You might also like
- 2011 - Autonomous Rangefinder System Based On PSOC PDFDocument67 pages2011 - Autonomous Rangefinder System Based On PSOC PDFpablocotanNo ratings yet
- Virtual Machine and Code Generator For PLC SystemsDocument369 pagesVirtual Machine and Code Generator For PLC SystemspablocotanNo ratings yet
- Thesis Comapring CoDeSys V2 and CoDeSys V3Document38 pagesThesis Comapring CoDeSys V2 and CoDeSys V3pablocotanNo ratings yet
- Ug Pna PDFDocument110 pagesUg Pna PDFpablocotanNo ratings yet
- Good 5990-7036en - Radar, Ew & Elint TestingDocument24 pagesGood 5990-7036en - Radar, Ew & Elint TestingpablocotanNo ratings yet
- How To Make Eye Catching User InterfacesDocument25 pagesHow To Make Eye Catching User InterfacespablocotanNo ratings yet
- UG1119 - Vivado Tutorial - Creating and Packaging Custom IP - Ver2015.2Document57 pagesUG1119 - Vivado Tutorial - Creating and Packaging Custom IP - Ver2015.2pablocotanNo ratings yet
- PFC PDFDocument92 pagesPFC PDFpablocotanNo ratings yet
- SASE2013 AllegroDocument20 pagesSASE2013 AllegropablocotanNo ratings yet
- FCC Antenna Factors PDFDocument6 pagesFCC Antenna Factors PDFpablocotan100% (1)
- 00 IntroductionDocument4 pages00 IntroductionpablocotanNo ratings yet
- Introduction to LabVIEW and Computer-Based MeasurementsDocument68 pagesIntroduction to LabVIEW and Computer-Based MeasurementsmgheryaniNo ratings yet
- PFC PDFDocument92 pagesPFC PDFpablocotanNo ratings yet
- Making Fast and Accurate Antenna MeasurementsDocument8 pagesMaking Fast and Accurate Antenna MeasurementspablocotanNo ratings yet
- Good 5989-7575en - Radar MeasurementsDocument88 pagesGood 5989-7575en - Radar MeasurementspablocotanNo ratings yet
- Development and Tests of A WSNDocument48 pagesDevelopment and Tests of A WSNpablocotanNo ratings yet
- Tips For Making Fast, Accurate Antenna MeasurementsDocument7 pagesTips For Making Fast, Accurate Antenna MeasurementspablocotanNo ratings yet
- Neuromonitoring SyllabusDocument9 pagesNeuromonitoring SyllabuspablocotanNo ratings yet
- Pic32mx1 - mx2 Starter KitDocument2 pagesPic32mx1 - mx2 Starter KitpablocotanNo ratings yet
- Arti Cial and Medical Innovations Applied To AnesthesiologyDocument2 pagesArti Cial and Medical Innovations Applied To AnesthesiologypablocotanNo ratings yet
- DM00039672 - AN3990 - Upgrading STM32F4DISCOVERY Board Firmware Using A USB KeyDocument14 pagesDM00039672 - AN3990 - Upgrading STM32F4DISCOVERY Board Firmware Using A USB KeypablocotanNo ratings yet
- Last UploadedDocument1 pageLast UploadedpablocotanNo ratings yet
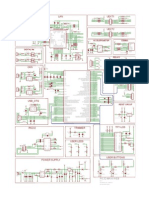
- PIC32 MAXI WEB Rev - A Schematic PDFDocument1 pagePIC32 MAXI WEB Rev - A Schematic PDFgeorgesmaccarioNo ratings yet
- Brstm32 - STM32 Platform ProcessorsDocument12 pagesBrstm32 - STM32 Platform ProcessorspablocotanNo ratings yet
- DM00038796 - AN3983 - STM32F4DISCOVERY Peripheral Firmware ExamplesDocument19 pagesDM00038796 - AN3983 - STM32F4DISCOVERY Peripheral Firmware ExamplespablocotanNo ratings yet
- 2008 - A Real-Time Person Detection Method For Moving CamerasDocument8 pages2008 - A Real-Time Person Detection Method For Moving CameraspablocotanNo ratings yet
- 2011 - Autonomous Rangefinder System Based On PSOCDocument67 pages2011 - Autonomous Rangefinder System Based On PSOCpablocotanNo ratings yet
- Software Utility For Control, Diagnostic and Communication With Inertial Measuring UnitDocument73 pagesSoftware Utility For Control, Diagnostic and Communication With Inertial Measuring UnitpablocotanNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Saint Paul University Newborn AssessmentDocument4 pagesSaint Paul University Newborn AssessmentCezanne Danabelle HutallaNo ratings yet
- Infection Control in NICUDocument9 pagesInfection Control in NICUMike CalipayanNo ratings yet
