Professional Documents
Culture Documents
NURSE 100 Course Info Medical Packet
Uploaded by
sygexCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
NURSE 100 Course Info Medical Packet
Uploaded by
sygexCopyright:
Available Formats
NURSE 100 NURSE ASSISTANT
COURSE INFORMATION AND MEDICAL PACKET
FALL 2012
Professor J. Young BHS, MHA, RN
youngj@arc.losrios.edu
American River College
Nursing Department
4700 College Oak Drive
Sacramento, CA 95841-4217
Telephone No: (916) 484-8206
NURSE 100 INFORMATION PACKET
Table of Contents
Welcome Letter and Mandatory Orientation Information ............................................................................................. 3
Student Fees and Supply Checklist for NURSE 100 .................................................................................................. 4
How Does a Roster or Waitlist Student Secure A Seat in the NURSE 100 Class? ..................................................... 5
How Does a Student Lose Eligibility to Be in the NURSE 100 Class? ........................................................................ 5
Explanation of Required Prerequisites for the NURSE 100 ........................................................................................ 6
English Prerequisite for NURSE 100 .......................................................................................................................... 7
Assessment Center .................................................................................................................................................... 8
NURSE 100 Course Information & Syllabus ............................................................................................................... 9
NURSE 100 Nurse Assistant Class Schedule .......................................................................................................... 12
Pre-class Mandatory Assignments ........................................................................................................................... 13
Assignment #1 Complete the reading assignments listed for the first seven (7) days ................................. 13
Assignment #2 Watch the Skills CD that comes with the textbook. ............................................................. 15
Assignment #3 Memorize the required Medical Abbreviation List ................................................................ 16
Assignment #4 Memorize the required Vital Signs and VS Characteristics ................................................. 17
Commitment for Success .......................................................................................................................................... 18
ARC Student Access Card / Clinical Name Tag Information ..................................................................................... 19
Supplying Social Security Number (Disclosure Statement) ...................................................................................... 20
Disqualifying Penal Codes ........................................................................................................................................ 21
Live Scan Fingerprints .............................................................................................................................................. 23
ARC Campus Map .................................................................................................................................................... 24
Medical Clearance: Print out the ARC medical forms (4 pages) located at the end of this packet ............................ 26
A. Health Clearance Checklist
B. Health History
C. Physical Exam
NURSE 100 - NURSE ASSISTANT
GENERAL INFORMATION
Welcome and thank you for your interest in the NURSE 100 Nurse Assistant class! The objective of the nurse assistant class is to teach the
student theory information that supports giving safe and thorough hands-on care to elderly residents who live in a long-term care facility. The
course is designed to incorporate theory knowledge with skill practice followed by hands-on clinical experience.
Students will learn basic care giving procedures and effective therapeutic communication measures. Students will also learn the theory of
conditions related to normal aging, common illnesses of the elderly as well as how to recognize and protect resident rights. At course completion,
the student will receive an ARC certificate of successful completion. The course is specifically designed to prepare the student to take the Nurse
Assistant exam to become a Certified Nurse Assistant in the state of California.
MANDATORY ORIENTATION FOR NURSE 100 AND ENGLISH PREREQUISITE SUBMISSION
Date: Tuesday, July 17, 2012
Time: 1:00 pm 2:00 pm English prerequisite requirement must be submitted during this time. (Students on the roster may also submit
medical requirements, if complete.)
2:00 pm 3:30 pm (Mandatory orientation meeting begins promptly at 2:00 pm).
Location: HEED Room 710 Note: Look for direction signs.
VITAL INFORMATION ABOUT ORIENTATION AND ENGLISH PREREQUISITE SUBMISSION
The orientation is a mandatory meeting for registered students and waitlisted students.
No student can enter the NURSE 100 class without having first submitted the English requirement on time.
No student can enter the NURSE 100 class without having first attended the entire pre-class mandatory orientation.
No late English prerequisite submission will be accepted and no late admittance to the orientation meeting will be permitted. Be on time!
FIRST CLASS
Time: 12:00 noon
Date: Monday, August 27, 2012
Location: HEED Room 716 (Parking is difficult at 11:45. Come and park early to be to class on time.)
Instructions: Attendance at the first class is mandatory. Students not present at the beginning of the first class will be dropped from the
class to allow a waitlisted student to add. Be sure to review the NURSE 100 Course Syllabus Attendance Policy.
