You might also like
- Qms 035 SampleDocument0 pagesQms 035 SamplenikjadhavNo ratings yet
- Clinical Trials BudgetingDocument52 pagesClinical Trials Budgetingjlbabson100% (5)
- Fertility YogaDocument6 pagesFertility Yoganikjadhav100% (2)
- Roles and Responsibilities of CRO and SponsorDocument33 pagesRoles and Responsibilities of CRO and SponsorShilpi Paliwal100% (2)
- The Duty for Sponor Oversight in Clinical Trials: Practical Guide: 2nd Edition Clinical Data ReviewFrom EverandThe Duty for Sponor Oversight in Clinical Trials: Practical Guide: 2nd Edition Clinical Data ReviewNo ratings yet
- Log Shipping Best PracticesDocument22 pagesLog Shipping Best PracticesnikjadhavNo ratings yet
- Quality Assurance Program PlanDocument128 pagesQuality Assurance Program PlanVictor50% (2)
- 1556-FDA Audit Preparation Checklist - NAV - 03JAN13Document26 pages1556-FDA Audit Preparation Checklist - NAV - 03JAN13Sandeep Somaiya100% (1)
- Annex IV To Guidance For The Conduct of GCP Inspections - Sponsor and Cro en PDFDocument7 pagesAnnex IV To Guidance For The Conduct of GCP Inspections - Sponsor and Cro en PDFMarcM77No ratings yet
- Monitoring Plan TemplateDocument8 pagesMonitoring Plan TemplateSanettezaNo ratings yet
- Clinical Research and PharmacovigilenceDocument22 pagesClinical Research and PharmacovigilenceSharadNo ratings yet
- SITE GEN-001 01 - SOP On Site ActivitiesDocument17 pagesSITE GEN-001 01 - SOP On Site ActivitiesCR Professionals IndiaNo ratings yet
- Audit and Inspection in Clinical TrialDocument57 pagesAudit and Inspection in Clinical TrialRanjeet Prasad100% (2)
- Standard Operating Procedure SOP 305 Creating and Maintaining A Trial Master FileDocument9 pagesStandard Operating Procedure SOP 305 Creating and Maintaining A Trial Master Filemo2bioNo ratings yet
- Quality Control and Assurance in Clinical ResearchDocument5 pagesQuality Control and Assurance in Clinical Researchvmreddi100% (4)
- Standard Operating Procedure For The Recording, Management and Reporting of Adverse Events by InvestigatorsDocument19 pagesStandard Operating Procedure For The Recording, Management and Reporting of Adverse Events by Investigatorsvikram kushwahaNo ratings yet
- SOPDocument5 pagesSOPJaime HinojosaNo ratings yet
- Flowchart vs. Process MapDocument5 pagesFlowchart vs. Process MapDian AbiyogaNo ratings yet
- MedDRA N SOPDocument32 pagesMedDRA N SOPsuri33350% (2)
- Clinical Trial DocumentsDocument37 pagesClinical Trial Documentsapi-37446750% (1)
- SOP 303 SiteInitiationVisitDocument3 pagesSOP 303 SiteInitiationVisitna sarvaNo ratings yet
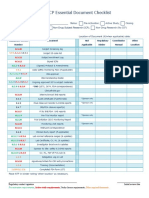
- ICH GCP Essential Document ChecklistDocument2 pagesICH GCP Essential Document ChecklistMohammed Yousffi50% (2)
- Process Validation GonoshyasthoDocument49 pagesProcess Validation GonoshyasthoMillat PharmaNo ratings yet
- Regulatory Binder ChecklistDocument4 pagesRegulatory Binder ChecklistOscar Pompa MeraNo ratings yet
- Monitoring Plan 4 WebsiteDocument5 pagesMonitoring Plan 4 WebsitejohncuyNo ratings yet
- Site FDA Inspection Preparation Checklist v1 (1) .0 22nov10Document9 pagesSite FDA Inspection Preparation Checklist v1 (1) .0 22nov10sreeraj.guruvayoorNo ratings yet
- Standard Operating Procedure Trial Master File and 421 Main Evidence in TheDocument33 pagesStandard Operating Procedure Trial Master File and 421 Main Evidence in Theahmed.bouchenakNo ratings yet
- Konsep GCP Good Clinical PracticeDocument48 pagesKonsep GCP Good Clinical PracticeeuhsahaNo ratings yet
