You might also like
- Donordarah PDFDocument1 pageDonordarah PDFjo_jo_maniaNo ratings yet
- Efficacy and Safety of Tigecycline - A Systematic Review and Meta-AnalysisDocument8 pagesEfficacy and Safety of Tigecycline - A Systematic Review and Meta-Analysisjo_jo_maniaNo ratings yet
- Canadian Contraception ConsensusDocument14 pagesCanadian Contraception Consensusjo_jo_maniaNo ratings yet
- Case Report: Pulmonary Sequestration: A Case Report and Literature ReviewDocument4 pagesCase Report: Pulmonary Sequestration: A Case Report and Literature Reviewjo_jo_maniaNo ratings yet
- 111992518Document6 pages111992518jo_jo_maniaNo ratings yet
- Dystocia SOGCDocument16 pagesDystocia SOGCAdhitia NugrahantoNo ratings yet
- Bioethic MetaphysicDocument6 pagesBioethic Metaphysicjo_jo_maniaNo ratings yet
- ContentServer 37.ASPaaaaaDocument6 pagesContentServer 37.ASPaaaaaAchmad Deza FaristaNo ratings yet
- Donor DarahDocument1 pageDonor Darahjo_jo_maniaNo ratings yet
- Chlamydial Infection Can Cause Disease in Many Organ SystemsDocument22 pagesChlamydial Infection Can Cause Disease in Many Organ Systemsjo_jo_maniaNo ratings yet
- Case Studies Module 1 - A Case of PcosDocument9 pagesCase Studies Module 1 - A Case of PcosBobNo ratings yet
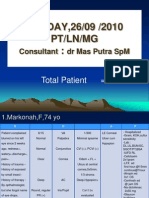
- Sunday, 26/09 /2010 PT/LN/MG:: Consultant DR Mas Putra SPMDocument6 pagesSunday, 26/09 /2010 PT/LN/MG:: Consultant DR Mas Putra SPMjo_jo_maniaNo ratings yet
- AnyelirDocument2 pagesAnyelirjo_jo_maniaNo ratings yet
- Structure Content: 1. EXERCISE 1 (Skill 1-2) 2. Toefl Review Exercise (Skill 1-2) 3. Answer KeysDocument3 pagesStructure Content: 1. EXERCISE 1 (Skill 1-2) 2. Toefl Review Exercise (Skill 1-2) 3. Answer Keysjo_jo_mania0% (1)
- IBT Q4 03 ReadingonlyDocument1 pageIBT Q4 03 Readingonlyjo_jo_maniaNo ratings yet
- HiResOligonucleoutide ACGH Analysis Under24Hrs AppNote5991-0643ENDocument8 pagesHiResOligonucleoutide ACGH Analysis Under24Hrs AppNote5991-0643ENjo_jo_maniaNo ratings yet
- Yg Belum Masuk IpadDocument1 pageYg Belum Masuk Ipadjo_jo_maniaNo ratings yet
- Induction of Labour Versus Expectant Monitoring ForDocument11 pagesInduction of Labour Versus Expectant Monitoring Forjo_jo_maniaNo ratings yet
- BARUPoliklinik Wangaya 4-8 Juli 2011Document14 pagesBARUPoliklinik Wangaya 4-8 Juli 2011jo_jo_maniaNo ratings yet
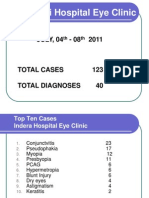
- NEW Weekly Indra 04-08 July 2011Document13 pagesNEW Weekly Indra 04-08 July 2011jo_jo_maniaNo ratings yet
- International Centre For Eye Health Teaching Set 2 The Eye in Primary Health CareDocument25 pagesInternational Centre For Eye Health Teaching Set 2 The Eye in Primary Health Carejo_jo_maniaNo ratings yet
- TOEFL Speaking - Question 1&2 TopicsDocument8 pagesTOEFL Speaking - Question 1&2 TopicsSiddharthaSidNo ratings yet
- Cancer RiskDocument1 pageCancer Riskjo_jo_maniaNo ratings yet
- Prediction Reccurence Prostat CADocument9 pagesPrediction Reccurence Prostat CAjo_jo_maniaNo ratings yet
- OrtoDocument61 pagesOrtojo_jo_maniaNo ratings yet
- Arterial Blood Gas: DR - Made Widia, Sp.A (K)Document19 pagesArterial Blood Gas: DR - Made Widia, Sp.A (K)jo_jo_mania100% (1)
- Laser Iridotomy and GlaucomaDocument2 pagesLaser Iridotomy and Glaucomajo_jo_maniaNo ratings yet
- Migraine Prophylaxis: Pharmacotherapy PerspectivesDocument11 pagesMigraine Prophylaxis: Pharmacotherapy Perspectivesjo_jo_maniaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Corrode Four Horsemen Book 3 by SarahDocument323 pagesCorrode Four Horsemen Book 3 by SarahSaoirse ZherineNo ratings yet
