You might also like
- Cameron 2016Document11 pagesCameron 2016CarmePonsNo ratings yet
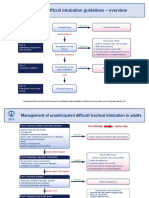
- Difficult Intubation Guidelines OverviewDocument3 pagesDifficult Intubation Guidelines OverviewMaufer AlNo ratings yet
- q1 Social CRMDocument17 pagesq1 Social CRMcésar_campos_45No ratings yet
- Poku2016 Q1Document4 pagesPoku2016 Q1césar_campos_45No ratings yet
- Gru Now 2013Document18 pagesGru Now 2013césar_campos_45No ratings yet
- Aerosales en VM 2015Document8 pagesAerosales en VM 2015césar_campos_45No ratings yet
- VM Prolongada JCC 2015Document7 pagesVM Prolongada JCC 2015césar_campos_45No ratings yet
- Insulinoterapia JCC 2015Document6 pagesInsulinoterapia JCC 2015césar_campos_45No ratings yet
- Aga en Uci 2015Document5 pagesAga en Uci 2015césar_campos_45No ratings yet
- Dar o No Dar Fluidos 2012Document8 pagesDar o No Dar Fluidos 2012césar_campos_45No ratings yet
- VM Seleccionando El Peep Correcto Cocc 2015Document8 pagesVM Seleccionando El Peep Correcto Cocc 2015césar_campos_45No ratings yet
- Hipercapnia, Relevancia Clinica y Mecanismos Cocc 2015Document6 pagesHipercapnia, Relevancia Clinica y Mecanismos Cocc 2015césar_campos_45No ratings yet
- Aki Inducida Por Sepsis Cocc 2014Document8 pagesAki Inducida Por Sepsis Cocc 2014césar_campos_45No ratings yet
- Vili Cocc 2015Document6 pagesVili Cocc 2015césar_campos_45No ratings yet
- Prognosis GuidelinesDocument103 pagesPrognosis GuidelinesPaola MedinaNo ratings yet
- (Inglés) Guía Infusión Insulina para Manejo Hiperglicemia Pctes Críticos (2012)Document26 pages(Inglés) Guía Infusión Insulina para Manejo Hiperglicemia Pctes Críticos (2012)césar_campos_45No ratings yet
- ARDS New Definition - Berlin ConsensusDocument8 pagesARDS New Definition - Berlin ConsensusAndreas IoannouNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Handling Housekeeping RequestsDocument10 pagesHandling Housekeeping RequestsDarlene De PazNo ratings yet
- Pengaruh Latihan Range of Motion (ROM) Ankle Terhadap Pencegahan Terjadinya Neuropati Dan Angiopati Pada Klien Diabetes MelitusDocument7 pagesPengaruh Latihan Range of Motion (ROM) Ankle Terhadap Pencegahan Terjadinya Neuropati Dan Angiopati Pada Klien Diabetes MelitusRafly PrasetyoNo ratings yet
- 4a Rust Preventive OilDocument17 pages4a Rust Preventive OilBalaji DDNo ratings yet
- Name: Muhammad Jazim Reg # L1F20BSCE0024 Subject: English - II Depression in The TeenageDocument2 pagesName: Muhammad Jazim Reg # L1F20BSCE0024 Subject: English - II Depression in The TeenageM jazimNo ratings yet
- Simple ModelsDocument52 pagesSimple ModelsRohan sharmaNo ratings yet
- Subjective:: Decreased Cardiac Output R/T HypertensionDocument3 pagesSubjective:: Decreased Cardiac Output R/T Hypertensionnurse_yramenaj67% (3)
- Gynaecological Ultrasound in Clinical PracticeDocument247 pagesGynaecological Ultrasound in Clinical Practiceyulb_1100% (5)
- FINAL - 15062012 - Dysphagia - Clinical - Guidelines - Web 5Document51 pagesFINAL - 15062012 - Dysphagia - Clinical - Guidelines - Web 5Nathalia Dos ReisNo ratings yet
- Quality and Regulatory Product Information (EMC)Document6 pagesQuality and Regulatory Product Information (EMC)ManuelaNo ratings yet
- Occupational Health, Safety and Wellbeing Strategy 2016-2021Document22 pagesOccupational Health, Safety and Wellbeing Strategy 2016-2021Taufan Arif ZulkarnainNo ratings yet
- Students Readiness For The Face-To-Face Classes in Junior and Senior High SchoolDocument12 pagesStudents Readiness For The Face-To-Face Classes in Junior and Senior High SchoolIJAR JOURNALNo ratings yet
- Thesis Shourya PPT 2 3Document24 pagesThesis Shourya PPT 2 3Y ShouryaNo ratings yet
- Msds Redispersible Polymer Powder RDPDocument8 pagesMsds Redispersible Polymer Powder RDPWANGYUSHENG Kima Chemical Co LtdNo ratings yet
- Monotoring Pathogen-Induced Sickness in Mice and RatsDocument12 pagesMonotoring Pathogen-Induced Sickness in Mice and RatsAntares Basulto NathNo ratings yet
- Biosample Stool Collection Protocol InfantDocument2 pagesBiosample Stool Collection Protocol Infantapi-531349549No ratings yet
- Barber 1961Document12 pagesBarber 1961mariavardehNo ratings yet
- RustagiDocument1 pageRustagiVIrat SamarNo ratings yet
- 2009Document45 pages2009jimmyNo ratings yet
- m6 Endocrine System - Lesson 1 HormonesDocument32 pagesm6 Endocrine System - Lesson 1 HormonesJunimar AggabaoNo ratings yet
- Evolve 5 - Mid Term Test ReviewDocument9 pagesEvolve 5 - Mid Term Test ReviewLaiza Godoy100% (3)
- Da Vinci Si Quick Reference Guide (Maximum Monopolar ESU Power Settings) (551183-01) PDFDocument1 pageDa Vinci Si Quick Reference Guide (Maximum Monopolar ESU Power Settings) (551183-01) PDFJuan RamirezNo ratings yet
- r128216119 - Maria - Millan - CUR128216119 3Document1 pager128216119 - Maria - Millan - CUR128216119 3Millan FamiliaNo ratings yet
- Developing Personal Magnetism Is About Enhancing Your CharismaDocument3 pagesDeveloping Personal Magnetism Is About Enhancing Your CharismafareedNo ratings yet
- Suicide Awareness and PreventionDocument4 pagesSuicide Awareness and PreventionKeerthi RajpurohitNo ratings yet
- Diagnostic Test in TLE 8 - 2nd QuarterDocument31 pagesDiagnostic Test in TLE 8 - 2nd QuarterRowel NillasNo ratings yet
- Dermoscopic Features of Pigmentary Disorders in Indian Skin: A Prospective Observational StudyDocument10 pagesDermoscopic Features of Pigmentary Disorders in Indian Skin: A Prospective Observational StudyIJAR JOURNALNo ratings yet
- Appendix G Site Management Safety Training Scheme (SMSTS)Document16 pagesAppendix G Site Management Safety Training Scheme (SMSTS)dodozeeNo ratings yet
- Various Attachments Used in Prosthodontics-A Review: November 2018Document5 pagesVarious Attachments Used in Prosthodontics-A Review: November 2018harshita parasharNo ratings yet
- Annotated BibliographyDocument9 pagesAnnotated BibliographyKavi rajputNo ratings yet
- A Review On Cosmetology in AyurvedaDocument9 pagesA Review On Cosmetology in AyurvedaCarla Vieira SoaresNo ratings yet