- Good Clinical Practice GuideFrom EverandGood Clinical Practice GuideRating: 5 out of 5 stars5/5 (1)
- Good Clinical PracticeDocument18 pagesGood Clinical PracticeMeenakshi HandaNo ratings yet
- Clinical Trial ChecklistDocument3 pagesClinical Trial ChecklistIzzi FekratNo ratings yet
- GCP Inspection Checklist: I. GeneralDocument10 pagesGCP Inspection Checklist: I. Generalsuhas lavhekarNo ratings yet
- Sop Informed ConsentDocument4 pagesSop Informed ConsentWelzha Meturan-kadmaerubunNo ratings yet
- SOP 40 AD 1 Vendor GCP Compliance Sample Questions V1.0Document2 pagesSOP 40 AD 1 Vendor GCP Compliance Sample Questions V1.0Jaime HinojosaNo ratings yet
- Parenteral Process Validation (1) DarusazDocument30 pagesParenteral Process Validation (1) Darusazeshwar_orgNo ratings yet
- SOP 302 SiteQualificationVisitDocument3 pagesSOP 302 SiteQualificationVisitna sarvaNo ratings yet
- Operational Qualification Report For Syringe Assembling Machine Machine Identification Name: - Report NoDocument3 pagesOperational Qualification Report For Syringe Assembling Machine Machine Identification Name: - Report NoMusyoka UrbanusNo ratings yet
- Sop Title: SOP Version No: 01 Date:: Reviewing and Obtaining Informed ConsentDocument12 pagesSop Title: SOP Version No: 01 Date:: Reviewing and Obtaining Informed ConsentMadhan MohanNo ratings yet
- 05 Ich GCPDocument25 pages05 Ich GCPBhaskar Satya Sankar Balaji100% (1)
- Site FDA Prep CklistDocument15 pagesSite FDA Prep Cklistana.acreis100% (2)
- WWORTH SOP10ProjectManagementV2.2 140507Document21 pagesWWORTH SOP10ProjectManagementV2.2 140507Fery Alapola100% (1)
- CLN-20 00 Investigational Product HandlingDocument4 pagesCLN-20 00 Investigational Product Handlingpopatlilo2No ratings yet
- Cro ChecklistDocument3 pagesCro ChecklistNikhil Jadhav73% (11)
- Audit Findings in Clinical TrialsDocument21 pagesAudit Findings in Clinical TrialsMohit SinghNo ratings yet
- Site Close-Out Visit: Standard Operating Procedures For Clinical Research at Kent State UniversityDocument4 pagesSite Close-Out Visit: Standard Operating Procedures For Clinical Research at Kent State Universityna sarvaNo ratings yet
- Process Validation - SDF - 1 - FDA PDFDocument111 pagesProcess Validation - SDF - 1 - FDA PDFdipakrussiaNo ratings yet
- FDA BIMO ChecklistDocument25 pagesFDA BIMO Checklistnasim50% (2)
- The Monitoring ProcessDocument10 pagesThe Monitoring Processapi-3810976100% (2)
- Standard Operating Procedures For Clinical Research CoordinatorsDocument13 pagesStandard Operating Procedures For Clinical Research Coordinatorsmmohit_990% (1)
- ICH E6-R3 GCP-Principles Draft 2021 0419Document7 pagesICH E6-R3 GCP-Principles Draft 2021 0419ramya sandraNo ratings yet
- Cra GuideDocument17 pagesCra Guidebitterlemon01No ratings yet
- Clinical Trial Monitoring Standard Operating ProcedureDocument14 pagesClinical Trial Monitoring Standard Operating Proceduresreeraj.guruvayoor100% (1)
- Monitoring Plan and Standard Operating Procedure: Protocol TitleDocument5 pagesMonitoring Plan and Standard Operating Procedure: Protocol TitleDipeshNo ratings yet
- Introduction To ICH GCPDocument15 pagesIntroduction To ICH GCPSwapnil BhowateNo ratings yet
- Media Fill ProtocolDocument33 pagesMedia Fill Protocoltetemaestro83% (6)
- Investigators Responsibilities With GCPDocument16 pagesInvestigators Responsibilities With GCPLlosa JuneNo ratings yet
- Essential Documents Checklist Clinical Trial InterventionalDocument3 pagesEssential Documents Checklist Clinical Trial InterventionalPunk Rombus LeeNo ratings yet
- Audit of A TrialDocument7 pagesAudit of A TrialSmita KumarNo ratings yet