- Daphne Goodsby - Before Another Tragedy Strikes-Address Bullying in Our SchoolsDocument4 pagesDaphne Goodsby - Before Another Tragedy Strikes-Address Bullying in Our Schoolsapi-327329006No ratings yet
- Lesson Plan: Learning OutcomesDocument4 pagesLesson Plan: Learning OutcomesJoshua AgucoyNo ratings yet
- Summary New Black Beauty Level 2Document23 pagesSummary New Black Beauty Level 2merinaNo ratings yet
- Ergonomic Risk Identification and Assessment - Identification and Assessment ToolDocument54 pagesErgonomic Risk Identification and Assessment - Identification and Assessment Toolhitm357No ratings yet
- Breech PresentationDocument85 pagesBreech Presentationwidya vannesaNo ratings yet
- Art of Fitness BrochureDocument62 pagesArt of Fitness Brochureprotein47No ratings yet
- Toolbox Talk Chemical GlovesDocument6 pagesToolbox Talk Chemical GlovesBomber Man100% (1)
- Wrist Anatomy and Surgical Approaches: Roy Cardoso, MD, Robert M. Szabo, MD, MPHDocument22 pagesWrist Anatomy and Surgical Approaches: Roy Cardoso, MD, Robert M. Szabo, MD, MPHMd Ahsanuzzaman PinkuNo ratings yet
- Plexo BraquialDocument26 pagesPlexo BraquialXavier RiveraNo ratings yet
- Epov EclipseDocument12 pagesEpov EclipseShivani JaiswalNo ratings yet
- Investigation of An Animal Mutilation Injuries in Cache County, UtahDocument33 pagesInvestigation of An Animal Mutilation Injuries in Cache County, UtahLionel Elyansun100% (1)
- New Power Cabinet Installation ManualDocument59 pagesNew Power Cabinet Installation ManualHerianto UntasNo ratings yet
- Jeopardy CPRDocument51 pagesJeopardy CPRapi-273870175No ratings yet
- Lec 11 UL Forarm Anterior CompartmentDocument32 pagesLec 11 UL Forarm Anterior CompartmenthusseinNo ratings yet
- What Are The Benefits of Chiropractic CareDocument2 pagesWhat Are The Benefits of Chiropractic CaretomNo ratings yet
- MRI REPORT OF LEFT KNEE (Tushar Singh)Document2 pagesMRI REPORT OF LEFT KNEE (Tushar Singh)Tushar SinghNo ratings yet
- Kinesiotaping TechniquesDocument26 pagesKinesiotaping TechniquesSuhana hidayat100% (1)
- Dtx10 SDocument60 pagesDtx10 Sлюбовь инжинирингNo ratings yet
- Ecto-Meso-Endo-Dermal LayersDocument3 pagesEcto-Meso-Endo-Dermal LayersCarissa NicholsNo ratings yet
- Risk Assessment - Window and Glass Partition InstallationDocument4 pagesRisk Assessment - Window and Glass Partition Installationburak80% (5)
- LungeDocument6 pagesLungeKaiNo ratings yet
- Iotn Training SlidesDocument38 pagesIotn Training SlidesAchini LiyanageNo ratings yet
- ATI Radially-Compliant Robotic Deburring Tools Flexdeburr™: Installation and Operation ManualDocument28 pagesATI Radially-Compliant Robotic Deburring Tools Flexdeburr™: Installation and Operation ManualAndrei JilaNo ratings yet
- 100 Opthalmology Questions For PracticeDocument37 pages100 Opthalmology Questions For Practicekyonaboy85% (13)
- SkullmethodDocument3 pagesSkullmethodJoeriz BartolomeNo ratings yet
- Assessment (1) Diagnosis: LT Knee OsteoarthritisDocument13 pagesAssessment (1) Diagnosis: LT Knee OsteoarthritisDounia A OdehNo ratings yet
- The Americans 1x01 - Pilot PDFDocument75 pagesThe Americans 1x01 - Pilot PDFDaniel GreenspanNo ratings yet
- NCLEX - Review (6514)Document51 pagesNCLEX - Review (6514)whereswaldo007yahooc100% (1)
- Panch Tantra Stories Part TwoDocument144 pagesPanch Tantra Stories Part TwoKrupal VithlaniNo ratings yet