You might also like
- Movement and Stability Dysfunction Conte PDFDocument12 pagesMovement and Stability Dysfunction Conte PDFGabriela RfNo ratings yet
- Training The Antifragile Athlete - A Preliminary Analysis of Neuromuscular Training Effects On Muscle Activation DynamicsDocument22 pagesTraining The Antifragile Athlete - A Preliminary Analysis of Neuromuscular Training Effects On Muscle Activation DynamicsGoranMarkovicNo ratings yet
- Strength Versus Stability - Part 1 Concept and Terms PDFDocument11 pagesStrength Versus Stability - Part 1 Concept and Terms PDFDiego Cruces OrdoñezNo ratings yet
- Pelvic Stability & Your Core: Written by Diane LeeDocument9 pagesPelvic Stability & Your Core: Written by Diane LeeisaNo ratings yet
- Dasar Rias 2Document9 pagesDasar Rias 2AnDi Anggara PeramanaNo ratings yet
- The Kinesiopathological Model and Mechanical Low Back PainDocument10 pagesThe Kinesiopathological Model and Mechanical Low Back PainGiovanny Vasquez VillegasNo ratings yet
- Stabilization Exercise For The Management of Low Back PainDocument33 pagesStabilization Exercise For The Management of Low Back PainKun HenriettaNo ratings yet
- Protocol For Core TrainingDocument31 pagesProtocol For Core Trainingpratapravindran100% (1)
- IBITA Assumptions enDocument12 pagesIBITA Assumptions enPedro FonsecaNo ratings yet
- Scapula Setting AnaIsabel AlmeidaDocument1 pageScapula Setting AnaIsabel AlmeidaPeter ZachNo ratings yet
- Basic of Manual TherapyDocument30 pagesBasic of Manual Therapycamy bhagatNo ratings yet
- Balance Assessment and TreatmentDocument55 pagesBalance Assessment and TreatmentMhmd Iraky100% (1)
- Gps Therapeutic PathwaysDocument16 pagesGps Therapeutic PathwaysStef HarleyNo ratings yet
- J Neurophysiol 2014 Rankin 374 83Document10 pagesJ Neurophysiol 2014 Rankin 374 83barros6No ratings yet
- Effects of Scapular Stabilization Exercises on Shoulder ImpingementDocument15 pagesEffects of Scapular Stabilization Exercises on Shoulder ImpingementDr Ahmed NabilNo ratings yet
- Interpretation of Modified FORCE CLOSURE Model: (Mark Comerford MCSP B.Phty MAPA)Document5 pagesInterpretation of Modified FORCE CLOSURE Model: (Mark Comerford MCSP B.Phty MAPA)karl24No ratings yet
- Locomotor SlingsDocument4 pagesLocomotor SlingsPhooi Yee LauNo ratings yet
- Assessing Lateral Hip StabilityDocument7 pagesAssessing Lateral Hip StabilityCristian Alejandro Flores PinuerNo ratings yet
- Clinical Lumbar Instability and Core Stabilization Exercise: A Literature ReviewDocument16 pagesClinical Lumbar Instability and Core Stabilization Exercise: A Literature ReviewwladjaNo ratings yet
- Spinal Stabilization Biomechanics UpdateDocument5 pagesSpinal Stabilization Biomechanics UpdateJenny IldefonsoNo ratings yet
- Chiropractic Technique Principles and Procedures 3Document22 pagesChiropractic Technique Principles and Procedures 3Colors of LifeNo ratings yet
- Rossi2014 PDFDocument8 pagesRossi2014 PDFDiana Magnavita MouraNo ratings yet
- Treatment of Proximal Hamstring Pain Using Active Release TechniqueDocument10 pagesTreatment of Proximal Hamstring Pain Using Active Release TechniqueRahees KhanNo ratings yet
- Jenkins, 2010 PDFDocument13 pagesJenkins, 2010 PDFPablo fernandezNo ratings yet
- Kinetic Control Cap1Document17 pagesKinetic Control Cap1Yennifer Serna MoncadaNo ratings yet
- Review Article: Kinetic Chain Rehabilitation: A Theoretical FrameworkDocument9 pagesReview Article: Kinetic Chain Rehabilitation: A Theoretical FrameworkVizaNo ratings yet
