y1-1 Week 9 Course TaskHannah BalunanNo ratings yet
- Breathe. Exhale. Repeat - The Benefits of Controlled BreathingDocument3 pagesBreathe. Exhale. Repeat - The Benefits of Controlled BreathingDaxten KienNo ratings yet
- NCMB317 RUBRICS Mental Status ExaminationDocument1 pageNCMB317 RUBRICS Mental Status Examinationkpbalay5921pamNo ratings yet
- MPT Musculoskeletal Physiotherapy-Smt Kashibai Navale College of Physiotherapy, Pune - Admission-Details - 20230925204502Document3 pagesMPT Musculoskeletal Physiotherapy-Smt Kashibai Navale College of Physiotherapy, Pune - Admission-Details - 20230925204502hindjai66No ratings yet
- Hand Hygiene Action Plan - Final Draft For IPCGDocument10 pagesHand Hygiene Action Plan - Final Draft For IPCGAnton NaingNo ratings yet
- Homeopathy and PainDocument9 pagesHomeopathy and Painoana777No ratings yet
- AAP Algorithm in Neonatal Hypoglycemia PDFDocument4 pagesAAP Algorithm in Neonatal Hypoglycemia PDFmefav7778520No ratings yet
- DSM 5 Update 2015 PDFDocument30 pagesDSM 5 Update 2015 PDFFlo RenceNo ratings yet