You might also like
- User's Guide to Echinacea and Other Cold & Flu FightersFrom EverandUser's Guide to Echinacea and Other Cold & Flu FightersRating: 5 out of 5 stars5/5 (2)
- Rheumatic Heart DiseaseDocument8 pagesRheumatic Heart DiseaseJehannaMarEnggingAbdurahmanNo ratings yet
- Nursing Care Plans: Nursing Diagnosis and Assessment, Nursing Interventions GuideFrom EverandNursing Care Plans: Nursing Diagnosis and Assessment, Nursing Interventions GuideRating: 5 out of 5 stars5/5 (4)
- Seminar On Rheumatic Fever UmeshDocument4 pagesSeminar On Rheumatic Fever UmeshawasthiphothocopyNo ratings yet
- Rheumatic FeverDocument3 pagesRheumatic FeverKennette LimNo ratings yet
- Rheumatic FeverDocument56 pagesRheumatic Feveralmawang100% (1)
- Rheumatic Heart DiseaseDocument30 pagesRheumatic Heart DiseasejustinahorroNo ratings yet
- Rheumatic Heart DiseaseDocument14 pagesRheumatic Heart Diseaseudaybujji100% (1)
- Rheumatic Heart DiseaseDocument26 pagesRheumatic Heart Diseasecandice_manuel_1No ratings yet
- A Very Lengthy AssignmentDocument7 pagesA Very Lengthy AssignmentElmoi DoguilesNo ratings yet
- Meningitis PediatricDocument5 pagesMeningitis PediatricLydia Angelia YanitaNo ratings yet
- Meningitis: Coli, and Listeria Species Are The Most CommonDocument6 pagesMeningitis: Coli, and Listeria Species Are The Most CommonSarika YadavNo ratings yet
- Rheumatic Fever Small Group DiscussionDocument13 pagesRheumatic Fever Small Group DiscussionLyca Mae AurelioNo ratings yet
- RHDocument6 pagesRHAMOS MELINo ratings yet
- Acute Rheumatic FeverDocument9 pagesAcute Rheumatic FeverHarish Kumar KumawatNo ratings yet
- 10rheumatic FeverDocument3 pages10rheumatic FeverKristina Ana ClaudioNo ratings yet
- Acute Rheumatic Fever: DR Mohamed Rafa MSC PediatricsDocument6 pagesAcute Rheumatic Fever: DR Mohamed Rafa MSC PediatricsPeace ManNo ratings yet
- PBL 1 InfectiousDocument9 pagesPBL 1 InfectiousHassaan-e MuhammedNo ratings yet
- Common ColdDocument8 pagesCommon Coldvaschuk_8No ratings yet
- Kawasaki Disease: First PhaseDocument12 pagesKawasaki Disease: First PhaseRalph Ryan TolentinoNo ratings yet
- Practice Essentials: Simple Febrile SeizureDocument7 pagesPractice Essentials: Simple Febrile SeizureRebeca SpataruNo ratings yet
- Case Study DengueDocument3 pagesCase Study Denguekevinramirez08No ratings yet
- Rheumatic Heart DiseaseDocument2 pagesRheumatic Heart DiseaseDiaz RahmadiNo ratings yet
- Systemic Diseases: Learning ObjectivesDocument29 pagesSystemic Diseases: Learning ObjectivesYuusuf MubarikNo ratings yet
- Articulo Miocarditis PDFDocument9 pagesArticulo Miocarditis PDFMILENA SIERRANo ratings yet
- Practice Essentials: Simple Febrile SeizureDocument3 pagesPractice Essentials: Simple Febrile SeizureannisaoktovianiNo ratings yet
- Rheumatic Heart Disease by Ajode Dan Matew (Sajoon2011)Document7 pagesRheumatic Heart Disease by Ajode Dan Matew (Sajoon2011)AMOS MELINo ratings yet
- Content Heart DiseaseDocument12 pagesContent Heart Diseaseshifa23No ratings yet
- I. Acute Convulsions:: CNS Tonsillitis Otitis MediaDocument2 pagesI. Acute Convulsions:: CNS Tonsillitis Otitis MediaJinky MonteagudoNo ratings yet
