You might also like
- Assignment On Pharamcological Aspects - BY KAMINI2Document9 pagesAssignment On Pharamcological Aspects - BY KAMINI2kamini ChoudharyNo ratings yet
- Complete Community Course Plan 2nd YearDocument6 pagesComplete Community Course Plan 2nd YearBabita DhruwNo ratings yet
- A Study To Evaluate The Effectiveness of Massaging of Foot On The Level of Pain Among Post-Operative Patient at Selected Hospital of BadamiDocument4 pagesA Study To Evaluate The Effectiveness of Massaging of Foot On The Level of Pain Among Post-Operative Patient at Selected Hospital of BadamiInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Shift Work Disorder and Associated Health Problems Among Nursing Staffs Working in A Tertiary Health Centre, Chennai, South IndiaDocument4 pagesShift Work Disorder and Associated Health Problems Among Nursing Staffs Working in A Tertiary Health Centre, Chennai, South IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cardiovascular System Diseases Part 2Document9 pagesCardiovascular System Diseases Part 2Prince Rener Velasco PeraNo ratings yet
- BSC Nursing Syllabus First YearDocument22 pagesBSC Nursing Syllabus First YearDiksha chaudharyNo ratings yet
- Seminar On Hemorrhage and ShockDocument6 pagesSeminar On Hemorrhage and ShockparmeshoriNo ratings yet
- Everything You Need to Know About Lung AbscessDocument46 pagesEverything You Need to Know About Lung AbscessJeevitha VanithaNo ratings yet
- Effectiveness of simulation-based CPR learning among studentsDocument29 pagesEffectiveness of simulation-based CPR learning among studentsenam professorNo ratings yet
- Esophageal CancerDocument25 pagesEsophageal CancerK poojithaNo ratings yet
- CP Head InjuryDocument9 pagesCP Head InjurySindhu S NairNo ratings yet
- Tamilnadu Nurses Council Inspection ReportDocument43 pagesTamilnadu Nurses Council Inspection ReportchrisNo ratings yet
- ENT Nursing Care GuideDocument32 pagesENT Nursing Care GuideabdulNo ratings yet
- Effectiveness of Structured Teaching Programme On Knowledge Regarding Acid Peptic Disease and Its Prevention Among The Industrial WorkersDocument6 pagesEffectiveness of Structured Teaching Programme On Knowledge Regarding Acid Peptic Disease and Its Prevention Among The Industrial WorkersIJAR JOURNALNo ratings yet
- Syllabus BSC SemesterDocument238 pagesSyllabus BSC SemesterRAMZAAN EDUCATIONNo ratings yet
- Recognize and Manage Common Pediatric Cardiac EmergenciesDocument73 pagesRecognize and Manage Common Pediatric Cardiac EmergenciesKristine CaringalNo ratings yet
- GERIATRIC CONSIDERATIONS IN NURSINGDocument70 pagesGERIATRIC CONSIDERATIONS IN NURSINGsanthiyasandy100% (1)
- Treatment Aspects in Perioperative NursingDocument51 pagesTreatment Aspects in Perioperative NursingShibin Jacob100% (2)
- A Study To Assess The Effectiveness of Foot Massage On The Level of Pain Among Post-Operative Patients at Dhanush Hospital BagalkotDocument7 pagesA Study To Assess The Effectiveness of Foot Massage On The Level of Pain Among Post-Operative Patients at Dhanush Hospital BagalkotInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- SodaPDF-converted-lesson Plan of Cervical Cancer For ResearchDocument54 pagesSodaPDF-converted-lesson Plan of Cervical Cancer For ResearchPatel KrimaNo ratings yet
- JG College of Nursing: Sub: Medical-Surgical NursingDocument33 pagesJG College of Nursing: Sub: Medical-Surgical NursingmilcahNo ratings yet
