You might also like
- Ecg ReadingsDocument10 pagesEcg ReadingsSasa LuarNo ratings yet
- Ecg RhythmsDocument9 pagesEcg RhythmsNoreena PrincessNo ratings yet
- ECG ReadingDocument11 pagesECG ReadingSuresh Shrestha100% (1)
- ECG AbnormalitiesDocument9 pagesECG Abnormalitiesbigabm062No ratings yet
- Ecg Rhythms: Normal Sinus RhythmDocument10 pagesEcg Rhythms: Normal Sinus RhythmJethJayme100% (1)
- Normal Sinus RhythmDocument13 pagesNormal Sinus RhythmJackson Yovin ChellyadhasNo ratings yet
- Clinical Teaching Ecg InterpretationDocument25 pagesClinical Teaching Ecg InterpretationAnusha VergheseNo ratings yet
- Normal Sinus RhythmDocument8 pagesNormal Sinus RhythmRosalyn YuNo ratings yet
- ECG Rythum Study Guide PDFDocument9 pagesECG Rythum Study Guide PDFArtika MayandaNo ratings yet
- RhythmDocument8 pagesRhythmparkmickyboo100% (1)
- ECG InterpretationDocument11 pagesECG InterpretationAndrea AndradaNo ratings yet
- Electrocardiograph Y: Dr. Fatimah Eliana, SPPD, Kemd, FinasimDocument118 pagesElectrocardiograph Y: Dr. Fatimah Eliana, SPPD, Kemd, FinasimTommy WidjayaNo ratings yet
- Electrocardiography ECGDocument60 pagesElectrocardiography ECGSalman KhanNo ratings yet
- ECG Normal and AbnormalDocument74 pagesECG Normal and Abnormalawaniedream8391100% (1)
- Dr. Adeel Ahmed Waheed: House Officer M-4Document84 pagesDr. Adeel Ahmed Waheed: House Officer M-4Hussain AzharNo ratings yet
- Cheong Kuan Loong Medical Department Hospital Sultan Haji Ahmad Shah, Temerloh 12/5/10Document99 pagesCheong Kuan Loong Medical Department Hospital Sultan Haji Ahmad Shah, Temerloh 12/5/10Haq10No ratings yet
- The ElectrocardiogramDocument2 pagesThe ElectrocardiogramOh DehNo ratings yet
- Ecg WorkshopDocument39 pagesEcg WorkshopUber SnooferNo ratings yet
- ECG PracticalDocument48 pagesECG PracticalbvkjtzrvnyNo ratings yet
- ECGDocument6 pagesECGMatthew MackeyNo ratings yet
- ECGDocument41 pagesECGmiguel mendezNo ratings yet
- KRIZELDocument13 pagesKRIZELKrizel Adina TanNo ratings yet
- Ecg PreparationDocument15 pagesEcg PreparationErika Danalle ArceoNo ratings yet
- EKG RhythmsDocument71 pagesEKG RhythmsalexaNo ratings yet
- Normal ECGDocument26 pagesNormal ECGJan Christian AramburoNo ratings yet
- Ipd Kuliah Ekg Blok KegawatdaruratanDocument118 pagesIpd Kuliah Ekg Blok Kegawatdaruratansiti solikhaNo ratings yet
- Ecg FileDocument29 pagesEcg Fileneha miriNo ratings yet
- KalaiDocument47 pagesKalaiArya VikneshNo ratings yet
- Kamis 10 September 2015 - IPD 2 - Kuliah-Ekg-Blok-KegawatdaruratanDocument118 pagesKamis 10 September 2015 - IPD 2 - Kuliah-Ekg-Blok-KegawatdaruratanIrfanArifZulfikarNo ratings yet
- Basic ECG Interpretation Review Questions Flashcards - QuizletDocument5 pagesBasic ECG Interpretation Review Questions Flashcards - Quizletdina sharafNo ratings yet
- How To Read An ECGDocument21 pagesHow To Read An ECGSlychenkoNo ratings yet
