You might also like
- The Successful Treatment of DisinhibitioDocument4 pagesThe Successful Treatment of DisinhibitioVicky NotesNo ratings yet
- Encefalitis Autoinmune 2011 PDFDocument11 pagesEncefalitis Autoinmune 2011 PDFDiana Vanessa SuarezNo ratings yet
- Neuropsychiatric Sequelae of Nipah Virus Encephalitis: MethodsDocument5 pagesNeuropsychiatric Sequelae of Nipah Virus Encephalitis: MethodsTryas YulithaNo ratings yet
- Neurosyphilis Presenting As Psychiatric Symptoms - An Unusual Case ReportDocument3 pagesNeurosyphilis Presenting As Psychiatric Symptoms - An Unusual Case ReportKinga KlimczykNo ratings yet
- Neurosyphilis: The Reemergence of An Historical DiseaseDocument2 pagesNeurosyphilis: The Reemergence of An Historical DiseaseDrashua AshuaNo ratings yet
- Hashimoto's Encephalopathy Case ReportsDocument2 pagesHashimoto's Encephalopathy Case ReportsKantiNareshNo ratings yet
- Encefalitis LimbicaDocument11 pagesEncefalitis LimbicaRandy UlloaNo ratings yet
- 1 Neuro A) IIHDocument3 pages1 Neuro A) IIHLoren boidNo ratings yet
- Osmotic demyelination syndromes: Two case reports of central and extrapontine myelinolysis with normal sodiumDocument5 pagesOsmotic demyelination syndromes: Two case reports of central and extrapontine myelinolysis with normal sodiumNontaphon PiyawattanamethaNo ratings yet
- Neurosyphilis and Organic Psychotic Disorder: A Case Report: Ömer Saatçio Lu, Aysel Kol Ak NC, Ayhan KöksalDocument3 pagesNeurosyphilis and Organic Psychotic Disorder: A Case Report: Ömer Saatçio Lu, Aysel Kol Ak NC, Ayhan KöksalDrashua AshuaNo ratings yet
- 148-Article Text-695-1-10-20180529Document5 pages148-Article Text-695-1-10-20180529fio rentiniNo ratings yet
- Uncovering an Uncommon Cause of PsychosisDocument2 pagesUncovering an Uncommon Cause of PsychosissavinaumarNo ratings yet
- Dementia Due To NeurosyphilisDocument3 pagesDementia Due To NeurosyphilisIOSRjournalNo ratings yet
- Status Epilepticus in Adults: A Study From Nigeria: SciencedirectDocument6 pagesStatus Epilepticus in Adults: A Study From Nigeria: SciencedirectLuther ThengNo ratings yet
- nti-N-Methyl - Aspartate Receptor Encephalitis: Article OutlineDocument7 pagesnti-N-Methyl - Aspartate Receptor Encephalitis: Article OutlineMichelle ImmaculataNo ratings yet
- Case Series: Neuropsychiatric Symptoms With Pediatric Systemic Lupus ErythematosusDocument4 pagesCase Series: Neuropsychiatric Symptoms With Pediatric Systemic Lupus ErythematosusJosue LayedraNo ratings yet
- 1536 FullDocument7 pages1536 FullJosue LayedraNo ratings yet
- The NORSE (New-Onset Refractory Status Epileptic Us) SyndromeDocument4 pagesThe NORSE (New-Onset Refractory Status Epileptic Us) Syndromebenghooi75No ratings yet
- Poster ProceedingsDocument804 pagesPoster Proceedingskhadidja BOUTOUILNo ratings yet
- ACTHIV29Document1 pageACTHIV29Drashua AshuaNo ratings yet
- Cerebral SLE Case Report and Diagnostic Test EvaluationDocument9 pagesCerebral SLE Case Report and Diagnostic Test EvaluationrandyardinalNo ratings yet
- 0717 9227 RCHNP 57 03 0283Document12 pages0717 9227 RCHNP 57 03 0283Araceli PerezNo ratings yet
- Psychiatric Manifestations of NeurosyphilisDocument3 pagesPsychiatric Manifestations of NeurosyphilisDrashua AshuaNo ratings yet
- Delirium: Robyn P. Thom, M.D., Nomi C. Levy-Carrick, M.D., M.Phil., Melissa Bui, M.D., David Silbersweig, M.DDocument9 pagesDelirium: Robyn P. Thom, M.D., Nomi C. Levy-Carrick, M.D., M.Phil., Melissa Bui, M.D., David Silbersweig, M.DfatinNo ratings yet