- Case Study About: Cardiac Failure and Pulmonary EdemaDocument32 pagesCase Study About: Cardiac Failure and Pulmonary EdemaIan Simon DorojaNo ratings yet
- Diagnosi S: MalariaDocument28 pagesDiagnosi S: MalariaOm Prakash SinghNo ratings yet
- Pooja FinalDocument35 pagesPooja FinalSagar ChiplunkarNo ratings yet
- Nephro Case StudyDocument26 pagesNephro Case Studyanimesh pandaNo ratings yet
- Cardiomyopathy SeminarDocument17 pagesCardiomyopathy SeminarJyoti SinghNo ratings yet
- Arterial Blood Gas (Abg) Analysis: Submitted ToDocument5 pagesArterial Blood Gas (Abg) Analysis: Submitted ToRumela ChakrabortyNo ratings yet
- Lesson Plan of BurnsDocument24 pagesLesson Plan of BurnsjrkedridgemwanakalandoNo ratings yet
- Lesson Plan Catheter Toilet.Document7 pagesLesson Plan Catheter Toilet.Miriward Zimba0% (1)
- Oxygen TherapyDocument3 pagesOxygen TherapyKristina PingolNo ratings yet
- Diabetic NephropathyDocument49 pagesDiabetic NephropathyDhanya Raghu100% (1)
- Hypertension: Mayur BV BPH 3 Semester PSPHDocument29 pagesHypertension: Mayur BV BPH 3 Semester PSPHBijay Kumar MahatoNo ratings yet
- Varicose VainsDocument28 pagesVaricose Vainssingireddi1revathiNo ratings yet
- Lesson Plan BMA&BDocument14 pagesLesson Plan BMA&BLoma Waghmare (Jadhav)No ratings yet
- Nursing care plan assessment, diagnosis, planning, implementation and evaluationDocument7 pagesNursing care plan assessment, diagnosis, planning, implementation and evaluationshweta singhNo ratings yet
- Assignment On Burns 2Document15 pagesAssignment On Burns 2Suby Beigh100% (2)
- Case Study 2Document37 pagesCase Study 2api-391842100No ratings yet
- Laryngeal Cancer Powerpoint FinalllllDocument30 pagesLaryngeal Cancer Powerpoint Finalllllapi-396575125No ratings yet
- Adrenal Crisis FinalDocument10 pagesAdrenal Crisis FinalAmanda Scarlet100% (1)
- Pacemaker ImplantationDocument17 pagesPacemaker ImplantationKaku ManishaNo ratings yet
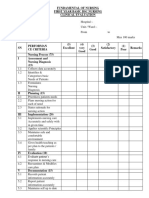
- Evaluation FormatDocument4 pagesEvaluation FormatKinjal VasavaNo ratings yet
- Case Presentation On Parkinsonism 4th YearDocument27 pagesCase Presentation On Parkinsonism 4th YearArchanaNo ratings yet
- Thrombolytic TherapyDocument37 pagesThrombolytic TherapySani sunilNo ratings yet
- Clinical Teaching On Neurological AssessmentDocument18 pagesClinical Teaching On Neurological AssessmentFiyas BiNo ratings yet
- NCP On TuberculosisDocument23 pagesNCP On TuberculosisPreeti ChouhanNo ratings yet
- Transurethral Resection of the Prostate (TURP) ExplainedDocument23 pagesTransurethral Resection of the Prostate (TURP) ExplainedColeen Comelle HuertoNo ratings yet
- Tracheostomy care guideDocument1 pageTracheostomy care guideDudil GoatNo ratings yet
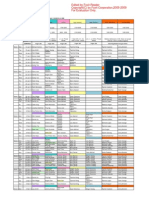
- Medical Surgical Nursing Course PlanDocument10 pagesMedical Surgical Nursing Course PlanRanjana SharmaNo ratings yet
- Artikel PTSS 10 QuestionnaireDocument17 pagesArtikel PTSS 10 QuestionnaireTELEPSIHIJATARNo ratings yet
- Nephrotic SyndromeDocument28 pagesNephrotic Syndromerupali khillareNo ratings yet
- MSC (N) SyllabusDocument246 pagesMSC (N) SyllabussabeethuNo ratings yet
- Procedure On Abdominal ParacentsisDocument22 pagesProcedure On Abdominal ParacentsisBhawna JoshiNo ratings yet
- Time Specific Objective Content Teaching Learning Activities Evaluati ONDocument20 pagesTime Specific Objective Content Teaching Learning Activities Evaluati ONAnnette BainesNo ratings yet
- Biophysiologic MeasuresDocument1 pageBiophysiologic MeasuresEdgar ElgortNo ratings yet
