You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- 02-EM The CapgeminiWay - The Value of Effective Delivery - V3.1Document17 pages02-EM The CapgeminiWay - The Value of Effective Delivery - V3.1amit_singhal50% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ex-NYPD Cop Awarded PTSD Benefits, Sues For 'Incalculable' Sexual Violence in The WorkplaceDocument61 pagesEx-NYPD Cop Awarded PTSD Benefits, Sues For 'Incalculable' Sexual Violence in The WorkplaceEric SandersNo ratings yet
- HR Audit ChecklistDocument9 pagesHR Audit Checklistchichi mpiNo ratings yet
- HR Topics For Debate CompetitionDocument1 pageHR Topics For Debate CompetitionEsha Aditya SalkarNo ratings yet
- Fed Biz 072909 CloudDocument2 pagesFed Biz 072909 Cloudshri85No ratings yet
- NITD BTech RegulationsDocument21 pagesNITD BTech Regulationsakbisoi1No ratings yet
- PythonDocument44 pagesPythonakbisoi1No ratings yet
- 1253acadmic Regulation UpdatedDocument37 pages1253acadmic Regulation Updatedsatyaranjan_313No ratings yet
- An Introduction To Python Programming LanguageDocument63 pagesAn Introduction To Python Programming Languageakbisoi1No ratings yet
- Chapter 2 Inverse Trigonometric FunctionsDocument0 pagesChapter 2 Inverse Trigonometric FunctionsAkash ChatterjeeNo ratings yet
- Arithmetic & Logic UnitDocument58 pagesArithmetic & Logic Unitakbisoi1No ratings yet
- Larman Chapter 6Document56 pagesLarman Chapter 6toomy144No ratings yet
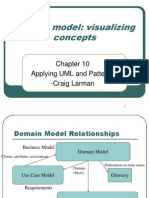
- Domain Model: Visualizing Concepts: Applying UML and Patterns - Craig LarmanDocument13 pagesDomain Model: Visualizing Concepts: Applying UML and Patterns - Craig Larmanakbisoi1No ratings yet
- Larman Chapter 9Document27 pagesLarman Chapter 9akbisoi1No ratings yet
- Larman Chapter 7Document14 pagesLarman Chapter 7akbisoi1No ratings yet
- Understanding Requirements: Applying UML and Patterns - Craig LarmanDocument8 pagesUnderstanding Requirements: Applying UML and Patterns - Craig Larmanakbisoi1No ratings yet
- From Inception To Elaboration: Applying UML and Patterns - Craig LarmanDocument14 pagesFrom Inception To Elaboration: Applying UML and Patterns - Craig Larmanakbisoi1No ratings yet
- Larman Chapter 6Document56 pagesLarman Chapter 6toomy144No ratings yet
- ICS4M0 - Final Culminating ProblemsDocument4 pagesICS4M0 - Final Culminating Problemsakbisoi1No ratings yet
- Larman Chapter 7Document14 pagesLarman Chapter 7akbisoi1No ratings yet
- TrigonometruyDocument3 pagesTrigonometruyRitu SharmaNo ratings yet
- Vedic Maths': Myths and FactsDocument6 pagesVedic Maths': Myths and FactsSrikanth Kasimohanty PatnaikNo ratings yet
- Module Design Issues: MSWE607 - Fall 2000 - Slides 12 © M V Zelkowitz, 2000Document17 pagesModule Design Issues: MSWE607 - Fall 2000 - Slides 12 © M V Zelkowitz, 2000akbisoi1No ratings yet
- Form 2Document1 pageForm 2vvskrNo ratings yet
- Solutions - Final Test On Unit 0Document3 pagesSolutions - Final Test On Unit 0akbisoi1No ratings yet
- Utkal Bca SyllabusDocument19 pagesUtkal Bca Syllabusakbisoi1No ratings yet
- Unit 3 - Advanced Algorithms and Programming PrinciplesDocument15 pagesUnit 3 - Advanced Algorithms and Programming Principlesakbisoi1No ratings yet
- Windows Operating System Part 1Document28 pagesWindows Operating System Part 1Adnan QuddosNo ratings yet
- Modularity and Coupling and Cohesion: SE464/CS446/ECE452Document30 pagesModularity and Coupling and Cohesion: SE464/CS446/ECE452admzaemNo ratings yet
