You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Antibiotic Guidelines - 2018 PDFDocument80 pagesAntibiotic Guidelines - 2018 PDFarnaldops333No ratings yet
- Practice: Interpreting A Covid-19 Test ResultDocument7 pagesPractice: Interpreting A Covid-19 Test ResultSteveNo ratings yet
- Antibiotic Guidelines - 2018 PDFDocument80 pagesAntibiotic Guidelines - 2018 PDFarnaldops333No ratings yet
- Combatting COVID-19 - 2020 - Ultrasound PDFDocument6 pagesCombatting COVID-19 - 2020 - Ultrasound PDFarnaldops333No ratings yet
- Clin Infect Dis.-2016-Kalil-cid-ciw353 PDFDocument51 pagesClin Infect Dis.-2016-Kalil-cid-ciw353 PDFarnaldops333No ratings yet
- Continuous and Extended Infusion Beta Lactams PDFDocument3 pagesContinuous and Extended Infusion Beta Lactams PDFarnaldops333No ratings yet
- Antibiotic Prophylaxis To ReduceDocument78 pagesAntibiotic Prophylaxis To Reducearnaldops333No ratings yet
- Nej MR A 1212788Document9 pagesNej MR A 1212788Cynthia TanuwijoyoNo ratings yet
- Antibiotic TherapyDocument9 pagesAntibiotic Therapyarnaldops333No ratings yet
- Empiric Antibiotic Use in Critically Ill Patients - 2007Document9 pagesEmpiric Antibiotic Use in Critically Ill Patients - 2007arnaldops333No ratings yet
- Nej MR A 1212788Document9 pagesNej MR A 1212788Cynthia TanuwijoyoNo ratings yet
- How Can We Predict Bacterial EradicationDocument8 pagesHow Can We Predict Bacterial Eradicationarnaldops333No ratings yet
- Ada 2012 PDFDocument7 pagesAda 2012 PDFSamuel UrrutiaNo ratings yet
- Update On The Antimicrobial Management of FootDocument7 pagesUpdate On The Antimicrobial Management of Footarnaldops333No ratings yet
- Asthma Guidlines RCPCHDocument28 pagesAsthma Guidlines RCPCHMohamed AmrNo ratings yet
- CES6 - Infectious Disease BookDocument138 pagesCES6 - Infectious Disease Bookarnaldops333No ratings yet
- Guide 2.1 AntimicrobialDocument11 pagesGuide 2.1 Antimicrobialarnaldops333No ratings yet
- Opp MycoDocument9 pagesOpp Mycoarnaldops333No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Papain, Chymotrypsin and Related Proteins-A Comparative Study of Their Beer Chill-Proofing Abilities and CharacteristicsDocument5 pagesPapain, Chymotrypsin and Related Proteins-A Comparative Study of Their Beer Chill-Proofing Abilities and CharacteristicsAna PaulaNo ratings yet
- Biosintesis Asam FenolikDocument92 pagesBiosintesis Asam FenolikSariyana Ana TogubuNo ratings yet
- BIOCHEMISTRY IntroductionDocument3 pagesBIOCHEMISTRY IntroductionKentNo ratings yet
- Antibiotics NotesDocument7 pagesAntibiotics NotesmuhammadridhwanNo ratings yet
- Pseudomonas Biofilm Formation and Antibiotic Resistance Are Linked To Phenotypic VariationDocument4 pagesPseudomonas Biofilm Formation and Antibiotic Resistance Are Linked To Phenotypic VariationChadi AzarNo ratings yet
- Cetirizine Degradation ProductsDocument7 pagesCetirizine Degradation ProductsASHOK KUMAR LENKANo ratings yet
- STSDocument4 pagesSTSMochaNo ratings yet
- Cover Letter PHDDocument2 pagesCover Letter PHDAmit Rath100% (3)
