You might also like
- Have Half-Lives in The Range 2 - 6 H. Lovenox Is 4.5 Hours. The Anticoagulant Effect ofDocument37 pagesHave Half-Lives in The Range 2 - 6 H. Lovenox Is 4.5 Hours. The Anticoagulant Effect ofkellixgNo ratings yet
- CHAPTER 12: Leukocyte Development Kinetics, and FunctionsDocument7 pagesCHAPTER 12: Leukocyte Development Kinetics, and FunctionsPrimo GeorgeNo ratings yet
- Abdominal AbscessDocument3 pagesAbdominal AbscessIchalAzNo ratings yet
- Abdominal Trauma: Fatin Amirah KamaruddinDocument29 pagesAbdominal Trauma: Fatin Amirah Kamaruddinvirz23No ratings yet
- Manage HypoglycemiaDocument57 pagesManage HypoglycemiaAmelia PricopNo ratings yet
- Fluids and Electrolytes Management in Surgical PatientsDocument4 pagesFluids and Electrolytes Management in Surgical PatientsJanine Maita BalicaoNo ratings yet
- Hypertension and Angina DrugsDocument158 pagesHypertension and Angina DrugsMelissa SalayogNo ratings yet
- Epithelial TissueDocument7 pagesEpithelial TissueJoan PaulineNo ratings yet
- Metabolic response to injuryDocument5 pagesMetabolic response to injuryZllison Mae Teodoro Mangabat100% (1)
- Anes Preoperative-AssessmentDocument6 pagesAnes Preoperative-AssessmentChristine Mendoza100% (1)
- Pharmacology of EthanolDocument5 pagesPharmacology of EthanolJoshua RemonNo ratings yet
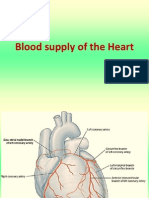
- Blood Supply of HeartDocument7 pagesBlood Supply of Heartmariposa_0612No ratings yet
- Shock (For Surgery)Document50 pagesShock (For Surgery)Emmanuel Rojith VazNo ratings yet
- Carcinoma of The Breast - Bailey & LoveDocument5 pagesCarcinoma of The Breast - Bailey & LoveKeyshia Yazid100% (1)
- USMLE Step 2 Lesson on Thyroid DiseaseDocument4 pagesUSMLE Step 2 Lesson on Thyroid DiseaseMavra zNo ratings yet
- Lecture 2-Introduction To MicroscopesDocument26 pagesLecture 2-Introduction To MicroscopesThuto SmithNo ratings yet
- Cardiovascular Physiology 4 - Gomez MD PDFDocument65 pagesCardiovascular Physiology 4 - Gomez MD PDFMelissa SalayogNo ratings yet
- JaundiceDocument53 pagesJaundiceAbhishiktaAbhiNo ratings yet
- Endo 3 Notes PDFDocument9 pagesEndo 3 Notes PDFDilNo ratings yet
- Immunity To MicrobesDocument65 pagesImmunity To Microbesmulatumelese100% (1)
- Pharmacology of Insulin and Oral Hypoglycaemic DrugsDocument27 pagesPharmacology of Insulin and Oral Hypoglycaemic Drugsdepren0% (1)
- Breast CancerDocument6 pagesBreast Cancersarguss14No ratings yet
- Understanding Liver Tests and DiseasesDocument65 pagesUnderstanding Liver Tests and DiseasesDokter MuhammadNo ratings yet
- Approach To Pleura LeffusionDocument91 pagesApproach To Pleura Leffusionrodie1050% (1)
- UrinalysisDocument9 pagesUrinalysisSukma EffendyNo ratings yet
- Examining The PrecordiumDocument83 pagesExamining The PrecordiumnicolNo ratings yet
- Lab Physiology Second Year PracticalDocument21 pagesLab Physiology Second Year PracticalNona NonicaaNo ratings yet
- Metabolic Response To InjuryDocument55 pagesMetabolic Response To InjuryMuhammad NaveedNo ratings yet
- Endocrine ChartDocument28 pagesEndocrine ChartNiki NikolićNo ratings yet
- Histology of Male Reproductive SystemDocument3 pagesHistology of Male Reproductive SystemSanna Asila AkramNo ratings yet
- Treatment of Hemostasis DisordersDocument17 pagesTreatment of Hemostasis DisordersDiana HyltonNo ratings yet
- Adrenal Hyperfunction: Cushing'S SyndromeDocument10 pagesAdrenal Hyperfunction: Cushing'S SyndromeJoaquim RodriguezNo ratings yet
