You might also like
- Intrusion Arches ShinuDocument66 pagesIntrusion Arches ShinuYuvashreeNo ratings yet
- Scissors Bite-Dragon Helix ApplianceDocument6 pagesScissors Bite-Dragon Helix ApplianceGaurav PatelNo ratings yet
- Open-Bite Malocclusion: Treatment and StabilityFrom EverandOpen-Bite Malocclusion: Treatment and StabilityGuilherme JansonRating: 5 out of 5 stars5/5 (1)
- Clinical Cases in Restorative and Reconstructive DentistryFrom EverandClinical Cases in Restorative and Reconstructive DentistryRating: 5 out of 5 stars5/5 (1)
- Fundamentals of Oral and Maxillofacial RadiologyFrom EverandFundamentals of Oral and Maxillofacial RadiologyRating: 4 out of 5 stars4/5 (1)
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFrom EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiNo ratings yet
- Burstone1962 PDFDocument18 pagesBurstone1962 PDFParameswaran ManiNo ratings yet
- Deepbite Correction With Incisor Intrusion inDocument6 pagesDeepbite Correction With Incisor Intrusion inAbad SalcedoNo ratings yet
- Methods of Correction of Unilateral Posterior CrossbiteDocument36 pagesMethods of Correction of Unilateral Posterior CrossbiteSwathiLingannagariNo ratings yet
- Skeletal Anchorage Systems in Orthodontics Absolute Anchorage Adream or RealityDocument10 pagesSkeletal Anchorage Systems in Orthodontics Absolute Anchorage Adream or RealitySoe San KyawNo ratings yet
- Early Alt-RAMEC and Facial Mask Protocol in Class III MalocclusionDocument9 pagesEarly Alt-RAMEC and Facial Mask Protocol in Class III MalocclusionNievecillaNeiraNo ratings yet
- Self-ligating brackets do not increase orthodontic treatment efficiencyDocument22 pagesSelf-ligating brackets do not increase orthodontic treatment efficiencyAnkit ChaurhaNo ratings yet
- Removable Appliance TherapyDocument6 pagesRemovable Appliance TherapyardyvanviestaNo ratings yet
- Open BiteDocument6 pagesOpen BiteBarot brindaNo ratings yet
- Drugs Commonly Used in Orthodontics and Their EffectsDocument43 pagesDrugs Commonly Used in Orthodontics and Their EffectsSushma Rayal SANo ratings yet
- Journal Club List Second Year Postgraduates: Department of Orthodontics and Dentofacial OrthopedicsDocument6 pagesJournal Club List Second Year Postgraduates: Department of Orthodontics and Dentofacial OrthopedicsMariyam0% (1)
- Sunday, March 2, 2008: Important Orthodontic StudiesDocument6 pagesSunday, March 2, 2008: Important Orthodontic StudiesXnb HajiNo ratings yet
- Orthodontic Management of A Maxillary Midline Diastema Using Beggs Mechanics Case ReportDocument3 pagesOrthodontic Management of A Maxillary Midline Diastema Using Beggs Mechanics Case ReportEditor IJTSRDNo ratings yet
- 66 Allery and OrthodonticDocument5 pages66 Allery and OrthodonticShruthi KamarajNo ratings yet
- The Midline Diagnosis and Treatment ARTUROCAMACHODocument10 pagesThe Midline Diagnosis and Treatment ARTUROCAMACHOMiguel AngelNo ratings yet
- Placing Piggy Back An Easy Way OutDocument2 pagesPlacing Piggy Back An Easy Way OutMawar Putri JulicaNo ratings yet
- Space AnalysisDocument43 pagesSpace AnalysismarieNo ratings yet
- Biomechanics of Deep Overbite CorrectionDocument8 pagesBiomechanics of Deep Overbite CorrectionLuis Paipay SantosNo ratings yet
- Management of Vertical Maxillary ExcessDocument24 pagesManagement of Vertical Maxillary ExcesssweetieNo ratings yet
