You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Prescott Harley Klein's Microbiology 7th EditionDocument37 pagesPrescott Harley Klein's Microbiology 7th EditionJendri Mamangkey-kossoh25% (4)
- Test Bank For Biology The Essentials 3rd EditionDocument8 pagesTest Bank For Biology The Essentials 3rd EditionKristi Markus100% (35)
- NOTESmtlaws LectureDocument11 pagesNOTESmtlaws LectureCes Manga100% (1)
- NotesCM (CEFI)Document30 pagesNotesCM (CEFI)Ces MangaNo ratings yet
- Books OverviewDocument10 pagesBooks OverviewCes MangaNo ratings yet
- The Measurement of Blood PressureDocument2 pagesThe Measurement of Blood PressureCes MangaNo ratings yet
- Animal Behavior Biological RhythmsDocument3 pagesAnimal Behavior Biological RhythmsAlok PatraNo ratings yet
- Yeast Make-Accumulate-Consume'' Life Strategy Evolved As A Multi-Step Process That Predates The Whole Genome DuplicationDocument12 pagesYeast Make-Accumulate-Consume'' Life Strategy Evolved As A Multi-Step Process That Predates The Whole Genome DuplicationdaveNo ratings yet
- Descriptive Text and A Diagram or Plan, Which You Have To Label According To TheDocument6 pagesDescriptive Text and A Diagram or Plan, Which You Have To Label According To TheJoanna BinanNo ratings yet
- The Role of Insulin in Maintaining Blood Glucose HomeostasisDocument2 pagesThe Role of Insulin in Maintaining Blood Glucose HomeostasisyaniqueNo ratings yet
- La Signifiance GnayoroDocument15 pagesLa Signifiance GnayorojeuneppNo ratings yet
- Animal Behaviour - Syamala Devi Natarajan - 1Document21 pagesAnimal Behaviour - Syamala Devi Natarajan - 1Syamala NatarajanNo ratings yet
- Ncku Courses Taught in English, AY2018-19: White Background: Undergraduate Level Gray Background: Graduate LevelDocument17 pagesNcku Courses Taught in English, AY2018-19: White Background: Undergraduate Level Gray Background: Graduate Levelasistensi varaNo ratings yet
- 19 Soft Tissue Tumors by DR NazishDocument55 pages19 Soft Tissue Tumors by DR NazishAhmed YTNo ratings yet
- Kalyanaraman B, 2013 - Teaching The Basic of Redox BiologyDocument14 pagesKalyanaraman B, 2013 - Teaching The Basic of Redox BiologyAnia Scholastika PutriNo ratings yet
- Surgical Pathology of Liver TumorsDocument480 pagesSurgical Pathology of Liver TumorsGeorgiana BuhociNo ratings yet
- Lesson 4 The Nucleus and DNA Organization and PBL Write Shops 5 6Document15 pagesLesson 4 The Nucleus and DNA Organization and PBL Write Shops 5 6Macky IbayNo ratings yet
- Oliveira Et Al. 2003Document8 pagesOliveira Et Al. 2003la_lu_izaNo ratings yet
- Nutrient Cycles: Answer The Questions BelowDocument7 pagesNutrient Cycles: Answer The Questions BelowNunuNo ratings yet
- 18 JL 7Document15 pages18 JL 7Irma SihotangNo ratings yet
- 17 BioDocument3 pages17 Biomuskan FatimaNo ratings yet
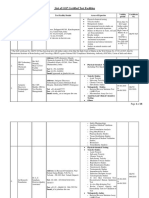
- List of GLP Certified Test FacilitiesDocument18 pagesList of GLP Certified Test FacilitiesBhushanNo ratings yet
- Biomedical Applications of CollagenDocument22 pagesBiomedical Applications of Collagenkiks123No ratings yet
- Tumour VirusesDocument57 pagesTumour VirusesCharles TownsendNo ratings yet
- 3rd Grading Exam ScienceDocument4 pages3rd Grading Exam ScienceRussel OchoNo ratings yet
- To Life Science: Maryrose Mallorca Peter Joedale Daling John Carlo Santiago "Pogi"Document33 pagesTo Life Science: Maryrose Mallorca Peter Joedale Daling John Carlo Santiago "Pogi"Jhen BonNo ratings yet
- Chemistry Education Research and Practice: Accepted ManuscriptDocument55 pagesChemistry Education Research and Practice: Accepted ManuscriptMusic HitzNo ratings yet
- Ethics in Behavioral GeneticsDocument8 pagesEthics in Behavioral GeneticsLavinia MariaNo ratings yet
- Bio 111 Biomolecules and CellsDocument2 pagesBio 111 Biomolecules and CellsDerrickNo ratings yet
- Brock Biology of MicrooDocument6 pagesBrock Biology of MicrooÇağla Koca100% (1)
- DR Vidya SagarDocument7 pagesDR Vidya SagarAnil KumarNo ratings yet
- Carbohydrates: Why Are Carbohydrates Important?Document4 pagesCarbohydrates: Why Are Carbohydrates Important?ir123No ratings yet
- Stem Cell Based Therapy Option in COVID-19 - Is It Really Promising?Document17 pagesStem Cell Based Therapy Option in COVID-19 - Is It Really Promising?diana.alyNo ratings yet
- Kelompok 2 - Keuntungan SSFDocument7 pagesKelompok 2 - Keuntungan SSFVirga ArgaNo ratings yet