- Surgical Anatomy of The Chest Wall, Pleura, and MediastinumDocument8 pagesSurgical Anatomy of The Chest Wall, Pleura, and MediastinumNooneNo ratings yet
- Metabolic Response to Trauma: Understanding the Physiological ConsequencesDocument52 pagesMetabolic Response to Trauma: Understanding the Physiological ConsequencesAnil BasnetNo ratings yet
- 2018 Overview Digestive System HandoutDocument11 pages2018 Overview Digestive System HandoutdraganNo ratings yet
- Pathophysiology Cell Injury GuideDocument7 pagesPathophysiology Cell Injury GuideWendy SuhNo ratings yet
- Hypoglycemia: Prepared By: Ahmed Rawhi DabourDocument84 pagesHypoglycemia: Prepared By: Ahmed Rawhi DabourKaterina FusaNo ratings yet
- Differential White Blood Cell CountDocument20 pagesDifferential White Blood Cell CountNada hasan100% (2)
- Acid-Base - Ppt-How To ReadDocument22 pagesAcid-Base - Ppt-How To ReadnursaidahNo ratings yet
- Physiologic MonitoringDocument4 pagesPhysiologic MonitoringAimie DagaleaNo ratings yet
- Lecture 7 ThermoregulationDocument30 pagesLecture 7 ThermoregulationLouella Artates100% (1)
- Liver Function Tests (Sem)Document6 pagesLiver Function Tests (Sem)Francisco NiegasNo ratings yet
- Lymph NodeDocument13 pagesLymph NodeNurul Ilma AllauwNo ratings yet
- 2-60-1 - Colon Cancer TreatmentDocument1 page2-60-1 - Colon Cancer Treatmentlyocco1No ratings yet
- Endocrine Disorders 1234399857677955 1Document130 pagesEndocrine Disorders 1234399857677955 1api-19824701No ratings yet
- Anticoagulants 161120143945Document29 pagesAnticoagulants 161120143945Roshan SahuNo ratings yet
- Evaluation of Abdominal PainDocument7 pagesEvaluation of Abdominal PainCherry Faith Merisco LabtangNo ratings yet
- Surgical Anatomy of the Stomach and DuodenumDocument75 pagesSurgical Anatomy of the Stomach and DuodenumMohamoud MohamedNo ratings yet
- ENDOCRINE PATHOLOGY WebpathDocument35 pagesENDOCRINE PATHOLOGY Webpathapi-3766657No ratings yet
- Neutrophils: in Health and DiseaseDocument65 pagesNeutrophils: in Health and DiseaseKush Pathak100% (1)
- NUTRITION LECTURE NOTES ON FAT-SOLUBLE AND WATER-SOLUBLE VITAMINSDocument5 pagesNUTRITION LECTURE NOTES ON FAT-SOLUBLE AND WATER-SOLUBLE VITAMINSfallenNo ratings yet
- LeukemiaDocument26 pagesLeukemiaochamocha100% (1)
- Interpretation of CBCDocument35 pagesInterpretation of CBCnth1992No ratings yet
- AlcoholsDocument23 pagesAlcoholsdhaineyNo ratings yet
- ShockDocument21 pagesShockMin-Joo Esther ParkNo ratings yet
- Protozoan Parasites Causing Malaria, Sleeping Sickness, Leishmaniasis and MoreDocument32 pagesProtozoan Parasites Causing Malaria, Sleeping Sickness, Leishmaniasis and MoreFort SalvadorNo ratings yet
- Antibiotics CompiledDocument30 pagesAntibiotics CompiledJoanne Chu100% (1)
- C - VVV VV VVVV VVV - VVV VV - VVVV VV VVDocument3 pagesC - VVV VV VVVV VVV - VVV VV - VVVV VV VVBea Angela Bithao AnonoyNo ratings yet
- Surgical MetabolismDocument12 pagesSurgical Metabolismjc_sibal13No ratings yet
- Initial Assessment & ManagementDocument3 pagesInitial Assessment & Managementjc_sibal13No ratings yet
- Nutrition AssignmentDocument2 pagesNutrition Assignmentapi-3720272No ratings yet
- Basic Life SupportDocument3 pagesBasic Life Supportjc_sibal13No ratings yet
- Basic Life SupportDocument1 pageBasic Life SupportMahmoud Hamad ElneelNo ratings yet
- ShockDocument3 pagesShockjc_sibal13No ratings yet
- Surgical Pediatric and Elderly PatientsDocument1 pageSurgical Pediatric and Elderly Patientsjc_sibal13No ratings yet
- Surgical InfectionsDocument2 pagesSurgical Infectionsjc_sibal13100% (1)
