You might also like
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- Case 1-PCGH Cerebrovascular DiseaseDocument40 pagesCase 1-PCGH Cerebrovascular DiseaseHynne Jhea EchavezNo ratings yet
- Patient History Amang 2Document7 pagesPatient History Amang 2Christine Evan HoNo ratings yet
- Junsay, Twinkle Mae D. Section A - Group 10 History #1Document15 pagesJunsay, Twinkle Mae D. Section A - Group 10 History #1Twinkle Mae JunsayNo ratings yet
- HISTORY # 1 - PCGH, EchavezDocument11 pagesHISTORY # 1 - PCGH, EchavezHynne Jhea EchavezNo ratings yet
- Date and Time: June 23, 2018, 3PM Chief Complaint: Difficulty of Breathing History of Present IllnessDocument3 pagesDate and Time: June 23, 2018, 3PM Chief Complaint: Difficulty of Breathing History of Present IllnessConcepcion R. AquinoNo ratings yet
- Week 3 Case - DOBDocument3 pagesWeek 3 Case - DOBKirk Matthew ZhuNo ratings yet
- IM - Patient Esguera (Final)Document4 pagesIM - Patient Esguera (Final)k.n.e.d.No ratings yet
- Highest Blood Pressure Was 140/90 MMHGDocument5 pagesHighest Blood Pressure Was 140/90 MMHGFG ArciagaNo ratings yet
- Psychiatric HistoryDocument6 pagesPsychiatric HistoryAlfonso PlantillaNo ratings yet
- Case 3.1Document11 pagesCase 3.1atdumagNo ratings yet
- History PCGH PXDocument3 pagesHistory PCGH PXAgape Love AbonadorNo ratings yet
- Im - TBDocument11 pagesIm - TBTrisNo ratings yet
- Case 2Document12 pagesCase 2atdumagNo ratings yet
- Ent Case Report Acute Otitis Media Stage IIIDocument12 pagesEnt Case Report Acute Otitis Media Stage IIIRem Alfelor100% (1)
- Case Report VI Internal MedicineDocument13 pagesCase Report VI Internal MedicineGidu SaidNo ratings yet
- Case 4Document12 pagesCase 4atdumagNo ratings yet
- Duran, Kayllien - Group 7 Sec ADocument5 pagesDuran, Kayllien - Group 7 Sec AKAYLLIEN DURANNo ratings yet
- 2 - 23 - 23 AM WardDocument10 pages2 - 23 - 23 AM WardkellogskrispiesNo ratings yet
- Case 3Document10 pagesCase 3atdumagNo ratings yet
- IM Gastro FinalDocument10 pagesIM Gastro FinalIzzyMaxinoNo ratings yet
- BPUDDocument26 pagesBPUDIvanNo ratings yet
- Acs Abeleda Abo AbrahamDocument70 pagesAcs Abeleda Abo AbrahamAj Christian Lacuesta IsipNo ratings yet
- Final Assessment Soap NoteDocument13 pagesFinal Assessment Soap Noteapi-494643478100% (3)
- History 1Document11 pagesHistory 1KaleabNo ratings yet
- Surgery: ENT: Case PresentationDocument67 pagesSurgery: ENT: Case Presentation15Ma. Shaira O PerigoNo ratings yet
- Clinical Case: Section A - Group 8Document68 pagesClinical Case: Section A - Group 8madison Deli100% (1)
- Chief ComplaintDocument7 pagesChief ComplaintyohannesNo ratings yet
- History and PE Med3ADocument3 pagesHistory and PE Med3Aawesome avedNo ratings yet
- Mundo - Ob Case 1Document6 pagesMundo - Ob Case 1Jxyp MundoNo ratings yet
- Ward Paper LegitDocument13 pagesWard Paper LegitLuigi FranciscoNo ratings yet
- Case Report II Internal MedicineDocument11 pagesCase Report II Internal MedicineGidu SaidNo ratings yet
- Enterobiasis CaseDocument4 pagesEnterobiasis CaseKimm Delos ReyesNo ratings yet
- IM-Hx and PE Cough and Dyspnea (CAP)Document34 pagesIM-Hx and PE Cough and Dyspnea (CAP)TrisNo ratings yet
- Acute PancreatitisDocument7 pagesAcute PancreatitisPatrick DycocoNo ratings yet