- Infectious Diseases of The HeartDocument84 pagesInfectious Diseases of The HeartHarold DiasanaNo ratings yet
- Symptoms of Pneumonia: o o o o o o oDocument2 pagesSymptoms of Pneumonia: o o o o o o oKathzkaMaeAgcaoiliNo ratings yet
- What Is Dengue Fever?Document30 pagesWhat Is Dengue Fever?Jeanie Rose AlduesoNo ratings yet
- Rheumatic Heart DiseaseDocument13 pagesRheumatic Heart Diseasedy15No ratings yet
- Guideline Summary NGC-9469: RecommendationsDocument6 pagesGuideline Summary NGC-9469: RecommendationsIbrahim MachmudNo ratings yet
- Dengue Paper-2-1Document6 pagesDengue Paper-2-1api-323119914No ratings yet
- RehumaticDocument3 pagesRehumaticgopscharanNo ratings yet
- Rheumatic HeartDocument47 pagesRheumatic HeartsmrutuNo ratings yet
- Rheumatic Heart DiseaseDocument5 pagesRheumatic Heart DiseasejessyNo ratings yet
- Febrile SeizureDocument8 pagesFebrile Seizureanon_944507650No ratings yet
- DengueDocument9 pagesDengueWinna Gonato100% (2)
- What Is Dengue FeverDocument6 pagesWhat Is Dengue Feveroctober_7No ratings yet
- FeverDocument29 pagesFeverYogesh KharcheNo ratings yet
- Blood: Symptoms of Dengue FeverDocument7 pagesBlood: Symptoms of Dengue FeverPrincess Viluan PazNo ratings yet
- EngelzaDocument50 pagesEngelzaGheorghe AntoniaNo ratings yet
- Febrile Seizures: Definition and ClassificationDocument3 pagesFebrile Seizures: Definition and ClassificationArmin AbasNo ratings yet
- Clinical Diagnostics SummaryDocument206 pagesClinical Diagnostics SummaryNeil Naidoo100% (1)
- Lecture 07. Acute Rheumatic FeverDocument39 pagesLecture 07. Acute Rheumatic FeverImanuel Far-FarNo ratings yet
- Eng Medicala004Document6 pagesEng Medicala004Alina-Mihaela MikiNo ratings yet
- Dengue 3Document9 pagesDengue 3Bernadette Collamar Dela CruzNo ratings yet
- NN Disease: Its Symptoms and Treatments (I)Document4 pagesNN Disease: Its Symptoms and Treatments (I)Markus ZahndNo ratings yet
- Dengue Hemorrhagic Fever Nursing Considerations and Nursing Care ManagementDocument5 pagesDengue Hemorrhagic Fever Nursing Considerations and Nursing Care Managementjanns tumanengNo ratings yet
- Assessment of Febrile Seizures in Children: ReviewDocument12 pagesAssessment of Febrile Seizures in Children: ReviewFerdina NidyasariNo ratings yet
- Acute Rheumatic FeverDocument39 pagesAcute Rheumatic FeverUzma BanoNo ratings yet
- Rheumatic FeverDocument27 pagesRheumatic FeverFerrariRoche_14No ratings yet
- Rare Juvenile Primary Systemic Vasculitis What Is It?: WWW - Pediatric-Rheumathology - Printo.itDocument7 pagesRare Juvenile Primary Systemic Vasculitis What Is It?: WWW - Pediatric-Rheumathology - Printo.itcocoramziNo ratings yet
- Signs and Symptoms: Kawasaki DiseaseDocument6 pagesSigns and Symptoms: Kawasaki DiseaseBhebe Ocela PanizaNo ratings yet
- Diseases - What Is Q Fever (Query Fever) What Causes Q Fever (Medical News Today-16 June 2010)Document5 pagesDiseases - What Is Q Fever (Query Fever) What Causes Q Fever (Medical News Today-16 June 2010)National Child Health Resource Centre (NCHRC)No ratings yet
- Biology ProjectDocument13 pagesBiology Projectnalini7723No ratings yet