- Orthodontics Classification of Skeletal PDFDocument7 pagesOrthodontics Classification of Skeletal PDFPriyank RaiNo ratings yet
- Perioral Forces and Dental Changes Resulting From Lip BumperDocument9 pagesPerioral Forces and Dental Changes Resulting From Lip Bumpersolodont1No ratings yet
- Finishing in Lingual OrthodonticsDocument7 pagesFinishing in Lingual OrthodonticsSreenivasa Krishna ChaitanyaNo ratings yet
- Arch ExpansionDocument32 pagesArch ExpansionMoola Bharath Reddy100% (5)
- Impacted Canine: Presented By: Dr. Ahmed Shihab Supervised By: Dr. SarahDocument34 pagesImpacted Canine: Presented By: Dr. Ahmed Shihab Supervised By: Dr. SarahAhmed ShihabNo ratings yet
- 3-Extraoral and Functional AppliancesDocument52 pages3-Extraoral and Functional Appliancessamar yousif mohamedNo ratings yet
- Growth QuesDocument8 pagesGrowth QuesShameer SFsNo ratings yet
- 3-Molar Distalization With Modified Palatal DistalizerDocument8 pages3-Molar Distalization With Modified Palatal DistalizerJunaid Israr - OrthodonticsNo ratings yet
- Face MaskDocument7 pagesFace MaskWaraphon JanewakornwongNo ratings yet
- Static Equilibrium and It's Importance - Mulligan-2 PDFDocument14 pagesStatic Equilibrium and It's Importance - Mulligan-2 PDFdrzana78No ratings yet
- Biomechanical Implications of Rotation Correction in Orthodontics - Case SeriesDocument5 pagesBiomechanical Implications of Rotation Correction in Orthodontics - Case SeriescempapiNo ratings yet
- TWEED PROFILE: FACIAL ESTHETICS AND MECHANICSDocument60 pagesTWEED PROFILE: FACIAL ESTHETICS AND MECHANICSJu Ju WareeratNo ratings yet
- Fudamentals of Biomechanics and Biomechanics of Levelling and Aligning Includes Biomechanics of Molar Control PDFDocument326 pagesFudamentals of Biomechanics and Biomechanics of Levelling and Aligning Includes Biomechanics of Molar Control PDFVioleta PajicNo ratings yet
- Wires FinalDocument120 pagesWires FinalarshabharataNo ratings yet
- Orthodontic Indices OverviewDocument10 pagesOrthodontic Indices OverviewBhavikPatelNo ratings yet
- Mixed DentitionDocument49 pagesMixed Dentitiongnna norNo ratings yet
- Sterilization in OrthodonticsDocument32 pagesSterilization in OrthodonticsLeo JuniorNo ratings yet
- Cone Beam Tomography in Orthodontics PDFDocument8 pagesCone Beam Tomography in Orthodontics PDFdruzair007No ratings yet
- Understanding the History and Mechanisms of the Activator ApplianceDocument91 pagesUnderstanding the History and Mechanisms of the Activator ApplianceCarlosAndresPabonCortesNo ratings yet
- Soft Tissus Ceph Analysis / Orthodontic Courses by Indian Dental AcademyDocument155 pagesSoft Tissus Ceph Analysis / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- Class III TTT OptionsDocument9 pagesClass III TTT OptionsMADANo ratings yet
- Guide to Timing Orthodontic TreatmentDocument5 pagesGuide to Timing Orthodontic Treatmentdrzana78No ratings yet
- Growth PredictionDocument64 pagesGrowth PredictionMothi KrishnaNo ratings yet
- Case Report Class III Orthodontic Camouflage: Is The "Ideal" Treatment Always The Best Option? A Documented Case ReportDocument7 pagesCase Report Class III Orthodontic Camouflage: Is The "Ideal" Treatment Always The Best Option? A Documented Case ReportDany PapuchoNo ratings yet
- Vari-Simplex DisciplineDocument60 pagesVari-Simplex DisciplineDrGurinder Kanwar100% (1)
- MDS in Orthodontics & Dentofacial OrthopedicsDocument12 pagesMDS in Orthodontics & Dentofacial OrthopedicsChetan S KumarNo ratings yet