- Cardiac Arrhythmias: Group 3ADocument39 pagesCardiac Arrhythmias: Group 3AAradhanaRamchandaniNo ratings yet
- How To Read An ECGDocument24 pagesHow To Read An ECGredroseeeeeeNo ratings yet
- ECG InterpretationDocument1 pageECG InterpretationCecil-An DalanonNo ratings yet
- Abnormal EcgDocument8 pagesAbnormal EcgM.DalaniNo ratings yet
- Electrocardiogram (ECG) : Voltage AmplitudeDocument15 pagesElectrocardiogram (ECG) : Voltage AmplitudeSafa SalmanNo ratings yet
- How To Read An ECGDocument15 pagesHow To Read An ECGSarah RonquilloNo ratings yet
- Definition ECGDocument8 pagesDefinition ECGMelody BoadoNo ratings yet
- How To Read An ECG: Confirm DetailsDocument15 pagesHow To Read An ECG: Confirm DetailsRinothja RajaratnamNo ratings yet
- Membaca EkgDocument90 pagesMembaca EkgDwi S WijayaNo ratings yet
- Abnomalites of ECGDocument81 pagesAbnomalites of ECGgrreddy8364320No ratings yet
- 2012 ECG HandoutDocument40 pages2012 ECG Handoutlizzy596No ratings yet
- Belajar Ekg YukDocument35 pagesBelajar Ekg Yukannisamuti10No ratings yet
- Ecg Reading Made EasyDocument59 pagesEcg Reading Made EasyAngealyn GaviolaNo ratings yet
- Sally Aburumman Bushra SaleemDocument75 pagesSally Aburumman Bushra SaleemAbdulrahman AlsayyedNo ratings yet
- EKG InterpretationDocument63 pagesEKG InterpretationMiriam Cindy MathullaNo ratings yet
- Mechanical and Electrical Events of The Cardiac CycleDocument39 pagesMechanical and Electrical Events of The Cardiac CyclecosedasapereNo ratings yet
- EKG Skill LabDocument61 pagesEKG Skill LabNina Widya NingrumNo ratings yet
- Ecg ProcedureDocument5 pagesEcg ProcedureLungu AdrianNo ratings yet
- ECG For BeginnersDocument61 pagesECG For Beginnersblndffl100% (2)
- ECG DocumentDocument10 pagesECG Document'SheenMarkReal'No ratings yet
- ACLS EKG Rhythms and InterpretationDocument10 pagesACLS EKG Rhythms and Interpretationdonheyzz_02No ratings yet
- Introduction To ECGDocument39 pagesIntroduction To ECGSingey LhendupNo ratings yet
- Kuliah Ekg UnswagatiDocument75 pagesKuliah Ekg UnswagatiiikNo ratings yet
- Electrocardiogram (ECG/EKG) : Jovel Balaba Tangonan InstructorDocument77 pagesElectrocardiogram (ECG/EKG) : Jovel Balaba Tangonan InstructorNecky AlbaciteNo ratings yet
- Normal Sinus RhythmDocument97 pagesNormal Sinus RhythmNatasha LiberisNo ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- Arritmias en El EmbarazoDocument10 pagesArritmias en El EmbarazoJuan Soto FarfanNo ratings yet
- Ucm 439476Document1 pageUcm 439476Fadel BilondatuNo ratings yet
- Degree), Intermittent Degree), or Complete Conduction Failure (3 Degree) - inDocument1 pageDegree), Intermittent Degree), or Complete Conduction Failure (3 Degree) - inLwin Maung Maung ThikeNo ratings yet
- Valvular Heart DiseaseDocument27 pagesValvular Heart DiseaseOwen J. WieseNo ratings yet
- HP 12 Analyzing The Heart With EKG - StudentDocument3 pagesHP 12 Analyzing The Heart With EKG - StudentandrewbardNo ratings yet
