You might also like
- Kurt Cobain Case StudyDocument11 pagesKurt Cobain Case StudyKC Respicio67% (3)
- Chest TraumaDocument9 pagesChest Traumaapi-3838240100% (7)
- Advances in Extraction TechniquesDocument13 pagesAdvances in Extraction TechniquesashajangamNo ratings yet
- Medical Mnemonic Sketches : Pulmonary DiseasesFrom EverandMedical Mnemonic Sketches : Pulmonary DiseasesNo ratings yet
- Atelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesFrom EverandAtelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesNo ratings yet
- Total Leukocyte Count by HemocytometerDocument4 pagesTotal Leukocyte Count by HemocytometerMalkish RajkumarNo ratings yet
- Symptoms and Signs of Respiratory Disease Lecture 2: DyspnoeaDocument9 pagesSymptoms and Signs of Respiratory Disease Lecture 2: DyspnoeaShannon RamsumairNo ratings yet
- Ards 2Document7 pagesArds 2LUCIBELLOT1No ratings yet
- Intestinal Polyps and PolyposisDocument244 pagesIntestinal Polyps and PolyposisVladislav KotovNo ratings yet
- Protective and Symptomatic Cough: Causes and AssessmentDocument10 pagesProtective and Symptomatic Cough: Causes and AssessmentCatharinaNoviaNo ratings yet
- Acute Lung InjuryDocument18 pagesAcute Lung InjuryM Rizal IsburhanNo ratings yet
- Acute Respiratory Distress SyndromeDocument17 pagesAcute Respiratory Distress SyndromeSanjeet SahNo ratings yet
- Atelectasis EditedDocument40 pagesAtelectasis EditedAimee Gutierrez100% (1)
- Non-Rebreather MaskDocument15 pagesNon-Rebreather MaskKesyaNo ratings yet
- Atelectasis: Go ToDocument10 pagesAtelectasis: Go Tosuci triana putriNo ratings yet
- ARDSDocument55 pagesARDSSandhya HarbolaNo ratings yet
- ATELECTASISDocument5 pagesATELECTASISAngellene GraceNo ratings yet
- Establish An AirwayDocument7 pagesEstablish An AirwayMarionne James Jaranilla DinongNo ratings yet
- Endotracheal Intubation Learning MaterialDocument8 pagesEndotracheal Intubation Learning MaterialLouie ParillaNo ratings yet
- Bronchospasm During Anaesthesia Update 2011Document5 pagesBronchospasm During Anaesthesia Update 2011hy3pjb1984No ratings yet
- Atelectasis-Dr JokoDocument20 pagesAtelectasis-Dr JokoMamanHermawanNo ratings yet
- Emphysema Is A LongDocument54 pagesEmphysema Is A LongryemoralesNo ratings yet
- Chest Trauma: DR - Amr BastawaisiDocument10 pagesChest Trauma: DR - Amr BastawaisiBara FakhryNo ratings yet
- NCM 103 Aliasas AtelectasisDocument3 pagesNCM 103 Aliasas AtelectasisDARREN EDMARKNo ratings yet
- Cough - Wikipedia PDFDocument59 pagesCough - Wikipedia PDFSrinivasreddy G Maali PatelNo ratings yet
- AtelectasisDocument3 pagesAtelectasisMicah MagallanoNo ratings yet
- ManagingAirwayObstruction PDFDocument5 pagesManagingAirwayObstruction PDFMeyNo ratings yet
- Occurs Most Often In:: Muscular DystrophyDocument4 pagesOccurs Most Often In:: Muscular DystrophyJiezl Abellano AfinidadNo ratings yet
- Pulmonary FailureDocument29 pagesPulmonary FailureWengel RedkissNo ratings yet
- Airway and Ventilatory ManagementDocument8 pagesAirway and Ventilatory ManagementAshen DissanayakaNo ratings yet
- Emergencies: Role OF PhysiotherapistsDocument37 pagesEmergencies: Role OF PhysiotherapistsDuppala Sateesh KumarNo ratings yet
- 2 - Dyspnea 讲课稿 2020Document16 pages2 - Dyspnea 讲课稿 2020mirabel IvanaliNo ratings yet
- AtherosclerosisDocument7 pagesAtherosclerosisAna MarieNo ratings yet
- Translet Part 2Document7 pagesTranslet Part 2Erica FitrianiNo ratings yet