- Journal Club / Orthodontic Courses by Indian Dental AcademyDocument19 pagesJournal Club / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Evaluation of Continuous Arch and Segmented Arch Leveling Techniques in Adult Patients-A Clinical Study PDFDocument6 pagesEvaluation of Continuous Arch and Segmented Arch Leveling Techniques in Adult Patients-A Clinical Study PDFDiana Paola FontechaNo ratings yet
- Maxillary molar distalization techniques under 40 charactersDocument8 pagesMaxillary molar distalization techniques under 40 charactersGoutam NookalaNo ratings yet
- Preventive OrthodonticsDocument14 pagesPreventive OrthodonticsVaisakh Ramachandran0% (1)
- Space AnalysisDocument43 pagesSpace AnalysismarieNo ratings yet
- Analysis of Diagnostic Records and Space EvaluationDocument78 pagesAnalysis of Diagnostic Records and Space EvaluationAtika Iftikhar MirNo ratings yet
- Bonding and Debonding From Metal To Ceramic: Research and Its Clinical ApplicationDocument13 pagesBonding and Debonding From Metal To Ceramic: Research and Its Clinical Applicationgriffone1No ratings yet
- The Clinical Application A Tooth-Size Analysis: IntroductiokDocument26 pagesThe Clinical Application A Tooth-Size Analysis: Introductiokapi-26468957No ratings yet
- An Analysis Permanent Mesiodistal Crown Sixe: Carlos Sanin and Bhim S. SavaraDocument13 pagesAn Analysis Permanent Mesiodistal Crown Sixe: Carlos Sanin and Bhim S. Savaraapi-26468957No ratings yet
- Managing Treatment For The Orthodontic Patient With Periodontal ProblemsDocument18 pagesManaging Treatment For The Orthodontic Patient With Periodontal Problemsapi-26468957No ratings yet
- A Longitudinal Study of Incremental Expansion Using A Mandibular Lip BumperDocument5 pagesA Longitudinal Study of Incremental Expansion Using A Mandibular Lip Bumperapi-26468957No ratings yet
- NullDocument14 pagesNullapi-26468957No ratings yet
- Beyond The Ligament: A Whole-Bone Periodontal View of Dentofacial Orthopedics and Falsification of Universal Alveolar ImmutabilityDocument14 pagesBeyond The Ligament: A Whole-Bone Periodontal View of Dentofacial Orthopedics and Falsification of Universal Alveolar Immutabilityapi-26468957No ratings yet
- Thinking Beyond The Wire: Emerging Biologic Relationships in Orthodontics andDocument15 pagesThinking Beyond The Wire: Emerging Biologic Relationships in Orthodontics andapi-26468957No ratings yet
- Bompereta Labial 2Document7 pagesBompereta Labial 2Aleja LombanaNo ratings yet
- NullDocument11 pagesNullapi-26468957No ratings yet
- Treatment Timing For Rapid Maxillary ExpansionDocument8 pagesTreatment Timing For Rapid Maxillary Expansiongriffone1No ratings yet
- Subgingival Microbial Samples From Patients With RefractoryDocument9 pagesSubgingival Microbial Samples From Patients With Refractoryapi-26468957No ratings yet
- Refractory Periodontitis Associated With Abnormal Polymorphonuclear Leucocyte PhagocytosisDocument8 pagesRefractory Periodontitis Associated With Abnormal Polymorphonuclear Leucocyte Phagocytosisapi-26468957No ratings yet
- Mcnamara in OrthodonticsDocument13 pagesMcnamara in Orthodonticsapi-26468957No ratings yet
- Time Interval Following Bonding Bond Failures Indirect DirectDocument7 pagesTime Interval Following Bonding Bond Failures Indirect Directapi-26468957No ratings yet