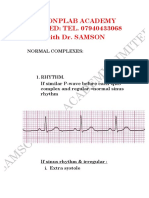
- ECG With DR Samson-1.Document10 pagesECG With DR Samson-1.Ebuwa AmadasunNo ratings yet
- Schedule D: List of Life Saveing or Life Sustaining Medical DevicesDocument5 pagesSchedule D: List of Life Saveing or Life Sustaining Medical DevicesAasma RehmanNo ratings yet
- Cardiac Failure ChiongDocument4 pagesCardiac Failure ChiongJohn Miguel ChiongNo ratings yet
- Chapter 34 Emergency Cardiovascular SystemDocument24 pagesChapter 34 Emergency Cardiovascular SystemDharlyn MungcalNo ratings yet
- ACLS PharmacologyDocument6 pagesACLS PharmacologyEunice Angela Fulgueras80% (5)
- Pulmonary HypertensionDocument1 pagePulmonary HypertensionSa KhunNo ratings yet
- Bedside Approach To Electrocardiography JapyeeDocument188 pagesBedside Approach To Electrocardiography JapyeeRichard MelialaNo ratings yet
- Atrioventricular Spetal Defect Avsd Partial EditDocument2 pagesAtrioventricular Spetal Defect Avsd Partial EditFelicia Shan SugataNo ratings yet
- AHA Guideline NSTEMI 2014 PDFDocument71 pagesAHA Guideline NSTEMI 2014 PDFkiyoeugraNo ratings yet
- 50 Cardiology Pimp Questions - LearntheHeartDocument19 pages50 Cardiology Pimp Questions - LearntheHearttrail 1No ratings yet
- 118 A Chapter 2.1 - RESPONSES TO ALTERED VENTILATORY FUNCTION (CARDIOMYOGRAPHY)Document8 pages118 A Chapter 2.1 - RESPONSES TO ALTERED VENTILATORY FUNCTION (CARDIOMYOGRAPHY)Joanna Taylan100% (1)
- 2 Medicine MCQs NephrologyDocument3 pages2 Medicine MCQs NephrologyDiwakesh C BNo ratings yet
- Ekg BadgebuddyDocument2 pagesEkg BadgebuddyreneecolemanNo ratings yet
- What Causes Glomerular DiseaseDocument5 pagesWhat Causes Glomerular DiseaseAswin AgusNo ratings yet
- Heartbeat Disorders: by Aisha Sara Tasnim Physician: Dr. SsebulibaDocument31 pagesHeartbeat Disorders: by Aisha Sara Tasnim Physician: Dr. SsebulibaNinaNo ratings yet
- Cardiac Glycosides - ScribdDocument12 pagesCardiac Glycosides - ScribdmiznahNo ratings yet
- Cardioversion and DefibrillationDocument15 pagesCardioversion and DefibrillationShalini ChanduNo ratings yet
- CV - Imaging of Heart Disease in Women - Review and Case PresentationDocument30 pagesCV - Imaging of Heart Disease in Women - Review and Case PresentationAndi Wetenri PadaulengNo ratings yet
- Stress Echo Cardiography (63328 - 1)Document18 pagesStress Echo Cardiography (63328 - 1)Griselda Maria Pinto SanchezNo ratings yet
- Rheumatic FeverDocument87 pagesRheumatic FeverFarida Mawaddah Husna100% (1)
- MCQ Cardio 2Document54 pagesMCQ Cardio 2Dian Paramita100% (1)
- Project ProposalDocument4 pagesProject ProposalLesterNo ratings yet
- Utah KidneyDocument16 pagesUtah KidneyChristineGonzalesNo ratings yet
- Acute Heart FailureDocument24 pagesAcute Heart FailureTeddy MauriceNo ratings yet
- Dobutamine Drug StudyDocument1 pageDobutamine Drug Studyzyr2189100% (2)