- Intestinal obstruction presentation summaryDocument10 pagesIntestinal obstruction presentation summaryAmlan jyoti thanapatiNo ratings yet
- Betty Neuman'S Theory: Introduction About TheoristDocument11 pagesBetty Neuman'S Theory: Introduction About TheoristRenita ChrisNo ratings yet
- Disorders of AortaDocument25 pagesDisorders of Aortavani reddyNo ratings yet
- Remember: Goals and Plan of Care Should Be Base According To Client's Problems/needs NOT According To Your OwnDocument11 pagesRemember: Goals and Plan of Care Should Be Base According To Client's Problems/needs NOT According To Your Ownavinash dhameriyaNo ratings yet
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- MelanomaDocument10 pagesMelanomaYhr YhNo ratings yet
- NetBank - TransactionsDocument1 pageNetBank - TransactionsYhr YhNo ratings yet
- The Pale Yellow in The Aorta Are The Earliest Lesion of AtherosclerosisDocument1 pageThe Pale Yellow in The Aorta Are The Earliest Lesion of AtherosclerosisYhr YhNo ratings yet
- O LiguriaDocument50 pagesO LiguriaYhr YhNo ratings yet
- Pathophysio of Coronary Artery DiseaseDocument9 pagesPathophysio of Coronary Artery DiseaseYhr YhNo ratings yet
- Crash LogDocument1 pageCrash Log陳邦立No ratings yet
- Pathophysio of Peripheral Vascular DiseaseDocument13 pagesPathophysio of Peripheral Vascular DiseaseYhr YhNo ratings yet
- Robin Goh Completes Hand Hygiene Training CertificateDocument1 pageRobin Goh Completes Hand Hygiene Training CertificateYhr YhNo ratings yet
- Pathophysio of Heart FailureDocument10 pagesPathophysio of Heart FailureYhr YhNo ratings yet
- Pathophysiology of Myocardial InfarctionDocument4 pagesPathophysiology of Myocardial InfarctionYhr YhNo ratings yet
- InsulinDocument1 pageInsulinYhr YhNo ratings yet
- Hyperlipidaemias (MRCP+ Step 1)Document2 pagesHyperlipidaemias (MRCP+ Step 1)Yhr YhNo ratings yet
- Bets - DunningrDocument5 pagesBets - DunningrYhr YhNo ratings yet
- ReadmeDocument3 pagesReadmeQuimolki Figueroa DurandNo ratings yet
- Bets - DunningrDocument5 pagesBets - DunningrYhr YhNo ratings yet
- Bets - DunningrDocument5 pagesBets - DunningrYhr YhNo ratings yet
- Bets - DunningrDocument5 pagesBets - DunningrYhr YhNo ratings yet
- Bets - DunningrDocument5 pagesBets - DunningrYhr YhNo ratings yet
- JVPDocument5 pagesJVPYhr YhNo ratings yet
- Feasibidlity For AustraliaDocument13 pagesFeasibidlity For AustraliaYhr YhNo ratings yet
- Feasibidlity For AustraliaDocument13 pagesFeasibidlity For AustraliaYhr YhNo ratings yet
- Reviewer's Report Title: Cutaneous Squamous Cell Carcinoma Metastatic To Parotid - Analysis ofDocument2 pagesReviewer's Report Title: Cutaneous Squamous Cell Carcinoma Metastatic To Parotid - Analysis ofYhr YhNo ratings yet
- Intern Term 2 2013Document9 pagesIntern Term 2 2013Yhr YhNo ratings yet
- CCCCDocument1 pageCCCCYhr YhNo ratings yet
- Staff Parking & Vehicle Cdetails FormDocument2 pagesStaff Parking & Vehicle Cdetails FormYhr YhNo ratings yet
- AHO Summary Published 11022013Document2 pagesAHO Summary Published 11022013Yhr YhNo ratings yet
- CP 111Document246 pagesCP 111Yhr YhNo ratings yet
- Orientation - Booklet DeclarationDocument1 pageOrientation - Booklet DeclarationYhr YhNo ratings yet
- Feasibidlity For AustraliaDocument13 pagesFeasibidlity For AustraliaYhr YhNo ratings yet
- ECG Fast and Easy PPDocument38 pagesECG Fast and Easy PPTara McNeillNo ratings yet