- Initial Assessment and Management Initial Assessment and ManagementDocument6 pagesInitial Assessment and Management Initial Assessment and Managementjc_sibal13No ratings yet
- TraumaDocument2 pagesTraumajc_sibal13No ratings yet
- Pediatric and Elderly Patients in SurgeryDocument4 pagesPediatric and Elderly Patients in Surgeryjc_sibal13No ratings yet
- Surgical Antimicrobial Prophylaxis PDFDocument10 pagesSurgical Antimicrobial Prophylaxis PDFPatrick JohnNo ratings yet
- Fluids and ElectrolytesDocument16 pagesFluids and Electrolytesjc_sibal13No ratings yet
- Surgical Infections Surgical Infections: HistoryDocument7 pagesSurgical Infections Surgical Infections: Historyjc_sibal13No ratings yet
- Surgical Infections Surgical Infections: HistoryDocument7 pagesSurgical Infections Surgical Infections: Historyjc_sibal13No ratings yet
- Surgical MetabolismDocument10 pagesSurgical Metabolismjc_sibal13No ratings yet
- Surgical MetabolismDocument12 pagesSurgical Metabolismjc_sibal13No ratings yet
- Systemic Response To InjuryDocument7 pagesSystemic Response To Injuryjc_sibal13No ratings yet
- Fluids and ElectrolytesDocument10 pagesFluids and Electrolytesjc_sibal13No ratings yet
- Systemic Response To InjuryDocument7 pagesSystemic Response To Injuryjc_sibal13No ratings yet
- Systemic Response To InjuryDocument2 pagesSystemic Response To Injuryjc_sibal13100% (1)
- Surgical MetabolismDocument12 pagesSurgical Metabolismjc_sibal13No ratings yet
- Fluids and ElectrolytesDocument10 pagesFluids and Electrolytesjc_sibal13No ratings yet
- CytokinesDocument2 pagesCytokinesjc_sibal13No ratings yet
- Discuss The Essentials of Hemostasis and Surgical BleedingDocument10 pagesDiscuss The Essentials of Hemostasis and Surgical Bleedingjc_sibal13No ratings yet
- Discuss The Essentials of Hemostasis and Surgical BleedingDocument17 pagesDiscuss The Essentials of Hemostasis and Surgical Bleedingjc_sibal13No ratings yet
- Discuss The Essentials of Hemostasis and Surgical BleedingDocument5 pagesDiscuss The Essentials of Hemostasis and Surgical Bleedingjc_sibal13No ratings yet
- Bleeding and Transfusion: Section I ResuscitationDocument22 pagesBleeding and Transfusion: Section I Resuscitationjc_sibal13No ratings yet
- Wound Healing Wound Healing and Wound and Wound Care Care Care CareDocument7 pagesWound Healing Wound Healing and Wound and Wound Care Care Care Carejc_sibal13No ratings yet
- EXAM QUESTIONS On Wound Healing and Surgical Site InfectionsDocument2 pagesEXAM QUESTIONS On Wound Healing and Surgical Site Infectionsjc_sibal13No ratings yet
- Urea Cycle Regulation and DisordersDocument41 pagesUrea Cycle Regulation and DisordersWahab KhaniNo ratings yet
- Amino Acids, Fatty Acids, and Dietary Fibre in Edible Seaweed ProductsDocument10 pagesAmino Acids, Fatty Acids, and Dietary Fibre in Edible Seaweed ProductsNadjla ChaïbNo ratings yet
- Lecture 2: Enzymes: Computational Systems BiologyDocument19 pagesLecture 2: Enzymes: Computational Systems Biologyahmad aliNo ratings yet
- Structure Based Drug Design - Muya PDFDocument831 pagesStructure Based Drug Design - Muya PDFIsis BugiaNo ratings yet
- BCH101 - L1 - The Chemical Basis of LifeDocument52 pagesBCH101 - L1 - The Chemical Basis of Lifesrabonty.siddikyNo ratings yet
- Experiment No1 Protein AnalysisDocument3 pagesExperiment No1 Protein AnalysisYellowNo ratings yet
- Acs Biochem 7b00795Document5 pagesAcs Biochem 7b00795Romana MasnikosaNo ratings yet
- Estimation of Amino Acids by Ninhydrin MethodDocument3 pagesEstimation of Amino Acids by Ninhydrin MethodSukaina AbbasNo ratings yet