- What Are The Symptoms?: Swine Flu FactfileDocument6 pagesWhat Are The Symptoms?: Swine Flu FactfileKrishna RajaNo ratings yet
- Acetaminophen Is An Analgesic Used To Temporarily Relieve Minor Aches and PainsDocument7 pagesAcetaminophen Is An Analgesic Used To Temporarily Relieve Minor Aches and Painsmysterious galNo ratings yet
- Cardiopulmonary ResuscitationDocument42 pagesCardiopulmonary ResuscitationVishuNo ratings yet
- PhilosophyDocument3 pagesPhilosophyVishuNo ratings yet
- Protein Energy MalnutritionDocument37 pagesProtein Energy MalnutritionVishu100% (1)
- World Health DaysDocument3 pagesWorld Health DaysVishuNo ratings yet
- VishwasDocument2 pagesVishwasVishuNo ratings yet
- Introduction To Nursing Research: NUR 499 Waynesburg CollegeDocument47 pagesIntroduction To Nursing Research: NUR 499 Waynesburg Collegekaktus420No ratings yet
- Diabetes Mellitus Autoimmune Insulin Beta Cells Pancreas Polyuria Polydipsia PolyphagiaDocument37 pagesDiabetes Mellitus Autoimmune Insulin Beta Cells Pancreas Polyuria Polydipsia PolyphagiaVishuNo ratings yet
- CertificateDocument2 pagesCertificateVishuNo ratings yet
- Conceptual Frame Work For STPDocument1 pageConceptual Frame Work For STPVishuNo ratings yet
- Model 2Document2 pagesModel 2VishuNo ratings yet
- No orDocument2 pagesNo orVishuNo ratings yet
- High Risk New BornDocument36 pagesHigh Risk New BornVishuNo ratings yet
- High RiskDocument42 pagesHigh RiskVishu100% (1)
- Rheumatic FeverDocument3 pagesRheumatic FeverKhalid Mahmud Arifin100% (3)
- Illness ImpactDocument8 pagesIllness ImpactVishuNo ratings yet
- Child To Child ApproachDocument4 pagesChild To Child ApproachVishu100% (5)
- Forgein Bodies PPDDocument22 pagesForgein Bodies PPDVishuNo ratings yet
- Toddler Behavior and Its Problem A SynopsisDocument18 pagesToddler Behavior and Its Problem A SynopsisVishu100% (1)
- Cardiopulmonary Resuscitation (CPR) : Presented byDocument45 pagesCardiopulmonary Resuscitation (CPR) : Presented byVishuNo ratings yet
- Pediatric CPRDocument5 pagesPediatric CPRVishuNo ratings yet
- Burns How To CoolDocument27 pagesBurns How To CoolVishuNo ratings yet
- VishuDocument4 pagesVishuVishuNo ratings yet
- Play TherapyDocument28 pagesPlay TherapyVishu100% (6)
- PhilHealth CF4Document2 pagesPhilHealth CF4B MNo ratings yet
- BisacodylDocument1 pageBisacodylJewel GutierrezNo ratings yet
- AUBF (Quizlet)Document34 pagesAUBF (Quizlet)Allyssa AniNo ratings yet
- Diagnostics: Rare Causes of Arterial Hypertension and Thoracic Aortic Aneurysms-A Case-Based ReviewDocument16 pagesDiagnostics: Rare Causes of Arterial Hypertension and Thoracic Aortic Aneurysms-A Case-Based ReviewBreeze ChloeNo ratings yet
- History and Objectives of Post Marketing SurveillanceDocument14 pagesHistory and Objectives of Post Marketing SurveillanceSohit Gupta100% (1)
- Meddra Important Medical Event Terms List Version 241 enDocument691 pagesMeddra Important Medical Event Terms List Version 241 enLuis Antonio Camacho CamachoNo ratings yet
- Practical MedicineDocument630 pagesPractical MedicineYong Lim80% (5)