- Dengue Nov2019Document87 pagesDengue Nov2019Marie Razel Lopez100% (1)
- CCCCCDocument1 pageCCCCCAlexxakaye BasilioNo ratings yet
- Template Gyn Lo Abd PainDocument18 pagesTemplate Gyn Lo Abd PainHassan HarirNo ratings yet
- CASE 3 MEDICINE JULY 10 2019 AcutePyeloDocument15 pagesCASE 3 MEDICINE JULY 10 2019 AcutePyeloTrisNo ratings yet
- I. General DataDocument7 pagesI. General Datamadison DeliNo ratings yet
- I. General DataDocument6 pagesI. General Datamadison DeliNo ratings yet
- Upper Gastrointestin Al Bleeding: Case Presentation BSN 3-1Document80 pagesUpper Gastrointestin Al Bleeding: Case Presentation BSN 3-1Lanrose Parocha100% (1)
- Monroy Christian CCMH OpdDocument5 pagesMonroy Christian CCMH OpdAlfonso PlantillaNo ratings yet
- Pedia August 29Document4 pagesPedia August 29Raymund AldabaNo ratings yet
- Low Back PainDocument9 pagesLow Back PainDoc AchondoNo ratings yet
- Family Case AnalysisDocument27 pagesFamily Case AnalysisEzekiel ArtetaNo ratings yet
- HIVCase Report II Internal MedicineDocument12 pagesHIVCase Report II Internal Medicineaxmedfare138No ratings yet
- PD2-Pulmo Embolism - AchondoDocument13 pagesPD2-Pulmo Embolism - AchondocarlosNo ratings yet
- Discharge Summary JAGONOYDocument6 pagesDischarge Summary JAGONOYKirstie de LunaNo ratings yet
- Type The Document Title: Department of Surgery Case Report-IiDocument10 pagesType The Document Title: Department of Surgery Case Report-IiEyosiyas AbiyNo ratings yet
- Write Up Surgery 1 TambahDocument22 pagesWrite Up Surgery 1 Tambahazizi abd rahmanNo ratings yet
- Constitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofDocument10 pagesConstitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofRichard ObinwankwoNo ratings yet
- Source and Reliability: Informant Is Her Mother With A Reliability of 90%Document3 pagesSource and Reliability: Informant Is Her Mother With A Reliability of 90%Dennis Jr ManguilimotanNo ratings yet
- Team C Final Written OutputDocument22 pagesTeam C Final Written OutputCarina SuarezNo ratings yet
- Case Presentation: Course: EndocrinologyDocument13 pagesCase Presentation: Course: EndocrinologyCalingalan Hussin CaluangNo ratings yet
- Adult Patient History & Physical Assessement: Central Philippine UniversityDocument10 pagesAdult Patient History & Physical Assessement: Central Philippine UniversityJoshua Elli BajadaNo ratings yet
- Protocol - IM Cough and DyspneaDocument7 pagesProtocol - IM Cough and DyspneaTrisNo ratings yet
- Case 1 Doc GonsalvesDocument7 pagesCase 1 Doc GonsalvesMonique Angela Turingan GanganNo ratings yet
- Milestone 8 PresentationDocument6 pagesMilestone 8 PresentationericNo ratings yet
- Chest CaseDocument19 pagesChest CaseNesma AdelNo ratings yet
- Iso 9227Document13 pagesIso 9227Raj Kumar100% (6)
- Chapter 8 - Lipids and Proteins Are Associated in Biological Membranes - Part 1Document44 pagesChapter 8 - Lipids and Proteins Are Associated in Biological Membranes - Part 1Tommy RamazzottoNo ratings yet
- STR Mpa-MpmDocument8 pagesSTR Mpa-MpmBANGGANo ratings yet
- Scoop of Practice aOTADocument9 pagesScoop of Practice aOTAfercespedNo ratings yet
- Beckhoff Service Tool - USB StickDocument7 pagesBeckhoff Service Tool - USB StickGustavo VélizNo ratings yet
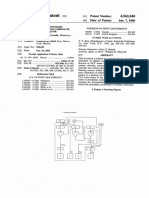