- Amino Acid and Protein PropertiesDocument12 pagesAmino Acid and Protein PropertiesAthinaNo ratings yet
- A Review of The Recent Developments in Biocomposites Based On Natural Fibres and Their Application PerspectivesDocument25 pagesA Review of The Recent Developments in Biocomposites Based On Natural Fibres and Their Application Perspectivesmn.gautamNo ratings yet
- DEMETHYLATION PROCEDUREDocument4 pagesDEMETHYLATION PROCEDUREFelipe MonteroNo ratings yet
- Protein FoldingDocument13 pagesProtein Foldingisaiah tariqNo ratings yet
- HPLC For Amino AcidDocument8 pagesHPLC For Amino AcidSylvia N. UtamaNo ratings yet
- Effect of Cold Plasma-Activated Water On The Physicochemical and Functional Properties of Bambara Groundnut GlobulinDocument10 pagesEffect of Cold Plasma-Activated Water On The Physicochemical and Functional Properties of Bambara Groundnut GlobulinKwabena MboomNo ratings yet
- B.SC Dialysis Technology First Year Paper I - Biochemistry I. Elaborate On: (3 10 30)Document5 pagesB.SC Dialysis Technology First Year Paper I - Biochemistry I. Elaborate On: (3 10 30)Jenifer DheboralNo ratings yet
- Biorefinery Methods For Extraction of Oil and Protein From Rubber SeedDocument11 pagesBiorefinery Methods For Extraction of Oil and Protein From Rubber SeedShivamNo ratings yet
- BIOMOLECULES Note (1st Class)Document10 pagesBIOMOLECULES Note (1st Class)Soumyadeep ChatterjeeNo ratings yet
- Bashir2016 Spirulina Platensis ProteinDocument8 pagesBashir2016 Spirulina Platensis Proteinanon_509992240No ratings yet
- Functionalized PEG for Biologically Relevant ConjugatesDocument16 pagesFunctionalized PEG for Biologically Relevant ConjugatesFranciscoNo ratings yet
- A Study of Milk Coagulability-PhD-2014Document145 pagesA Study of Milk Coagulability-PhD-2014ziza20 ZizaNo ratings yet
- Characteristics and Uses of CollagenDocument6 pagesCharacteristics and Uses of CollagenRoxana ElenaNo ratings yet
- Characterization of Intact Protein and Hydrolyzate by Color ReactionsDocument5 pagesCharacterization of Intact Protein and Hydrolyzate by Color ReactionsakeriaravenheartNo ratings yet
- Non Ruminant DigestionDocument29 pagesNon Ruminant Digestionshivabt07No ratings yet
- BIOMOLECULESDocument54 pagesBIOMOLECULESTanmayNo ratings yet
- Spoilage of Protein & CarbsDocument43 pagesSpoilage of Protein & CarbsA RahmanNo ratings yet
- Cheese Flavor and The GenomicsDocument8 pagesCheese Flavor and The GenomicsharizNo ratings yet
- Tifr 2012 ChemistryDocument7 pagesTifr 2012 ChemistryDHARMVEER BHEDINo ratings yet
- Ace-2 Structure and Covid ReceptorDocument8 pagesAce-2 Structure and Covid ReceptorJin Xiai TianNo ratings yet
- Nutrition Concepts and Controversies 14th Edition Sizer Test BankDocument32 pagesNutrition Concepts and Controversies 14th Edition Sizer Test Bankstarostyadjustaged5p100% (23)
- L4.1 Protein StructureDocument23 pagesL4.1 Protein StructureAzamu Shahiullah ProttoyNo ratings yet
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Power Souping: 3-Day Detox, 3-Week Weight-Loss PlanFrom EverandPower Souping: 3-Day Detox, 3-Week Weight-Loss PlanRating: 3.5 out of 5 stars3.5/5 (3)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (3)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyFrom EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyRating: 5 out of 5 stars5/5 (1)