- First-Page Spinal ControlDocument1 pageFirst-Page Spinal ControlReagir ReagirNo ratings yet
- Biomechanical and Neurophysiological Mechanisms Related To Postural Control and Efficiency of Movement: A ReviewDocument15 pagesBiomechanical and Neurophysiological Mechanisms Related To Postural Control and Efficiency of Movement: A ReviewRicardoNo ratings yet
- Full Text 01Document20 pagesFull Text 01saurav.das2030No ratings yet
- Immediate Effects of Ankle Joint Mobilization With Movement OnDocument10 pagesImmediate Effects of Ankle Joint Mobilization With Movement OnChrissyNo ratings yet
- Manual Muscle Testing (MMT) : Dr. Neha KashyapDocument66 pagesManual Muscle Testing (MMT) : Dr. Neha KashyapshushmaNo ratings yet
- Paper Positional Release Technique SF MWDocument17 pagesPaper Positional Release Technique SF MWkamNo ratings yet
- Application of Fascial Manipulation Technique in Chronic Shoulder PainDocument9 pagesApplication of Fascial Manipulation Technique in Chronic Shoulder PainIsabelGuijarroMartinezNo ratings yet
- Core Stability An IntroductionDocument70 pagesCore Stability An Introductionruth sosaNo ratings yet
- Application of Fascial Manipulation Technique in Chronic Shoulder PainDocument8 pagesApplication of Fascial Manipulation Technique in Chronic Shoulder PainEnyaw DroffatsNo ratings yet
- LORMA COLLEGES THERAPEUTIC EXERCISE MODULEDocument13 pagesLORMA COLLEGES THERAPEUTIC EXERCISE MODULEZgama AbdulrahmanNo ratings yet
- Postural Orientation and Equilibrium: What Do We Need To Know About Neural Control of Balance To Prevent Falls?Document5 pagesPostural Orientation and Equilibrium: What Do We Need To Know About Neural Control of Balance To Prevent Falls?Karla Alzenda CruzeiroNo ratings yet
- Bauer 2019Document10 pagesBauer 2019Rafa ZalfaNo ratings yet
- Balancing in Handstand On The Floor: Petr Hedbávný, Jana Sklenaříková, Dušan Hupka, Miriam KalichováDocument11 pagesBalancing in Handstand On The Floor: Petr Hedbávný, Jana Sklenaříková, Dušan Hupka, Miriam KalichovámargaritassNo ratings yet
- Soft Tissue DysfunctionDocument8 pagesSoft Tissue DysfunctionphysioaliNo ratings yet
- Strain Counter-Strain PDFDocument7 pagesStrain Counter-Strain PDFCarlosCarpinteroRubioNo ratings yet
- Chapter 7 - Management of The Hypermobile AdultDocument19 pagesChapter 7 - Management of The Hypermobile AdultDavid MansoNo ratings yet
- Theoretical Considerations in Balance AssessmentDocument12 pagesTheoretical Considerations in Balance AssessmentJuliette Salum AeschlimannNo ratings yet
- Or Tho TicsDocument11 pagesOr Tho TicsvsripathirajaNo ratings yet
- Mechanisms of Postural Control and Movement EfficiencyDocument28 pagesMechanisms of Postural Control and Movement Efficiencymerloy84No ratings yet
- Lumbopelvic Stability: SyllabusDocument13 pagesLumbopelvic Stability: Syllabusrapannika100% (3)
- Animal Movement, Mechanical Tuning and Coupled SystemsDocument7 pagesAnimal Movement, Mechanical Tuning and Coupled SystemsFadhlan MuchlasNo ratings yet
- Lex D de Jong, Pieter U Dijkstra, Johan Gerritsen, Alexander CH Geurts and Klaas PostemaDocument12 pagesLex D de Jong, Pieter U Dijkstra, Johan Gerritsen, Alexander CH Geurts and Klaas PostemaAnggelia jopa sariNo ratings yet
- SENSORY MOTOR TRAINING FOR BALANCE AND POSTURAL CONTROLDocument7 pagesSENSORY MOTOR TRAINING FOR BALANCE AND POSTURAL CONTROLGiancarlo Gardella Martínez100% (1)