- SOP 032 Handling of Non-Compliance v1.1 24 FEB 2017 PDFDocument15 pagesSOP 032 Handling of Non-Compliance v1.1 24 FEB 2017 PDFHaroon RasheedNo ratings yet
- Ethical Issues in Clinical TrialsDocument16 pagesEthical Issues in Clinical TrialsPranjal KothaleNo ratings yet
- CGMP in Clinical InvestigationDocument44 pagesCGMP in Clinical InvestigationrwbbartonNo ratings yet
- Documentation of Clinical Trial Monitoring: A practical guide compliant with Good Clinical PracticeFrom EverandDocumentation of Clinical Trial Monitoring: A practical guide compliant with Good Clinical PracticeRating: 5 out of 5 stars5/5 (1)
- Clsi H15 A3Document51 pagesClsi H15 A3Cristian Gutiérrez VeraNo ratings yet
- Ethical Issues in Clinical ResearchDocument23 pagesEthical Issues in Clinical ResearchDaxesh PatelNo ratings yet
- Sop Title: Assessing Protocol Feasibility: Sop No: Effective DateDocument7 pagesSop Title: Assessing Protocol Feasibility: Sop No: Effective Datetiara rengganis100% (1)
- Pyriproxyfen Papaya Draft ProtocolDocument16 pagesPyriproxyfen Papaya Draft ProtocolprecauteNo ratings yet
- Clinical Trials Audit Preparation: A Guide for Good Clinical Practice (GCP) InspectionsFrom EverandClinical Trials Audit Preparation: A Guide for Good Clinical Practice (GCP) InspectionsNo ratings yet
- Risk Based Quality Management in Clinical TrialDocument15 pagesRisk Based Quality Management in Clinical Trialsreeraj.guruvayoorNo ratings yet
- New Cro Audit FormDocument4 pagesNew Cro Audit FormSiragamSaikumar100% (1)
- Hvac PQDocument24 pagesHvac PQShumaila IftikharNo ratings yet
- Writing Research Protocol - Formulation of Health Research Protocol - A Step by Step DescriptionDocument6 pagesWriting Research Protocol - Formulation of Health Research Protocol - A Step by Step DescriptionCelso Gonçalves100% (1)
- Evaluation of Precision Performance of Quantitative Measurement Methods Approved Guideline-Second EditionDocument52 pagesEvaluation of Precision Performance of Quantitative Measurement Methods Approved Guideline-Second EditionTrần Tiến Đạt100% (2)
- Level of Monitoring v30 1328Document5 pagesLevel of Monitoring v30 1328Josef BreuerNo ratings yet
- Automated Signal DetectionDocument7 pagesAutomated Signal DetectionSutirtho MukherjiNo ratings yet
- Works For Sanofi AventisDocument6 pagesWorks For Sanofi AventisMohit AroraNo ratings yet
- Ora Laboratory Manual: Section 5 Section 5Document30 pagesOra Laboratory Manual: Section 5 Section 5kamamiNo ratings yet
- Risk Assessment For Trial SOPDocument8 pagesRisk Assessment For Trial SOPAsni IbrahimNo ratings yet
- Me Module 3Document28 pagesMe Module 3nikjadhavNo ratings yet
- Rent AgreementDocument6 pagesRent AgreementnikjadhavNo ratings yet
- 2.3. A.1 Facilities and Equipments (Loprazolam 2 MG Tablets, PRIMEGEN Limited)Document3 pages2.3. A.1 Facilities and Equipments (Loprazolam 2 MG Tablets, PRIMEGEN Limited)nikjadhavNo ratings yet
- AmulDocument30 pagesAmulnikjadhavNo ratings yet
- Conditions of Learning (R. Gagne) : OverviewDocument9 pagesConditions of Learning (R. Gagne) : OverviewnikjadhavNo ratings yet
- Log ShippingDocument94 pagesLog ShippingnikjadhavNo ratings yet
- WC 500003981Document211 pagesWC 500003981nikjadhavNo ratings yet
- Configuring EWADocument14 pagesConfiguring EWAnikjadhavNo ratings yet
- PassportApplicationForm Main English V1.0Document1 pagePassportApplicationForm Main English V1.0nikjadhavNo ratings yet
- BRtoolsDocument38 pagesBRtoolsnikjadhavNo ratings yet