- Pacemakers & Implantable Cardioverter-Defibrillators (Icds) - Anaesthesia Tutorial of The Week 299 25 November 2013Document8 pagesPacemakers & Implantable Cardioverter-Defibrillators (Icds) - Anaesthesia Tutorial of The Week 299 25 November 2013Anup SasalattiNo ratings yet
- ST JudeDocument10 pagesST JudeLanguage in PhoneticsNo ratings yet
- Dysrhythmias ChartDocument6 pagesDysrhythmias Chartjkrix100% (1)
- ARRHYTHMIADocument25 pagesARRHYTHMIAAsma MuhammadiNo ratings yet
- Cardiovascular Physiology For University Students: S. I. Ogungbemi Department of Physiology University of LagosDocument136 pagesCardiovascular Physiology For University Students: S. I. Ogungbemi Department of Physiology University of LagosTeeNo ratings yet
- Dysrhythmias Nursing InterventionsDocument7 pagesDysrhythmias Nursing InterventionsGail Lian Santos100% (1)
- Ecg Mcqs - Aippg ForumDocument19 pagesEcg Mcqs - Aippg Forumbmhsh100% (1)
- Teaching Cardiac Arrhythmias A Focus On PathophysiDocument10 pagesTeaching Cardiac Arrhythmias A Focus On PathophysiJoao FonsecaNo ratings yet
- DR Yassir Javaid Interpreting The 12 Lead ECGDocument28 pagesDR Yassir Javaid Interpreting The 12 Lead ECGTirtha TaposhNo ratings yet
- ECG Arrhythmia Classification GuideDocument6 pagesECG Arrhythmia Classification GuideEzzat SalemNo ratings yet
- Heart BlockDocument10 pagesHeart BlockEköw Santiago JavierNo ratings yet
- EcgDocument86 pagesEcgHidayatul ゆきNo ratings yet
- Understanding Arrhythmia: Irregular Heartbeat Causes and TypesDocument17 pagesUnderstanding Arrhythmia: Irregular Heartbeat Causes and TypesMaham SaleemNo ratings yet
- Heart BlocksDocument20 pagesHeart BlocksGhaida AlshehriNo ratings yet
- Normal Sinus RhythmDocument97 pagesNormal Sinus RhythmNatasha LiberisNo ratings yet
- ECG Interpretation SkillsDocument46 pagesECG Interpretation SkillsSumeet TripathiNo ratings yet
- Contec Ms400 User Manual EngDocument28 pagesContec Ms400 User Manual EngLeonardo Quevedo100% (1)
- Cardiac Implantable Electronic DevicesDocument49 pagesCardiac Implantable Electronic DevicespriyathasanNo ratings yet
- Rhythm EKG Rate (BPM) Rhythm EKG InterventionsDocument6 pagesRhythm EKG Rate (BPM) Rhythm EKG InterventionsRawabi rawabi1997No ratings yet
- ECG Quiz: Test Your Heart Rhythm Knowledge in 17 QuestionsDocument9 pagesECG Quiz: Test Your Heart Rhythm Knowledge in 17 Questionsamol dahiphaleNo ratings yet
- Anaesthetic Management of Emergency LSCS, An Unusual Case of Complete Heart Block With Permanent Pace MakerDocument2 pagesAnaesthetic Management of Emergency LSCS, An Unusual Case of Complete Heart Block With Permanent Pace MakerIOSRjournalNo ratings yet
- Heart BlocksDocument6 pagesHeart BlocksMark Hammerschmidt100% (1)
- Download ebook Goldbergers Clinical Electrocardiography A Simplified Approach Pdf full chapter pdfDocument52 pagesDownload ebook Goldbergers Clinical Electrocardiography A Simplified Approach Pdf full chapter pdfjames.farnan170100% (21)
- Cardiac ArrhythmiasDocument14 pagesCardiac ArrhythmiasArvin John ManuelNo ratings yet
- ECG Made Easy - Heart Block Types ExplainedDocument37 pagesECG Made Easy - Heart Block Types ExplainedabdallahNo ratings yet
- EkggDocument44 pagesEkggLedy ErvitaNo ratings yet
- Cvs PathoDocument36 pagesCvs PathoISRAELNo ratings yet
- AV Nodal BlocksDocument19 pagesAV Nodal BlocksHarsha VijaykumarNo ratings yet
- Goldbergers Clinical Electrocardiography 9th Edition PDFDocument360 pagesGoldbergers Clinical Electrocardiography 9th Edition PDFdr_mego75% (4)