- Ankle Inestability Article EvidenceDocument6 pagesAnkle Inestability Article EvidenceAldo Martínez SerranoNo ratings yet
- Kozar ScienceOfMotorControlLectureDocument114 pagesKozar ScienceOfMotorControlLectureMari PaoNo ratings yet
- Kinesiology For Occupational Therapy-32-50Document19 pagesKinesiology For Occupational Therapy-32-50birjuNo ratings yet
- Cervico Thoracic Rehab ProgramDocument20 pagesCervico Thoracic Rehab ProgramulaNo ratings yet
- Combined Arm Stretch Positioning and Neuromuscular Electrical Stimulation in Patients After Stroke A Random TrialDocument10 pagesCombined Arm Stretch Positioning and Neuromuscular Electrical Stimulation in Patients After Stroke A Random TrialwahyonoNo ratings yet
- Muscle Shortening Manoeuver in CPDocument6 pagesMuscle Shortening Manoeuver in CPlabsoneducationNo ratings yet
- MWM Prescription ParametersDocument21 pagesMWM Prescription ParametersKanika SinhaNo ratings yet
- Functional Rehabilitation of Some Common Neurological Conditions: A Physical Management Strategy to Optimise Functional Activity LevelFrom EverandFunctional Rehabilitation of Some Common Neurological Conditions: A Physical Management Strategy to Optimise Functional Activity LevelNo ratings yet
- EMG Flexion AnteriorDocument8 pagesEMG Flexion AnteriorSimon Ocares AranguizNo ratings yet
- A New Perspective On Risk AssessmentDocument12 pagesA New Perspective On Risk AssessmentSimon Ocares AranguizNo ratings yet
- Does A SLAP Lesion Affect Shoulder Muscle Recruitment As Measured by EMG Activity During A Rugby Tackle?Document10 pagesDoes A SLAP Lesion Affect Shoulder Muscle Recruitment As Measured by EMG Activity During A Rugby Tackle?Simon Ocares AranguizNo ratings yet
- Terapia Manual Research ReviewDocument3 pagesTerapia Manual Research ReviewSimon Ocares AranguizNo ratings yet
- Massage Low Back PainDocument15 pagesMassage Low Back PainSimon Ocares AranguizNo ratings yet
- J Crad 2007 11 011Document7 pagesJ Crad 2007 11 011Simon Ocares AranguizNo ratings yet
- Bronfort Report 2010 ChiropracticDocument33 pagesBronfort Report 2010 ChiropracticvicarofskepticNo ratings yet
- Trigger PointsDocument14 pagesTrigger PointsJaime Belmar DíazNo ratings yet
- Biomechanics of The HipDocument12 pagesBiomechanics of The HipSimon Ocares AranguizNo ratings yet
- Phys Ther 2006 Medlicott 955 73Document21 pagesPhys Ther 2006 Medlicott 955 73Simon Ocares AranguizNo ratings yet
- Gluteal Muscle Activity and Patellofemoral Pain Syndrome, A Systematic ReviewDocument10 pagesGluteal Muscle Activity and Patellofemoral Pain Syndrome, A Systematic ReviewVale castroNo ratings yet
- Trigger PointsDocument14 pagesTrigger PointsJaime Belmar DíazNo ratings yet
- 98Document7 pages98Simon Ocares AranguizNo ratings yet
- Rehab Distal RadiusDocument14 pagesRehab Distal RadiusSimon Ocares AranguizNo ratings yet
- 1 PBDocument11 pages1 PBSimon Ocares AranguizNo ratings yet
- 1 s2.0 S1356689X12001488 MainDocument5 pages1 s2.0 S1356689X12001488 MainSimon Ocares AranguizNo ratings yet
- SCI Shoulder InjuriesDocument92 pagesSCI Shoulder InjuriesSimon Ocares AranguizNo ratings yet
- Efficacy of Electrical Nerve Stimulation For Chronic Musculoskeletal PainDocument9 pagesEfficacy of Electrical Nerve Stimulation For Chronic Musculoskeletal PainGiancarlo Gardella MartínezNo ratings yet
- Treatment Protocol Against Covid 19 From WWW - Ippocrateorg.orgDocument4 pagesTreatment Protocol Against Covid 19 From WWW - Ippocrateorg.orgJohnuri MoraNo ratings yet