- An Overview of AssessmentDocument10 pagesAn Overview of AssessmentnikjadhavNo ratings yet
- NSS - Readme FirstDocument2 pagesNSS - Readme FirstnikjadhavNo ratings yet
- Primer Order - RG Aug 24 2011Document192 pagesPrimer Order - RG Aug 24 2011nikjadhavNo ratings yet
- Data Analysis Chp9 RMDocument9 pagesData Analysis Chp9 RMnikjadhavNo ratings yet
- Nano Applications Start Micro-And Nano - TherapeuticsDocument4 pagesNano Applications Start Micro-And Nano - TherapeuticsnikjadhavNo ratings yet
- Recent Development in T2DM - Review - JP Yadav - 2010Document16 pagesRecent Development in T2DM - Review - JP Yadav - 2010nikjadhavNo ratings yet
- PHD Report Embedded Doc 1-4 - RG - 2011Document1 pagePHD Report Embedded Doc 1-4 - RG - 2011nikjadhavNo ratings yet
- Georges Millers Pyramid RM CHP 4Document1 pageGeorges Millers Pyramid RM CHP 4nikjadhavNo ratings yet
- Applying PatchesDocument16 pagesApplying PatchesnikjadhavNo ratings yet
- Basis BasicsDocument24 pagesBasis BasicsRobson Leal De OliveiraNo ratings yet
- Basis BasicsDocument24 pagesBasis BasicsRobson Leal De OliveiraNo ratings yet
- ABCDocument1 pageABCnikjadhavNo ratings yet
- How To Calculate Oracle DB Performance ParameterDocument23 pagesHow To Calculate Oracle DB Performance ParameternikjadhavNo ratings yet
- Procedure For Processing The Proposal For Utilization of Hazardous Waste Under Rule 9, of HWM Rules 2016Document9 pagesProcedure For Processing The Proposal For Utilization of Hazardous Waste Under Rule 9, of HWM Rules 2016LoveinderNo ratings yet
- CV GraceMorgan-HolmesDocument7 pagesCV GraceMorgan-HolmesKatrina ReyesNo ratings yet
- Transfer of Analytical MethodsDocument3 pagesTransfer of Analytical MethodsBhaskar NapteNo ratings yet
- The CONSORT Statement: ArticleDocument4 pagesThe CONSORT Statement: ArticleiikhsanhNo ratings yet
- Equipment Qualification and Validation of Tablet Compression MachineDocument3 pagesEquipment Qualification and Validation of Tablet Compression MachineRajaSekhararayudu SanaNo ratings yet
- Cleaning Validation ProtocolDocument3 pagesCleaning Validation Protocolpuneetogupta100% (1)
- Commentary To Ag:Pt/T101 - Method of Sampling Polymer Modified Binders, Polymers and Crumb RubberDocument8 pagesCommentary To Ag:Pt/T101 - Method of Sampling Polymer Modified Binders, Polymers and Crumb RubberMEHDI FARROKHINo ratings yet
- NelsonLabs TechConsult ExamplesDocument3 pagesNelsonLabs TechConsult ExamplesNancy LonnrothNo ratings yet
- Protocol For Validation of Test Method For Assay ofDocument16 pagesProtocol For Validation of Test Method For Assay ofAsaikkutti AnnamalaiNo ratings yet
- Bmjopen 2019 034828Document9 pagesBmjopen 2019 034828Nindie AulhieyaNo ratings yet
- TDR Competency Wheel by WHODocument1 pageTDR Competency Wheel by WHOachint8kumarNo ratings yet
- Audits & Inspections CRO Perspective: DR - Prashant BodheDocument74 pagesAudits & Inspections CRO Perspective: DR - Prashant BodheJayanta DasguptaNo ratings yet
- How To Write A ProtocolDocument8 pagesHow To Write A ProtocolMohamed SalemNo ratings yet
- Part 1: Introduction Part 2: QA and Monitoring Role Part 3: Trial Monitoring Activities Part 4: Summary of Key PointsDocument12 pagesPart 1: Introduction Part 2: QA and Monitoring Role Part 3: Trial Monitoring Activities Part 4: Summary of Key PointsRenzo FernandezNo ratings yet
- EUROLAB Cook Book - Doc No 17 Interlaboratory Comparison - The Views of Laboratories - Rev. 2017Document3 pagesEUROLAB Cook Book - Doc No 17 Interlaboratory Comparison - The Views of Laboratories - Rev. 2017Pataki SandorNo ratings yet