- AloeVeritas Announces The Launch of AloeMDDocument3 pagesAloeVeritas Announces The Launch of AloeMDPR.comNo ratings yet
- Report ViewerDocument2 pagesReport ViewerHamid RazaNo ratings yet
- Woodrow - PPT Chapter 1 8eDocument13 pagesWoodrow - PPT Chapter 1 8ete dyNo ratings yet
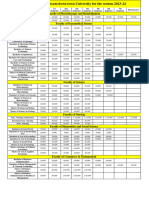
- Fees Structure Assam Down Town University For The Session 2023 2Document2 pagesFees Structure Assam Down Town University For The Session 2023 2Debashish SharmaNo ratings yet
- Uganda Health Sector and Partnership Opportunities Final PDFDocument69 pagesUganda Health Sector and Partnership Opportunities Final PDFPatrickLnanduNo ratings yet
- TKR OADocument1 pageTKR OAfitrianisyaNo ratings yet
- Sonographic Evaluation of The DiaphragmDocument1 pageSonographic Evaluation of The DiaphragmAngelo LongoniNo ratings yet
- Latino Voices: The Impacts of Crime and Criminal Justice Policies On LatinosDocument32 pagesLatino Voices: The Impacts of Crime and Criminal Justice Policies On LatinosLos Angeles Daily NewsNo ratings yet
- Accident English PracticeDocument2 pagesAccident English PracticeNindy Indah PratiwiNo ratings yet
- Obm 752-Hospital Management Cse Dept QPDocument2 pagesObm 752-Hospital Management Cse Dept QPJUSTUS KEVIN T 2019-2023 CSENo ratings yet
- 6.6 CEOS (Philadelphia, USA)Document14 pages6.6 CEOS (Philadelphia, USA)Tarot NightshadeNo ratings yet
- Residency Survival Guide: Canadian Association of General Surgeons Residents CommitteeDocument53 pagesResidency Survival Guide: Canadian Association of General Surgeons Residents CommitteeIrina MincuNo ratings yet
- Petrosea Klinik Medical Services AgreementDocument29 pagesPetrosea Klinik Medical Services AgreementChaqhim YvciNo ratings yet
- Preparation and Treatment of Periodontally Compromised DentitionDocument16 pagesPreparation and Treatment of Periodontally Compromised DentitionsankarNo ratings yet
- Malawi National Health Indicators FINAL v11 Clean WT Sign ComboDocument118 pagesMalawi National Health Indicators FINAL v11 Clean WT Sign ComboMarwa El SayedNo ratings yet
- Comparative Role of Pregabalin and Carbamazepine Regarding Efficacy in Painful Diabetic NeuropathyDocument4 pagesComparative Role of Pregabalin and Carbamazepine Regarding Efficacy in Painful Diabetic NeuropathyNur AyuNo ratings yet
- A Clinical Study of Abdominal Wound DehiscenceDocument25 pagesA Clinical Study of Abdominal Wound DehiscenceKarthikeyan RNo ratings yet
- Infection Control Checklist Nursing DepartmentDocument5 pagesInfection Control Checklist Nursing DepartmentNoreen PunjwaniNo ratings yet
- Hospital AdmissionDocument27 pagesHospital AdmissionHurley ReefNo ratings yet
- ModernaDocument22 pagesModernagoslugs12No ratings yet
- Philippine Clinical Practice Guidelines On The Diagnosis andDocument83 pagesPhilippine Clinical Practice Guidelines On The Diagnosis andREnren ConsolNo ratings yet
- DR Ela ResumeDocument2 pagesDR Ela Resumeellangovan marimuthuNo ratings yet
- 16.11.24 FBonora - 15 Tips For SJT SuccessDocument65 pages16.11.24 FBonora - 15 Tips For SJT SuccessUmer AnwarNo ratings yet
- GRK CertificateDocument1 pageGRK CertificateRadha KrishnaNo ratings yet
- Pharmacogenomics: Current Status and Future PerspectivesDocument13 pagesPharmacogenomics: Current Status and Future PerspectivesSergio VillicañaNo ratings yet
- Improving Hand Hygiene Practice at Adama Hospital Medical CollegeDocument9 pagesImproving Hand Hygiene Practice at Adama Hospital Medical Collegewassie gebiNo ratings yet
- Final Webcheck Stations Open - WebDocument6 pagesFinal Webcheck Stations Open - WebDiemut NaknanNo ratings yet
- Intravenous Drug Incompatibilities in The IntensivDocument6 pagesIntravenous Drug Incompatibilities in The IntensivJagan100% (1)