- GeriatricsDocument108 pagesGeriatricsQasim AwanNo ratings yet
- Materi Praktikum Pap Smear Modul ReproduksiDocument77 pagesMateri Praktikum Pap Smear Modul Reproduksisusilorini100% (10)
- Wilson Disease - Treatment and Prognosis - UpToDateDocument13 pagesWilson Disease - Treatment and Prognosis - UpToDatericanoy191No ratings yet
- English Robot Script FinalDocument4 pagesEnglish Robot Script FinalKumaresh MuthuNo ratings yet
- Test Bank For Holes Human Anatomy Physiology 16th Edition Charles Welsh Cynthia Prentice Craver DownloadDocument33 pagesTest Bank For Holes Human Anatomy Physiology 16th Edition Charles Welsh Cynthia Prentice Craver Downloadaliciarodriguezswrtpyjemk100% (24)
- Nursing Did You Know FactsDocument1 pageNursing Did You Know FactsmikErlhNo ratings yet
- Nur 1210 Maternal Module #2 Nursing Care of The Pregnant Client (Hemorrhagic)Document21 pagesNur 1210 Maternal Module #2 Nursing Care of The Pregnant Client (Hemorrhagic)aaaaa100% (1)
- Acute Cellulitis and Erysipelas in Adults - Treatment - UpToDateDocument34 pagesAcute Cellulitis and Erysipelas in Adults - Treatment - UpToDateBrian VianaNo ratings yet
- Ananya Deb - 18IUT0290004Document26 pagesAnanya Deb - 18IUT0290004subankar NagNo ratings yet
- Genetic Disorder Brochure ProjectDocument1 pageGenetic Disorder Brochure ProjectErika ContrerasNo ratings yet
- Acute Kidney FailureDocument8 pagesAcute Kidney Failureanimesh pandaNo ratings yet
- Erythroderma PresentationDocument19 pagesErythroderma PresentationSarah Racheal AkelloNo ratings yet
- AntitrombolitikDocument7 pagesAntitrombolitikadityaNo ratings yet
- Institute of Neurosciences Kolkata (Schedule) PDFDocument2 pagesInstitute of Neurosciences Kolkata (Schedule) PDFpvkdasaNo ratings yet
- Review Notes 2000 - Geriatrics PDFDocument12 pagesReview Notes 2000 - Geriatrics PDFeset5No ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakaJendriellaNo ratings yet
- Causes of Erectile Dysfunction As Explained in AyurvedaDocument25 pagesCauses of Erectile Dysfunction As Explained in Ayurvedacharanmann9165No ratings yet
- Soft Tissue SarcomaDocument19 pagesSoft Tissue SarcomaEkvanDanangNo ratings yet
- Difference Between Signs and SymptomsDocument5 pagesDifference Between Signs and SymptomsSitlalin RamosNo ratings yet
- Newborn AssessmentDocument6 pagesNewborn AssessmentAyuni Salleh100% (1)
- Atenolol: Atenolol Is A Beta Blocker MedicationDocument6 pagesAtenolol: Atenolol Is A Beta Blocker MedicationAbdelrhman AboodaNo ratings yet
- Lecture 20 CarcinogenesisDocument84 pagesLecture 20 CarcinogenesisMohammad_Islam87100% (1)
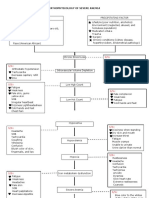
- Pathophysiology of Severe AnemiaDocument3 pagesPathophysiology of Severe AnemiaChrizley Shawn DeroniaNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (28)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No ratings yet
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (58)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)
- Troubled: A Memoir of Foster Care, Family, and Social ClassFrom EverandTroubled: A Memoir of Foster Care, Family, and Social ClassRating: 4.5 out of 5 stars4.5/5 (26)