- Lec 16 Metrics CohesionDocument22 pagesLec 16 Metrics Cohesionakbisoi1100% (1)
- Practice Problems 1Document34 pagesPractice Problems 1akbisoi1No ratings yet
- RaoDocument30 pagesRaoakbisoi1No ratings yet
- Lesson 3Document10 pagesLesson 3Smita R. S.No ratings yet
- Lec 20Document8 pagesLec 20akbisoi1No ratings yet
- 2017 UcdDocument60 pages2017 UcdfirstNo ratings yet
- IG1-IGC1 Sample of Past Paper August 2020Document5 pagesIG1-IGC1 Sample of Past Paper August 2020Razvan-Teodor PuscasuNo ratings yet
- Arup Future of Project Management2Document68 pagesArup Future of Project Management2LaurentiuNo ratings yet
- ECE1012 RaDocument162 pagesECE1012 RaNonoyTaclinoNo ratings yet
- AP Executive SummaryDocument6 pagesAP Executive SummarySyed IrfanuddinNo ratings yet
- Jan Shiksha Sansthan: Ministry of Skill Development and EntreprenurshipDocument11 pagesJan Shiksha Sansthan: Ministry of Skill Development and EntreprenurshipRitik ShuklaNo ratings yet
- 12harrod Domar Model NOTESDocument4 pages12harrod Domar Model NOTESShivaditya VermanNo ratings yet
- Application FormDocument6 pagesApplication Form150 270No ratings yet
- The Industrial Disputes ActDocument29 pagesThe Industrial Disputes ActVummitti ChandhiniNo ratings yet
- The Gallo Company Uses A Flexible Budget and Standard CostsDocument2 pagesThe Gallo Company Uses A Flexible Budget and Standard CostsAmit PandeyNo ratings yet
- Apturja Case Decision SheetDocument6 pagesApturja Case Decision SheetSajin SomanNo ratings yet
- PMR Employment Application Form. EDMONDDocument5 pagesPMR Employment Application Form. EDMONDEdmond EddieNo ratings yet
- INZ 1016 - Work Visa Guide (INZ 1016) - July 2015Document20 pagesINZ 1016 - Work Visa Guide (INZ 1016) - July 2015Dragoslav DzolicNo ratings yet
- WWW - Pakassignment.Blog: Send Your Assignments and Projects To Be Displayed Here As Sample For Others atDocument46 pagesWWW - Pakassignment.Blog: Send Your Assignments and Projects To Be Displayed Here As Sample For Others atPakassignmentNo ratings yet
- EMPLOYEE BENEFITS - Written ReportDocument20 pagesEMPLOYEE BENEFITS - Written ReportGerha Marie Bugtay PabutawanNo ratings yet
- Work System Design: Operations Management R. Dan Reid & Nada R. SandersDocument40 pagesWork System Design: Operations Management R. Dan Reid & Nada R. Sanderssani29No ratings yet
- Fti Tvet Leadership & Management: Course: Tvet Management By: Bekre H. (PHD) Addis Ababa EthiopiaDocument113 pagesFti Tvet Leadership & Management: Course: Tvet Management By: Bekre H. (PHD) Addis Ababa EthiopiaTsega BirhanuNo ratings yet
- Case LawDocument40 pagesCase LawSwati SharmaNo ratings yet
- Contoh TerdekatDocument45 pagesContoh Terdekatidirz tonyNo ratings yet
- Health and Safety Dissertation1Document34 pagesHealth and Safety Dissertation1Arjuna Cuttaree100% (3)
- Utf-8''Guinea Labour Code 10 Jan 14 (En)Document83 pagesUtf-8''Guinea Labour Code 10 Jan 14 (En)med ouaerNo ratings yet
- The Pay Model-3Document16 pagesThe Pay Model-3Bharti PunjabiNo ratings yet
- Job Safety Analysis Worksheet: Tie - in For Power Cable 33 KVDocument3 pagesJob Safety Analysis Worksheet: Tie - in For Power Cable 33 KVmohammed a hseNo ratings yet
- Fundamentals of Occupational Safety and HealthDocument1 pageFundamentals of Occupational Safety and HealthNjoroge IkonyeNo ratings yet
- Contoh Surat Lamaran Kerja Bhs InggrisDocument3 pagesContoh Surat Lamaran Kerja Bhs InggrisGito LiemNo ratings yet
- 6Document14 pages6WaqarNo ratings yet