- Go To:: Respiratory ImpairmentDocument18 pagesGo To:: Respiratory ImpairmentNanik LestariNo ratings yet
- CR Patho SummaryDocument22 pagesCR Patho SummaryDNAANo ratings yet
- Evaluation of DyspneaDocument11 pagesEvaluation of DyspneaNeil AlviarNo ratings yet
- Acute Respiratory Failure-PRINTDocument5 pagesAcute Respiratory Failure-PRINTJan SicatNo ratings yet
- Wikipedia - Cough (For CHECK)Document8 pagesWikipedia - Cough (For CHECK)pixoguiasNo ratings yet
- Airway ManagementDocument28 pagesAirway ManagementghazyNo ratings yet
- Laryngoscopy0 + 5 – 10secondsPlacement of ETT0 + 10 – 15secondsPositive pressure ventilation0 + 15 – 20secondsPost-intubation careDocument38 pagesLaryngoscopy0 + 5 – 10secondsPlacement of ETT0 + 10 – 15secondsPositive pressure ventilation0 + 15 – 20secondsPost-intubation careKrmilla KumillNo ratings yet
- Principles of Diagnosis and Management of Traumatic PneumothoraxDocument14 pagesPrinciples of Diagnosis and Management of Traumatic PneumothoraxEkaNo ratings yet
- Case Study For PneumothoraxDocument4 pagesCase Study For PneumothoraxGabbii CincoNo ratings yet
- Pneumothorax: Risk Factors For A PneumothoraxDocument12 pagesPneumothorax: Risk Factors For A Pneumothoraxyangi dokaNo ratings yet
- Acute Respiratory Distress Syndrome....Document55 pagesAcute Respiratory Distress Syndrome....sangi vinayagamNo ratings yet
- Pneumothorax, COPD, CVDsDocument156 pagesPneumothorax, COPD, CVDsakoeljames8543No ratings yet
- ARDS: Acute Respiratory Distress Syndrome Pathophysiology & TreatmentDocument17 pagesARDS: Acute Respiratory Distress Syndrome Pathophysiology & TreatmentAnastasia CebotariNo ratings yet
- Airway ObstructionDocument7 pagesAirway ObstructionnesredeNo ratings yet
- Vet Clin Small Anim Approach to Respiratory DistressDocument11 pagesVet Clin Small Anim Approach to Respiratory DistressDiana CarolinaNo ratings yet
- RESTRICTIVE LUNG DISEASES (Autosaved)Document40 pagesRESTRICTIVE LUNG DISEASES (Autosaved)Dr. Rabail MalikNo ratings yet
- Get Homework/Assignment DoneDocument9 pagesGet Homework/Assignment DoneHomework PingNo ratings yet
- Home - Clinical - Management - News - Products - Protocols/Guidelines - Research - Buyer's Guide - Expert Insight - ArchivesDocument8 pagesHome - Clinical - Management - News - Products - Protocols/Guidelines - Research - Buyer's Guide - Expert Insight - ArchivesDuvvuri SankarNo ratings yet
- Ventilator TroubleshootingDocument1 pageVentilator TroubleshootingJohn RaufNo ratings yet
- Clinical Presentation and Diagnosis of PneumothoraxDocument49 pagesClinical Presentation and Diagnosis of PneumothoraxisahNo ratings yet
- Acute Respiratory Failure 1Document7 pagesAcute Respiratory Failure 1Trish 0019No ratings yet
- Major Disorders of The Respiratory System: Sheryll Joy Lopez-Calayan, RN, MSNDocument69 pagesMajor Disorders of The Respiratory System: Sheryll Joy Lopez-Calayan, RN, MSNSheryll Joy Lopez CalayanNo ratings yet
- Interstitial Lung DiseaseDocument14 pagesInterstitial Lung DiseaseAzkaZulfiqarNo ratings yet
- ARDSDocument23 pagesARDSDumora FatmaNo ratings yet
- Go To:: Indications For Mechanical VentilationDocument25 pagesGo To:: Indications For Mechanical VentilationsakuraleeshaoranNo ratings yet
- Define The Acute Respiratory Distress ?: - Exudative - Proliferative - Fibrotic 1) ExudativeDocument6 pagesDefine The Acute Respiratory Distress ?: - Exudative - Proliferative - Fibrotic 1) ExudativenuraNo ratings yet