- Time Interval Following Bonding Bond Failures Indirect DirectDocument7 pagesTime Interval Following Bonding Bond Failures Indirect Directapi-26468957No ratings yet
- Postpone Elective Oral Surgical Procedures Until Cancer TreatmentDocument10 pagesPostpone Elective Oral Surgical Procedures Until Cancer Treatmentapi-26468957100% (2)
- Scorebuilders 6Document58 pagesScorebuilders 6pokharelriwaj82No ratings yet
- Muscle and Bone PalpationDocument9 pagesMuscle and Bone PalpationIzzati WanNo ratings yet
- SyllabusDocument6 pagesSyllabusRafkha HakamNo ratings yet
- Fetal Medicine FoundationDocument2 pagesFetal Medicine Foundationrrodriguezg1No ratings yet
- 3rd Quarter Exam Science 10Document3 pages3rd Quarter Exam Science 10Evelyn71% (7)
- C9apstudy GuideDocument37 pagesC9apstudy GuidejqtdNo ratings yet
- Physical Assessment Guide of Head-To-ToeDocument9 pagesPhysical Assessment Guide of Head-To-Toeneleh gray100% (2)
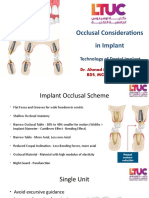
- Implant Occlusal Considerations for LongevityDocument16 pagesImplant Occlusal Considerations for LongevityDania TahboubNo ratings yet
- SGL Dan CST BEDAHDocument3 pagesSGL Dan CST BEDAHForensik UMINo ratings yet
- Humeral Shaft Fractures: Supervisior: Dr. Dewi Kurniati P, SP - OT Teguh Triananda PutraDocument20 pagesHumeral Shaft Fractures: Supervisior: Dr. Dewi Kurniati P, SP - OT Teguh Triananda Putrateguh triananda putraNo ratings yet
- CDDocument3 pagesCDMeireza AdityaNo ratings yet
- Stroke Rehab ExercisesDocument14 pagesStroke Rehab ExercisesEdna Mineva50% (2)
- LE Muscles OINADocument5 pagesLE Muscles OINAUshuaia Chely FilomenoNo ratings yet
- Meditation and Its Regulatory Role On Sleep: Ravindra P. Nagendra, Nirmala Maruthai and Bindu M. KuttyDocument4 pagesMeditation and Its Regulatory Role On Sleep: Ravindra P. Nagendra, Nirmala Maruthai and Bindu M. KuttyMariaNo ratings yet
- Esthetics in Dental ImplantsDocument87 pagesEsthetics in Dental ImplantsRavi Uttara100% (3)
- LXER - Gr12LifeSciences - The Human Eye and Ear - Nov2014Document10 pagesLXER - Gr12LifeSciences - The Human Eye and Ear - Nov2014Nicole Paul100% (1)
- 4 Cotofana 2016Document8 pages4 Cotofana 2016Thamyres Branco100% (1)
- English Masterclass - Speak English With VanessaDocument28 pagesEnglish Masterclass - Speak English With Vanessaisadacis cisnerosNo ratings yet
- Thyroid Examination and ThyroidectomyDocument9 pagesThyroid Examination and ThyroidectomyAhmadNo ratings yet
- (11.10) Imaging of The Endocrine System (TG1-CG14) Final VersionDocument12 pages(11.10) Imaging of The Endocrine System (TG1-CG14) Final VersionLANCE GILL TolentinoNo ratings yet
- 1.embryology Q ADocument11 pages1.embryology Q ADr P N N ReddyNo ratings yet
- Lungs IDocument34 pagesLungs Iavirajput1230987No ratings yet
- Anatomy of AgingDocument5 pagesAnatomy of AgingAndre3893No ratings yet
- Gordons PerosDocument14 pagesGordons PerosAlthea DetallaNo ratings yet
- Endocrine SystemDocument6 pagesEndocrine SystemCaviles, Jasmin S.No ratings yet
- Assessment CardsDocument3 pagesAssessment CardsLindsay Couillard100% (3)
- Chapter 6 - IntegumentaryDocument63 pagesChapter 6 - Integumentaryapi-297069611No ratings yet
- Lindo, Hannah Bea C. YOGADocument4 pagesLindo, Hannah Bea C. YOGAHannahbea LindoNo ratings yet
- Thyroiditis: What Is The Thyroid Gland?Document3 pagesThyroiditis: What Is The Thyroid Gland?Angga M RahmanNo ratings yet
- Aapc 2016Document92 pagesAapc 2016Ravi Pal75% (4)