- Criteria For Diagnosing Disease: Parlunson'sDocument3 pagesCriteria For Diagnosing Disease: Parlunson'sapi-3806049No ratings yet
- "Undifferentiated Schizophrenia" RevisitedDocument2 pages"Undifferentiated Schizophrenia" RevisitedNengLukmanNo ratings yet
- Hant PDFDocument6 pagesHant PDFRodrigo AriasNo ratings yet
- 6-Diagnosis and Treatment of Nonepileptic Seizures.11Document16 pages6-Diagnosis and Treatment of Nonepileptic Seizures.11مجاهد إسماعيل حسن حسينNo ratings yet
- Acute Intermittent Porphyria - Clinicopathologic Correlation - Report of A Case and Review of The Literature (1997)Document7 pagesAcute Intermittent Porphyria - Clinicopathologic Correlation - Report of A Case and Review of The Literature (1997)Triple ANo ratings yet
- Case Report Herpes EncephalitisDocument3 pagesCase Report Herpes EncephalitisAyu WindyaningrumNo ratings yet
- Exercise en Clinical ReasoningDocument4 pagesExercise en Clinical ReasoningFrederico PóvoaNo ratings yet
- 1311 IjirmsDocument4 pages1311 Ijirmsbayekha04No ratings yet
- Farmacologia de Los Medicamentos Antipsicoticos en AmDocument9 pagesFarmacologia de Los Medicamentos Antipsicoticos en AmedgarmoncadaNo ratings yet
- Case ReportDocument5 pagesCase ReportJenesse Kacy GalugaNo ratings yet
- Infectious Dan Autoantibody Associated EncephalitisDocument13 pagesInfectious Dan Autoantibody Associated EncephalitisAyudiah ParamitaNo ratings yet
- Hypertension Induced PsychosisDocument2 pagesHypertension Induced PsychosiscinthyaandiniNo ratings yet
- Uncommon Disorders Masquerading as Acute Flaccid Paralysis in ChildrenDocument7 pagesUncommon Disorders Masquerading as Acute Flaccid Paralysis in ChildrenAnonymous G20oAbl6p8No ratings yet
- Status Epilepticus in AdultsDocument3 pagesStatus Epilepticus in AdultsampalNo ratings yet
- Pons LesionDocument4 pagesPons Lesiontjimen2No ratings yet
- Roberts Psychiatric 1992Document3 pagesRoberts Psychiatric 1992Drashua AshuaNo ratings yet
- Confusion: Muath AlismailDocument22 pagesConfusion: Muath AlismailMuath ASNo ratings yet
- Appi Neuropsych 18010005Document6 pagesAppi Neuropsych 18010005sarahNo ratings yet
- Anti-NMDA-receptor Encephalitis in An Adolescent With HIV Infection and Review of The LiteratureDocument3 pagesAnti-NMDA-receptor Encephalitis in An Adolescent With HIV Infection and Review of The LiteratureJeremy Eckhart S ParhusipNo ratings yet
- Neuroleptic Malignant Syndrome: Kathryn RosenblattDocument12 pagesNeuroleptic Malignant Syndrome: Kathryn RosenblattTroy FengNo ratings yet
- 2012-European Journal of Neurology IMPRIMIR PAGINA 141Document368 pages2012-European Journal of Neurology IMPRIMIR PAGINA 141Francisco A. Villegas-LópezNo ratings yet
- 01 WNL 0000042787 51461 d1Document2 pages01 WNL 0000042787 51461 d1veronikiNo ratings yet
- Paraneoplasic Encephalitis LalDocument13 pagesParaneoplasic Encephalitis Lalkmarmol77No ratings yet
- Ref 7Document12 pagesRef 7Tiago BaraNo ratings yet
- Jurnal ReadingDocument27 pagesJurnal ReadingPatresya LantanNo ratings yet
- Clinical CaseDocument6 pagesClinical Casedani_zurita_1No ratings yet
- Encefalitis NmdaDocument9 pagesEncefalitis Nmdamariafernandasv98No ratings yet
- Case Presentation NewDocument13 pagesCase Presentation Newsherief maroufNo ratings yet
- ng00229 PDFDocument3 pagesng00229 PDFPaijo SusenoNo ratings yet
- 7 Management of Neuropsychiatric Lupus: John G. HanlyDocument23 pages7 Management of Neuropsychiatric Lupus: John G. HanlyNungki TriandariNo ratings yet