- 10.1.polendo (Additional Patent)Document11 pages10.1.polendo (Additional Patent)Rima AmaliaNo ratings yet
- Removing Eyelid LesionsDocument4 pagesRemoving Eyelid LesionsMohammad Abdullah BawtagNo ratings yet
- 220hp Caterpillar 3306 Gardner Denver SSP Screw Compressor DrawingsDocument34 pages220hp Caterpillar 3306 Gardner Denver SSP Screw Compressor DrawingsJVMNo ratings yet
- Abfraction, Abrasion, Biocorrosion, and The Enigma of Noncarious Cervical Lesions: A 20-Year PerspectivejerdDocument14 pagesAbfraction, Abrasion, Biocorrosion, and The Enigma of Noncarious Cervical Lesions: A 20-Year PerspectivejerdLucianoNo ratings yet
- Literary Portraiture & Modern Spain: Dr. Rebecca M. Bender (Document6 pagesLiterary Portraiture & Modern Spain: Dr. Rebecca M. Bender (Pedro PorbénNo ratings yet
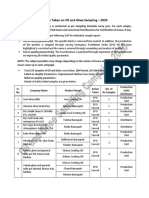
- Action Taken On Oil and Ghee Sampling - 2020Document2 pagesAction Taken On Oil and Ghee Sampling - 2020Khalil BhattiNo ratings yet
- Grand Hyatt Manila In-Room Dining MenuDocument14 pagesGrand Hyatt Manila In-Room Dining MenuMetroStaycation100% (1)
- (Cô Vũ Mai Phương) Tài liệu LIVESTREAM - Chuyên đề thi THPT - Câu hỏi giao tiếp xã hội (Buổi 1)Document4 pages(Cô Vũ Mai Phương) Tài liệu LIVESTREAM - Chuyên đề thi THPT - Câu hỏi giao tiếp xã hội (Buổi 1)nguyen duong trungNo ratings yet
- PPC Production PlantDocument106 pagesPPC Production PlantAljay Neeson Imperial100% (1)
- Unit-7 (EVS)Document32 pagesUnit-7 (EVS)g6614134No ratings yet
- Hamraki Rag April 2010 IssueDocument20 pagesHamraki Rag April 2010 IssueHamraki RagNo ratings yet
- Onuaguluchi1996 1Document10 pagesOnuaguluchi1996 1IkaSugihartatikNo ratings yet
- Resume Massage Therapist NtewDocument2 pagesResume Massage Therapist NtewPartheebanNo ratings yet
- MAOH600 Ropu 48 Presentation Script and ReferencesDocument10 pagesMAOH600 Ropu 48 Presentation Script and ReferencesFano AsiataNo ratings yet
- Assignment On Inservice Education Sub: Community Health NursingDocument17 pagesAssignment On Inservice Education Sub: Community Health NursingPrity DeviNo ratings yet
- Total Elbow Arthroplasty and RehabilitationDocument5 pagesTotal Elbow Arthroplasty and RehabilitationMarina ENo ratings yet
- Chomp Excersie 3Document5 pagesChomp Excersie 3Omahri24No ratings yet
- Reverse Osmosis Desalination: Our Global Expertise To Address Water ScarcityDocument16 pagesReverse Osmosis Desalination: Our Global Expertise To Address Water Scarcitynice guyNo ratings yet
- Active Contracts by Contract Number Excluded 0Document186 pagesActive Contracts by Contract Number Excluded 0JAGUAR GAMINGNo ratings yet
- Acuson P10Document2 pagesAcuson P10anon-259218No ratings yet
- 3 Ways To Take Isabgol - WikiHowDocument6 pages3 Ways To Take Isabgol - WikiHownasirNo ratings yet
- Case Report 3 MukokelDocument3 pagesCase Report 3 MukokelWidychii GadiestchhetyaNo ratings yet
- Essay 31 - Permissive ParentingDocument2 pagesEssay 31 - Permissive Parentingqbich37No ratings yet
- Chapter One - FiveDocument118 pagesChapter One - FivePrecious AnthonyNo ratings yet
- Method Statement For Installation of Chilled Water Pump & Condenser Water PumpDocument14 pagesMethod Statement For Installation of Chilled Water Pump & Condenser Water Pump721917114 47No ratings yet