- Intervenciones en Dermatitis Atópica CaninaDocument16 pagesIntervenciones en Dermatitis Atópica CaninaMaka.ibanezNo ratings yet
- Respiratory Anatomy & PhysiologyDocument28 pagesRespiratory Anatomy & PhysiologyKaye CorNo ratings yet
- The Wayland News November 2014Document20 pagesThe Wayland News November 2014Julian HornNo ratings yet
- Ventilator Associated Pneumonia 1Document14 pagesVentilator Associated Pneumonia 1Tulus ArisonoNo ratings yet
- Typhoid FeverDocument38 pagesTyphoid FeverRonelenePurisimaNo ratings yet
- Plab-1 1700 MCQs Solved With Explanation (Shared by Ussama Maqbool)Document729 pagesPlab-1 1700 MCQs Solved With Explanation (Shared by Ussama Maqbool)Omar Abo el nagaNo ratings yet
- 4 - Treatment of FracturesDocument28 pages4 - Treatment of FracturesmojahidmobarkNo ratings yet
- Human Values Case Study: Group-5 Kartikeya Berry 03851203119 It (Eve)Document25 pagesHuman Values Case Study: Group-5 Kartikeya Berry 03851203119 It (Eve)Kartikeya BerryNo ratings yet
- PreliminariesDocument6 pagesPreliminariesBe ChahNo ratings yet
- Showa University Introduces Dental Patient RobotDocument4 pagesShowa University Introduces Dental Patient RobotDent YomarajNo ratings yet
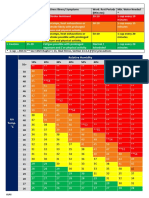
- Aramco Heat IndexDocument1 pageAramco Heat IndexDLPS HSE0% (1)
- Measuring Basic Observations: OSCE ChecklistDocument2 pagesMeasuring Basic Observations: OSCE Checklistahmad50% (4)
- Future Oriented PsychotherapyDocument10 pagesFuture Oriented PsychotherapyzarrarNo ratings yet
- Quotation of Pain Relief Laser Therapy Device-ZJKCDocument5 pagesQuotation of Pain Relief Laser Therapy Device-ZJKCsanthigiNo ratings yet
- Acetabulum Fractures - Classification and Management - Emile LetournelDocument26 pagesAcetabulum Fractures - Classification and Management - Emile LetournelThanat AuwattanamongkolNo ratings yet
- BreechDocument2 pagesBreechBrel KirbyNo ratings yet
- Applying Philosophy To Science and Technology by Sarah Jane ToledanoDocument24 pagesApplying Philosophy To Science and Technology by Sarah Jane ToledanoNicoelNo ratings yet
- 10 Essentials To Improving EyesightDocument9 pages10 Essentials To Improving EyesightdrakpoNo ratings yet
- Jurnal Case Report Carcinoma Maxillaris PDFDocument3 pagesJurnal Case Report Carcinoma Maxillaris PDFEnvhy WinaNo ratings yet
- A M CDocument769 pagesA M CMohammad Tanvir Khan94% (18)
- STM - Grp4 - Sec - B - ThedaCare..... Ques OneDocument3 pagesSTM - Grp4 - Sec - B - ThedaCare..... Ques OneAdam MorganNo ratings yet
- Respiratory Questions by DR - OkashaDocument96 pagesRespiratory Questions by DR - Okashamohammed okashaNo ratings yet
- Practical Book of TherapeuticsDocument28 pagesPractical Book of TherapeuticsSara AbdoNo ratings yet
- Physics of Blood FlowDocument15 pagesPhysics of Blood FlowNahidNo ratings yet
- Bee Venom Therapy: Dr. Joanne R. MirandaDocument25 pagesBee Venom Therapy: Dr. Joanne R. MirandaValerie Villena67% (3)
- Course Outline (Anatomy)Document3 pagesCourse Outline (Anatomy)Jhason John J. CabigonNo ratings yet
- Demo Doctor - Edit PrescriptionDocument1 pageDemo Doctor - Edit PrescriptiongauravchauNo ratings yet
- TK Heme 13-24Document49 pagesTK Heme 13-24rotat2348No ratings yet
- The CORE Understanding It and Retraining Its DysfunctionDocument19 pagesThe CORE Understanding It and Retraining Its DysfunctionAriene RibeiroNo ratings yet