- 10 1016@j Semarthrit 2020 12 004Document78 pages10 1016@j Semarthrit 2020 12 004karol castellonNo ratings yet
- Yu 2006Document8 pagesYu 2006Josue LayedraNo ratings yet
- Encephalitis and Aseptic Meningitis: Short-Term and Long-Term Outcome, Quality of Life and Neuropsychological FunctioningDocument9 pagesEncephalitis and Aseptic Meningitis: Short-Term and Long-Term Outcome, Quality of Life and Neuropsychological FunctioningRoberto SoehartonoNo ratings yet
- FHLH 1Document13 pagesFHLH 1habibe koçNo ratings yet
- Posterior Reversible Encephalopathy Syndrome Secondary To Acute Post-Streptococcal Glomerulonephritis in A 12-Year-Old GirlDocument2 pagesPosterior Reversible Encephalopathy Syndrome Secondary To Acute Post-Streptococcal Glomerulonephritis in A 12-Year-Old GirlwawaningNo ratings yet
- Keys CardiologyDocument1 pageKeys CardiologyDrashua AshuaNo ratings yet
- DM CardiologyDocument39 pagesDM CardiologyDrashua AshuaNo ratings yet
- Telephone Directory EngDocument8 pagesTelephone Directory EngDrashua AshuaNo ratings yet
- Bihar PG15 ProspectusDocument37 pagesBihar PG15 ProspectusDrashua AshuaNo ratings yet
- Post Graduate Medical Admission Test (Pgmat) - 2015 For MD/MS/PGD, MDS & MD (Ayurveda)Document2 pagesPost Graduate Medical Admission Test (Pgmat) - 2015 For MD/MS/PGD, MDS & MD (Ayurveda)Drashua AshuaNo ratings yet
- Muscle Origins and InsertionsDocument9 pagesMuscle Origins and Insertionsnoisytaost92% (12)
- Post Graduate Medical Admission Test (Pgmat) - 2014 For MD/MS/PGD, MDS & MD (Ayurveda)Document1 pagePost Graduate Medical Admission Test (Pgmat) - 2014 For MD/MS/PGD, MDS & MD (Ayurveda)Drashua AshuaNo ratings yet
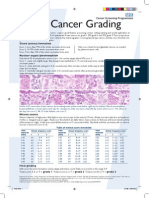
- Breast Cancer Grading PDFDocument1 pageBreast Cancer Grading PDFDrashua AshuaNo ratings yet
- Bence Jones Protein-UrineDocument16 pagesBence Jones Protein-UrineDrashua Ashua100% (2)
- Post Graduate Medical Admission Test (Pgmat) - 2015 For MD/MS/PGD, MDS & MD (Ayurveda)Document2 pagesPost Graduate Medical Admission Test (Pgmat) - 2015 For MD/MS/PGD, MDS & MD (Ayurveda)Drashua AshuaNo ratings yet
- Bio Medical Rules PDFDocument28 pagesBio Medical Rules PDFDrashua AshuaNo ratings yet
- Compliance rate study of bio-medical waste segregationDocument50 pagesCompliance rate study of bio-medical waste segregationAman Dheer Kapoor100% (2)
- ABO in The Context ofDocument21 pagesABO in The Context ofDrashua AshuaNo ratings yet
- CBD FullDocument5 pagesCBD FullDrashua AshuaNo ratings yet
- Hilgendorf Bio 07Document52 pagesHilgendorf Bio 07Drashua AshuaNo ratings yet
- Application PDFDocument2 pagesApplication PDFDrashua AshuaNo ratings yet
- SHIGELLOSISDocument1 pageSHIGELLOSISDrashua AshuaNo ratings yet
- HematologyDocument58 pagesHematologyAchmad DainuriNo ratings yet
- Shigella BackgroundDocument2 pagesShigella BackgroundDrashua AshuaNo ratings yet
- Ecp Shigella InfectionDocument4 pagesEcp Shigella InfectionDrashua AshuaNo ratings yet
- P 133-1430Document11 pagesP 133-1430Drashua AshuaNo ratings yet
- Shigella in Child-Care SettingsDocument2 pagesShigella in Child-Care SettingsDrashua AshuaNo ratings yet
- Shige LLDocument7 pagesShige LLDrashua AshuaNo ratings yet
- ID 20i2.1Document12 pagesID 20i2.1Drashua AshuaNo ratings yet
- 420 079 Guideline ShigellosisDocument7 pages420 079 Guideline ShigellosisDrashua AshuaNo ratings yet
- ShigellaDocument2 pagesShigellaDrashua AshuaNo ratings yet
- P 133-1430Document11 pagesP 133-1430Drashua AshuaNo ratings yet
- Shigellosis: Frequently Asked QuestionsDocument2 pagesShigellosis: Frequently Asked QuestionsDrashua AshuaNo ratings yet