- Conversion RPM G CentrifugaDocument1 pageConversion RPM G CentrifugaEsaú E RodriguezNo ratings yet
- Std08 I MSSS EM 2 PDFDocument56 pagesStd08 I MSSS EM 2 PDFSenthilmurugan RamalingamNo ratings yet
- Eva Green Bio Rad PDFDocument2 pagesEva Green Bio Rad PDFMoniqueNo ratings yet
- An Introduction To BiotechnologyDocument21 pagesAn Introduction To BiotechnologyBrayan Trujillo rojasNo ratings yet
- Timeline DNADocument1 pageTimeline DNAEleyra Llanos ParraNo ratings yet
- LIST of Fake JournalsDocument11 pagesLIST of Fake JournalsG NagarajanNo ratings yet
- Real Time PCR Guide Bio RadDocument105 pagesReal Time PCR Guide Bio Radeubacteria100% (1)
- Contemporary Issues in Pharmaceutical MicrobiologyDocument49 pagesContemporary Issues in Pharmaceutical MicrobiologyTim Sandle100% (2)
- SopDocument3 pagesSopSharmaRubinaNo ratings yet
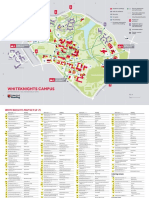
- Whiteknights Campus MapDocument4 pagesWhiteknights Campus MapRajvirBhogalNo ratings yet
- Agricultural Biotechnology in The PhilippinesDocument11 pagesAgricultural Biotechnology in The PhilippinesAnonymous HXLczq3No ratings yet
- Fish Protein FingerprintingDocument23 pagesFish Protein Fingerprintingrahmi93No ratings yet
- Proteus Mirabilis Producing The OXA-58 Carbapenemase in PolandDocument7 pagesProteus Mirabilis Producing The OXA-58 Carbapenemase in PolandAlexandru MunteanNo ratings yet
- Autotrophic Growth and Carotenoid Production of HP in A 30 Liter Air Lift PhotobioreactorDocument6 pagesAutotrophic Growth and Carotenoid Production of HP in A 30 Liter Air Lift PhotobioreactorcikpayungNo ratings yet
- The Pharmaceutical and Chemical JournalDocument2 pagesThe Pharmaceutical and Chemical JournalAlexandru CroitoruNo ratings yet
- Scilligence Joins Accenture's Life Sciences Research Platform Ecosystem To Help Drive Innovation in Drug Discovery and Scientific ResearchDocument3 pagesScilligence Joins Accenture's Life Sciences Research Platform Ecosystem To Help Drive Innovation in Drug Discovery and Scientific ResearchPR.comNo ratings yet
- History, Development and Status of BT Cotton in IndiaDocument73 pagesHistory, Development and Status of BT Cotton in IndiaRajasekarNo ratings yet
- Fhéç - F©LHW Eâ Ú® Ïiz Ò¡F: %.2180 Nfhoæš NK Bfhÿs G L Gâia Ãw Âat® B#AyèjhDocument4 pagesFhéç - F©LHW Eâ Ú® Ïiz Ò¡F: %.2180 Nfhoæš NK Bfhÿs G L Gâia Ãw Âat® B#AyèjhmuslimleaguetnNo ratings yet
- Chapter - 12 Need For The Introduction of Regulatory Affairs in The Pharmacy CurriculumDocument2 pagesChapter - 12 Need For The Introduction of Regulatory Affairs in The Pharmacy CurriculumSalil IlmeNo ratings yet
- Polymerase Chain Reaction: Investigation Strategies and MethodsDocument24 pagesPolymerase Chain Reaction: Investigation Strategies and MethodsHelda GadjaNo ratings yet
- OriginofeukaryoticcellsDocument1 pageOriginofeukaryoticcellsSam JayNo ratings yet
- Cochran Fellowship Rpogram Alumni Interview Questions Forbiotech Program...Document2 pagesCochran Fellowship Rpogram Alumni Interview Questions Forbiotech Program...precaute100% (1)