You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Cases CX CarcinomaDocument2 pagesCases CX Carcinomadgina8800No ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Rush Echo Massive Air EmbolismDocument3 pagesRush Echo Massive Air Embolismdgina8800No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Target Marketing: Target Marketing Is "The Process of Identifying Market Segments, Selecting OneDocument7 pagesTarget Marketing: Target Marketing Is "The Process of Identifying Market Segments, Selecting Onedgina8800No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- 44 Traditional Medicine FINALDocument72 pages44 Traditional Medicine FINALdgina8800No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Echocardiography AdvanceDocument8 pagesEchocardiography Advancedgina88000% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- E Learn CAE - ICCU - LoRes PDFDocument8 pagesE Learn CAE - ICCU - LoRes PDFdgina8800No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- 4 Print Form Cardiac - USDocument1 page4 Print Form Cardiac - USdgina8800No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Echo Case Ao RegurgDocument3 pagesEcho Case Ao Regurgdgina8800No ratings yet
- 4P Fellowship Pros & Cons & Focus On Ultrasound Fellowship GaspariDocument5 pages4P Fellowship Pros & Cons & Focus On Ultrasound Fellowship Gasparidgina8800No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- New Brochure FTTE 11-2-2010Document4 pagesNew Brochure FTTE 11-2-2010dgina8800No ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Standardized Echo Report Rev1Document38 pagesStandardized Echo Report Rev1dgina8800100% (1)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Medical Terminology On CPC Exam2 - YouTubeDocument2 pagesMedical Terminology On CPC Exam2 - YouTubedgina8800No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- A FEEL@Chelmers Flyer 02 14Document1 pageA FEEL@Chelmers Flyer 02 14dgina8800No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Ocr Graphics Gcse CourseworkDocument6 pagesOcr Graphics Gcse Courseworkzys0vemap0m3100% (2)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- A Study On Mistakes and Errors in Consecutive Interpretation From Vietnamese To English. Dang Huu Chinh. Qhf.1Document38 pagesA Study On Mistakes and Errors in Consecutive Interpretation From Vietnamese To English. Dang Huu Chinh. Qhf.1Kavic100% (2)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Ant Colony AlgorithmDocument11 pagesAnt Colony Algorithmjaved765No ratings yet
- B2 First Unit 11 Test: Section 1: Vocabulary Section 2: GrammarDocument1 pageB2 First Unit 11 Test: Section 1: Vocabulary Section 2: GrammarNatalia KhaletskaNo ratings yet
- India Internet Goldman SachsDocument86 pagesIndia Internet Goldman SachsTaranjeet SinghNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- SDLC Review ChecklistDocument4 pagesSDLC Review Checklistmayank govilNo ratings yet
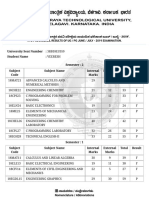
- VTU Result PDFDocument2 pagesVTU Result PDFVaibhavNo ratings yet
- Kepimpinan BerwawasanDocument18 pagesKepimpinan BerwawasanandrewanumNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- 3723 Modernizing HR at Microsoft BCSDocument14 pages3723 Modernizing HR at Microsoft BCSYaseen SaleemNo ratings yet
- NCLEX 20QUESTIONS 20safety 20and 20infection 20controlDocument8 pagesNCLEX 20QUESTIONS 20safety 20and 20infection 20controlCassey MillanNo ratings yet
- Paleontology 1Document6 pagesPaleontology 1Avinash UpadhyayNo ratings yet
- Tate J. Hedtke SPED 608 Assignment #6 Standard # 8 Cross Categorical Special Education/ Learning Disabilities Artifact SummaryDocument5 pagesTate J. Hedtke SPED 608 Assignment #6 Standard # 8 Cross Categorical Special Education/ Learning Disabilities Artifact Summaryapi-344731850No ratings yet
- Local Anesthesia For The Dental Hygienist 2nd Edition Logothetis Test BankDocument12 pagesLocal Anesthesia For The Dental Hygienist 2nd Edition Logothetis Test BankJessicaPorterfqmei100% (18)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Schmitt Allik 2005 ISDP Self Esteem - 000 PDFDocument20 pagesSchmitt Allik 2005 ISDP Self Esteem - 000 PDFMariana KapetanidouNo ratings yet
- Visual Impairments in Young Children: Fundamentals of and Strategies For Enhancing DevelopmentDocument13 pagesVisual Impairments in Young Children: Fundamentals of and Strategies For Enhancing Developmentfadil ahmadiNo ratings yet
- Superscope, Inc. v. Brookline Corp., Etc., Robert E. Lockwood, 715 F.2d 701, 1st Cir. (1983)Document3 pagesSuperscope, Inc. v. Brookline Corp., Etc., Robert E. Lockwood, 715 F.2d 701, 1st Cir. (1983)Scribd Government DocsNo ratings yet
- MathTextbooks9 12Document64 pagesMathTextbooks9 12Andrew0% (1)
- ECON266 Worksheet 8Document4 pagesECON266 Worksheet 8Oi OuNo ratings yet
- Operations Management and Operations PerformanceDocument59 pagesOperations Management and Operations PerformancePauline LagtoNo ratings yet
- Top Websites Ranking - Most Visited Websites in May 2023 - SimilarwebDocument3 pagesTop Websites Ranking - Most Visited Websites in May 2023 - SimilarwebmullahNo ratings yet
- BattleRope Ebook FinalDocument38 pagesBattleRope Ebook FinalAnthony Dinicolantonio100% (1)
- Unilateral Lower Limb SwellingDocument1 pageUnilateral Lower Limb SwellingLilius TangNo ratings yet
- Evaluation of The Performance of HRCT in The Diagnostic and Management of Covid-19Document7 pagesEvaluation of The Performance of HRCT in The Diagnostic and Management of Covid-19IJAR JOURNALNo ratings yet
- Ais Activiy Chapter 5 PDFDocument4 pagesAis Activiy Chapter 5 PDFAB CloydNo ratings yet
- Adobe Voice Assessment Tool-FinalDocument1 pageAdobe Voice Assessment Tool-Finalapi-268484302No ratings yet
- WaveDocument1 pageWavejimbieNo ratings yet
- U6 - S7 - Trabajo Individual 7 - Ficha de Aplicación INGLES 3Document2 pagesU6 - S7 - Trabajo Individual 7 - Ficha de Aplicación INGLES 3Antonio Andres Duffoo MarroquinNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- OITE - MCQ S QuestionsFinal2011Document67 pagesOITE - MCQ S QuestionsFinal2011KatKut99100% (7)
- FSR 2017-2018 KNL CircleDocument136 pagesFSR 2017-2018 KNL CircleparthaNo ratings yet
- Observation: Student: Liliia Dziuda Date: 17/03/21 Topic: Movie Review Focus: Writing SkillsDocument2 pagesObservation: Student: Liliia Dziuda Date: 17/03/21 Topic: Movie Review Focus: Writing SkillsLiliaNo ratings yet
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)