You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Software Dev Processes Project 1Document2 pagesSoftware Dev Processes Project 1ereter50% (8)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Learning Styles Kolb QuestionnaireDocument6 pagesLearning Styles Kolb QuestionnaireAkshay BellubbiNo ratings yet
- CT Canon Aquilion Lightning enDocument36 pagesCT Canon Aquilion Lightning enTAIWO ISHOLANo ratings yet
- Probation Period ReportDocument17 pagesProbation Period ReportMiranti Puspitasari0% (1)
- Maternal Mortality SaudiDocument5 pagesMaternal Mortality SaudiJestoni Dulva ManiagoNo ratings yet
- Cultural DiversityDocument35 pagesCultural DiversityJestoni Dulva ManiagoNo ratings yet
- NRS 361 - Unit 1Document9 pagesNRS 361 - Unit 1Jestoni Dulva ManiagoNo ratings yet
- History of NursingDocument38 pagesHistory of NursingJestoni Dulva ManiagoNo ratings yet
- OLDS Week2 QwizdomDocument142 pagesOLDS Week2 QwizdomJestoni Dulva ManiagoNo ratings yet
- Pots Muscles: (COPD)Document19 pagesPots Muscles: (COPD)Jestoni Dulva ManiagoNo ratings yet
- Nursing TBTB1Document104 pagesNursing TBTB1ptkduong100% (1)
- OLDS Week2 QwizdomDocument142 pagesOLDS Week2 QwizdomJestoni Dulva ManiagoNo ratings yet
- Bioethical PrinciplesDocument4 pagesBioethical PrinciplesJestoni Dulva ManiagoNo ratings yet
- Competency Validation: Practice Exercises IIDocument2 pagesCompetency Validation: Practice Exercises IIJestoni Dulva ManiagoNo ratings yet
- Competency Validation IVDocument7 pagesCompetency Validation IVJestoni Dulva ManiagoNo ratings yet
- Man 204 PrimerDocument38 pagesMan 204 PrimerJestoni Dulva ManiagoNo ratings yet
- Research B (Research Proposal Matrix)Document9 pagesResearch B (Research Proposal Matrix)Jestoni Dulva ManiagoNo ratings yet
- Competency Validation: Practice Exercises IIIDocument3 pagesCompetency Validation: Practice Exercises IIIJestoni Dulva ManiagoNo ratings yet
- 4 Three Way Factorial AnovaDocument21 pages4 Three Way Factorial AnovaJestoni Dulva ManiagoNo ratings yet
- Competency Validation: Practice Exercises IDocument2 pagesCompetency Validation: Practice Exercises IJestoni Dulva ManiagoNo ratings yet
- Norepinephrine Acetylcholine (Ach)Document6 pagesNorepinephrine Acetylcholine (Ach)Jestoni Dulva Maniago100% (3)
- Realistic Robot SimulationDocument102 pagesRealistic Robot SimulationDraconixNo ratings yet
- Pengenalan Dan Pemanfaatan Marketplace E-Commerce Untuk Pelaku Ukm Wilayah CilegonDocument8 pagesPengenalan Dan Pemanfaatan Marketplace E-Commerce Untuk Pelaku Ukm Wilayah CilegonPemetaanPendidikanNo ratings yet
- Getting Started With STM32 - Introduction To STM32CubeIDEDocument18 pagesGetting Started With STM32 - Introduction To STM32CubeIDEXiaofang JiangNo ratings yet
- Verona Medical Group - DENT-X EVA 2010Document4 pagesVerona Medical Group - DENT-X EVA 2010VeronaMedicalGroupYYNo ratings yet
- FS2Crew Airbus X Voice Control Manual PDFDocument49 pagesFS2Crew Airbus X Voice Control Manual PDFViorica Sburlea-MarinNo ratings yet
- Cambridge IGCSE: Computer Science 0478/21Document16 pagesCambridge IGCSE: Computer Science 0478/21Ahmed ZeeshanNo ratings yet
- SOP Section Rolling Machine #10011234567891123Document3 pagesSOP Section Rolling Machine #10011234567891123saturnelNo ratings yet
- Switch TI PG541Document3 pagesSwitch TI PG541KeviinCarrilloNo ratings yet
- Schedule: Timing Topic: 30 Minutes 50 Minutes Practice 80 Minutes TotalDocument115 pagesSchedule: Timing Topic: 30 Minutes 50 Minutes Practice 80 Minutes TotalCacobitoNo ratings yet
- Lovehatethings 2008Document107 pagesLovehatethings 2008Anthony MarcoNo ratings yet
- Li-B17E7 User ManualDocument1 pageLi-B17E7 User ManualKatia KorndorferNo ratings yet
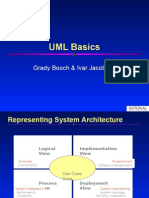
- UML Basics: Grady Booch & Ivar JacobsonDocument101 pagesUML Basics: Grady Booch & Ivar Jacobsongunasekaran.subramani3879100% (1)
- Middleware Seminar ReportDocument22 pagesMiddleware Seminar ReportSudipta Dhara33% (3)
- High Performance Cleanrooms - Cleanroom Design Guide - January 2006Document48 pagesHigh Performance Cleanrooms - Cleanroom Design Guide - January 2006Hubert BonamisNo ratings yet
- A SEMINAR REPORT Tele-Immersion 1gowDocument25 pagesA SEMINAR REPORT Tele-Immersion 1gowSunil RAYALASEEMA GRAPHICSNo ratings yet
- BuiltIn Proactive Services List - 05 - 12 - 2020Document20 pagesBuiltIn Proactive Services List - 05 - 12 - 2020oorhan41No ratings yet
- Activity 3 - 2nd QRTRDocument3 pagesActivity 3 - 2nd QRTRdagamacvincentjade10No ratings yet
- IMP Q For End Sem ExaminationDocument2 pagesIMP Q For End Sem Examinationzk8745817No ratings yet
- PVV Solar Cell US0123 PDFDocument2 pagesPVV Solar Cell US0123 PDFNguyễn Anh DanhNo ratings yet
- NBH DBH BBH Comparision SikarDocument21 pagesNBH DBH BBH Comparision SikarNikhil Kumar Gupta100% (1)
- Training ReportDocument30 pagesTraining ReportManuka DilshanNo ratings yet
- An565 Rev. 7Document4 pagesAn565 Rev. 7David WongNo ratings yet
- Graseby MR10 - Respiration Monitor - Service ManualDocument34 pagesGraseby MR10 - Respiration Monitor - Service ManualEduardoNo ratings yet
- Nokia.Document1 pageNokia.kshiti ahireNo ratings yet
- Ford C Max 2011 UKDocument25 pagesFord C Max 2011 UKDumitru PopescuNo ratings yet
- 1par Regular (New)Document8 pages1par Regular (New)Daw Aye NweNo ratings yet
- Resistors: Take A Stance, The Resist StanceDocument35 pagesResistors: Take A Stance, The Resist Stancepavan pujarNo ratings yet