- EMPHYSEMADocument2 pagesEMPHYSEMAJerick DaangNo ratings yet
- Management of AirwaysDocument12 pagesManagement of AirwaysdyahNo ratings yet
- Day 5 Respiratory DiseaseDocument71 pagesDay 5 Respiratory DiseaseRamzen Raphael DomingoNo ratings yet
- Pneumothorax Review: Causes, Diagnosis and ManagementDocument5 pagesPneumothorax Review: Causes, Diagnosis and ManagementAby SuryaNo ratings yet
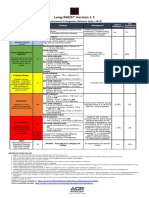
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Document1 pageLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotNo ratings yet
- Theory and Practice of Pure Tone Audiometry - PTADocument12 pagesTheory and Practice of Pure Tone Audiometry - PTAsolhazNo ratings yet
- Cervical Lymphoepithelial CystDocument6 pagesCervical Lymphoepithelial CystAhmed Al-jumailiNo ratings yet
- Definition of NephrolithiasisDocument30 pagesDefinition of Nephrolithiasiszz_13No ratings yet
- Cardiology Case 1Document2 pagesCardiology Case 1vil62650% (2)
- Asthma Attack Nursing Care Plan for Married Female PatientDocument5 pagesAsthma Attack Nursing Care Plan for Married Female PatientMarivic Yuson MalagarNo ratings yet
- Past PapaersDocument515 pagesPast PapaersShariq ShaNo ratings yet
- Autism and Dietary Therapy: Case Report and Review of The LiteratureDocument6 pagesAutism and Dietary Therapy: Case Report and Review of The LiteratureAntiopi PanteliNo ratings yet
- Comparison Between DOAC To Enoxaparin For Risk of Intracranial BleedingDocument2 pagesComparison Between DOAC To Enoxaparin For Risk of Intracranial BleedingFathima Sheik KatherNo ratings yet
- ACLS NotesDocument3 pagesACLS Notessaxmanwrv0% (1)
- Urolithiasis Overview: Classification, Pathogenesis and Treatment ModalitiesDocument38 pagesUrolithiasis Overview: Classification, Pathogenesis and Treatment Modalitiesraed ganmNo ratings yet
- Jomi 7657Document27 pagesJomi 7657casto.carpetasmiaNo ratings yet
- Dental Perspective of Pemphigus VulgarisDocument5 pagesDental Perspective of Pemphigus VulgarisSherlyNo ratings yet
- Abnormal PuerperiumDocument65 pagesAbnormal PuerperiumNigus AfessaNo ratings yet
- Abu Dhabi DRGDocument62 pagesAbu Dhabi DRGDolly creationsNo ratings yet
- Case Study 5 Year Boy With CoughDocument3 pagesCase Study 5 Year Boy With CoughAryl Eduarte100% (1)
- GROUP 10 Senstive Abt Food and Food AllergiesDocument16 pagesGROUP 10 Senstive Abt Food and Food AllergiesLilis nopita SarryNo ratings yet
- Ann JeinaDocument7 pagesAnn JeinaMizumoriFumairaNo ratings yet
- MSUDDocument23 pagesMSUDDivya AjithNo ratings yet
- QuestionsDocument6 pagesQuestionsLorvic Andrew Juanson UmaliNo ratings yet
- Lesson 3 ReviewDocument4 pagesLesson 3 ReviewHo Yong WaiNo ratings yet
- MGM Muthoot Medical Centre Patient Transfer CriteriaDocument2 pagesMGM Muthoot Medical Centre Patient Transfer CriteriaDr Jisha TuNo ratings yet
- Leaflet YTiG Plus Tablet For CHCDocument1 pageLeaflet YTiG Plus Tablet For CHCDesi Health Tips UpdateNo ratings yet
- NSAID's QuestionsDocument3 pagesNSAID's QuestionsManikanta Guptha100% (2)
- HEPATITIS B VACCINE NURSING RESPONSIBILITIESDocument14 pagesHEPATITIS B VACCINE NURSING RESPONSIBILITIESJannine BensiNo ratings yet
- Congestive Heart Failure, Pulmonary Edema, and CPAPDocument35 pagesCongestive Heart Failure, Pulmonary Edema, and CPAPSherwan R Shal100% (1)