- ShigellaDocument1 pageShigellaDrashua AshuaNo ratings yet
- 0314Document6 pages0314Drashua AshuaNo ratings yet
- Case Study - EmphysemaDocument6 pagesCase Study - Emphysemamackie_041992No ratings yet
- Poster Ramesh MMDocument5 pagesPoster Ramesh MMRameshKrishnanNo ratings yet
- Amyotrophic Lateral SclerosisDocument2 pagesAmyotrophic Lateral SclerosisJrBong SemaneroNo ratings yet
- Personality DisordersDocument43 pagesPersonality DisordersJeanette Klaber100% (2)
- Understanding Toxic Goiter and Its Nursing CareDocument22 pagesUnderstanding Toxic Goiter and Its Nursing CareJohn Matley Caampued100% (2)
- Emergency visits and readmissions after bariatric surgeryDocument7 pagesEmergency visits and readmissions after bariatric surgerylicgenaroNo ratings yet
- Sciences Basic To PsychiatryDocument2 pagesSciences Basic To Psychiatrynisha chauhanNo ratings yet
- Caries Risk AssessmentDocument33 pagesCaries Risk AssessmentSomya Jain100% (1)
- CB Inf HaematinicsDocument4 pagesCB Inf Haematinicsbassam alharaziNo ratings yet
- University of Delaware College of Health and Nursing Sciences - Hepatitis B Vaccine Declination Form Students)Document2 pagesUniversity of Delaware College of Health and Nursing Sciences - Hepatitis B Vaccine Declination Form Students)DonnaNo ratings yet
- Feeding and Eating Disorders GuideDocument42 pagesFeeding and Eating Disorders GuideCharlaine BacasnoNo ratings yet
- NCM 112 Rle: A Case Study On: Typhoid FeverDocument17 pagesNCM 112 Rle: A Case Study On: Typhoid FeverMadelyn Serneo100% (1)
- Drugs requiring loading dosesDocument1 pageDrugs requiring loading dosesandirio7486No ratings yet
- Ohio Voter Rights CoalitionDocument19 pagesOhio Voter Rights CoalitionsrichardsonNo ratings yet
- Advia 2120i Hematology SystemDocument8 pagesAdvia 2120i Hematology SystemDwitaRiadiniNo ratings yet
- Rotator Cuff Injuries: Symptoms, Causes and TreatmentDocument2 pagesRotator Cuff Injuries: Symptoms, Causes and TreatmentMinnie Hubalde-LoprettiNo ratings yet
- Pathway GGKDocument1 pagePathway GGKVieocta Apsari ParadiseNo ratings yet
- Typhoid Fever PathophysiologyDocument1 pageTyphoid Fever PathophysiologyJim Christian EllaserNo ratings yet
- I-3 Pediatric and Adolescent GynecologyDocument8 pagesI-3 Pediatric and Adolescent GynecologyuvioscribdNo ratings yet
- Uterine Rupture and Cervical TearDocument16 pagesUterine Rupture and Cervical Tearsangita patil0% (1)
- Laser SafetyDocument3 pagesLaser SafetyEbaa BarghouthiNo ratings yet
- Mendelson's SyndromeDocument17 pagesMendelson's SyndromeYuvetha IndranNo ratings yet
- Malaria in Children: Department of Paediatrics and Child Health, Mbarara UniversityDocument13 pagesMalaria in Children: Department of Paediatrics and Child Health, Mbarara UniversityMwanja MosesNo ratings yet
- Inventaris IGD 2022 TerbaruDocument5 pagesInventaris IGD 2022 TerbaruEryNo ratings yet
- Chapter 3 Rationality of DrugsDocument56 pagesChapter 3 Rationality of DrugsS.Srinivasan ('Chinu'); Renu KhannaNo ratings yet
- Coding Case StudiesDocument2 pagesCoding Case Studiesapi-385484216100% (1)
- Tugas Baca Jurnal BT ShuntDocument53 pagesTugas Baca Jurnal BT ShuntVashNo ratings yet
- Common Peroneal Nerve: AnatomyDocument13 pagesCommon Peroneal Nerve: AnatomySitti Maryam AmiliNo ratings yet
- Referral System in IndiaDocument24 pagesReferral System in IndiaKailash Nagar100% (1)
- Extrahepatic Biliary AtresiaDocument3 pagesExtrahepatic Biliary AtresiaTiti Afrianto100% (1)