- Keto Friendly Recipes: Easy Keto For Busy PeopleFrom EverandKeto Friendly Recipes: Easy Keto For Busy PeopleRating: 2 out of 5 stars2/5 (1)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouFrom EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNo ratings yet
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- Allen Carr's Easy Way for Women to Lose Weight: The original Easyway methodFrom EverandAllen Carr's Easy Way for Women to Lose Weight: The original Easyway methodRating: 4.5 out of 5 stars4.5/5 (18)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeFrom EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNo ratings yet
- Glucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingFrom EverandGlucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingRating: 5 out of 5 stars5/5 (59)
- The Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthFrom EverandThe Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthRating: 5 out of 5 stars5/5 (37)
- Happy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainFrom EverandHappy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainRating: 3.5 out of 5 stars3.5/5 (6)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- Summary of Mary Claire Haver's The Galveston DietFrom EverandSummary of Mary Claire Haver's The Galveston DietRating: 5 out of 5 stars5/5 (1)
- Lose Weight by Eating: 130 Amazing Clean-Eating Makeovers for Guilt-Free Comfort FoodFrom EverandLose Weight by Eating: 130 Amazing Clean-Eating Makeovers for Guilt-Free Comfort FoodRating: 2 out of 5 stars2/5 (1)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthFrom EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNo ratings yet
- The Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossFrom EverandThe Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossRating: 4 out of 5 stars4/5 (22)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeFrom EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeRating: 5 out of 5 stars5/5 (1)
- Proteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItFrom EverandProteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItRating: 4.5 out of 5 stars4.5/5 (19)
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeFrom EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeRating: 4 out of 5 stars4/5 (3)
- The Longevity Plan: Seven Life-Transforming Lessons from Ancient ChinaFrom EverandThe Longevity Plan: Seven Life-Transforming Lessons from Ancient ChinaNo ratings yet
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- Ultrametabolism: The Simple Plan for Automatic Weight LossFrom EverandUltrametabolism: The Simple Plan for Automatic Weight LossRating: 4.5 out of 5 stars4.5/5 (28)
- How Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseFrom EverandHow Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseRating: 4.5 out of 5 stars4.5/5 (83)
- The Ultimate Volumetrics Diet: Smart, Simple, Science-Based Strategies for Losing Weight and Keeping It OffFrom EverandThe Ultimate Volumetrics Diet: Smart, Simple, Science-Based Strategies for Losing Weight and Keeping It OffNo ratings yet
- Think Yourself Thin: A 30-Day Guide to Permanent Weight LossFrom EverandThink Yourself Thin: A 30-Day Guide to Permanent Weight LossRating: 4.5 out of 5 stars4.5/5 (22)
- The Toxin Solution: How Hidden Poisons in the Air, Water, Food, and Products We Use Are Destroying Our Health—AND WHAT WE CAN DO TO FIX ITFrom EverandThe Toxin Solution: How Hidden Poisons in the Air, Water, Food, and Products We Use Are Destroying Our Health—AND WHAT WE CAN DO TO FIX ITRating: 5 out of 5 stars5/5 (1)