Come to the first class with:
1. Textbook (listed in the course syllabus)
2. Having completed the four (4) pre-class assignments. Assignments are in this packet.
3. Class Supplies (listed in course syllabus)
4. $10.00 for mobile fingerprint convenience fee
THEORY CLASSES
Time: 12:00 pm - 4:50 pm
Location: HEED Room 716
CLINICAL LABS
Time: 12:00 pm - 8:05 pm
Location: Manor Care in Citrus Heights
Instructions: Clinical information will be given during the first week of class
STUDENT/INSTRUCTOR CONTACT
Students must activate their ARC iMail account. Students may contact instructor by email with specific questions or concerns.
-3-
Professor J. Young, BHS, MHA, RN
Office 740
Phone Number: (916) 484-8206
Email: youngj@arc.losrios.edu
STUDENT CHECKLIST FOR NURSE 100
1. Student Tuition
Current cost /unit? Go to ARC Home Website. Click on fees. Fees must be paid at time of registration.
ARC computer system will automatically drop students for non-payment of fees.
If automatic drop occurs, the student cannot be added back into the class.
2. Activate your ARC iMail account. This format is used to email students.
3. Tuberculin Skin Test
$5.00 if obtained at the ARC Student Health Center. Call 484-8383 for office hours and TB appointment.
4. Physical Exam
Must be obtained from your private MD or other medical source.
Must be completed using the Nurse Assistant medical form attached at the back of this packet.
5. Fingerprint Mobile Convenience Fee
$10.00 - Submit to instructor during week one of class. DOJ processing fee - no cost to the student.
6. Student Access Card It is your name identification card for clinical. Obtain during week one of class.
7. Course Textbook Textbook information is found in the course syllabus. Cost? Bookstore Website
8. Pre-class Assignments
1. Student must come the first class having already read the required pre-class reading assignment.
2. Memorize the normal vital sign [VS] ranges, and normal characteristic. A VS exam will be given first week of class
3. Study the medical abbreviations used in the CNA class. Pre-class assignments are in this information packet.
9. Three ring binder 1.5 in - 2.0 in and Black ink pen non-erasable, and Highlighter any color
10. 2-3 pencils with erasers that erase cleanly and, 4 Scantrons - #882 E for class exams
11. Disposable non-latex gloves for skill labs - 1 box $3.50 - $5.00. You will need by third week of class.
12. AQuick release@ gait belt Purchase from ARC student store - approx $10.00. Ask for the Aquick release@ belt.
13. Fanny Pak black, blue or white Buy small to medium size pouch. cost varies between $7.50 - $12.00.
14. Breath mints or breath spray (optional). Keep in clinical fanny pak. NO GUM
15. Personal size hand sanitizer (optional). Keep in clinical fanny pak.
16. Personal size hand cream (optional). Keep in clinical fanny pak.
17. Small nail file with nail cleaner tip (optional). Keep in clinical fanny pak.
18. Clinical Shoes - white with white shoe laces. Tennis shoe with a minimal secondary color is OK.
Shoes must be closed heel and closed toe. Shoes must be washable shoes.
19. Clinical White scrub-type top with pockets
If you wear a tee shirt under your uniform top it must be short sleeved, white, and have no logos on it.
20. Clinical White scrub-type long pants. No crop pants.
21. Socks or trouser stockings must be a solid neutral color such as white, beige, or brown.
22. Clips, elastic bands, hair spray etc. Hair must be up, off of shoulders and secured back, off of face.
No side tendrils or long bangs.
23. Small stud earrings - one earring in each ear lobe. No other jewelry is allowed.
24.
Wrist Watch with a Second Hand is mandatory for this class and must be worn to every clinical.
No bracelets or necklaces are allowed. Exception: medical alert bracelet
25. Large Safety Pin about 1" long. You will apply to underside of uniform top at shoulder and clip your name tag to it.
26. Malpractice Insurance $5.00 - Pay fee at business desk in main administration building after week one.
Bring your receipt to Professor Young by Wednesday of week two.
27. State Exam Fee $90.00 - You must submit a $90.00 money order or cashiers check to Professor Young about the
3r
d
week of class. NO Cash, NO personal checks. Make your check payable to Red Cross - CNA Testing. The $90.00 is
non-refundable.
28. College Parking - $1.00 / day or you may purchase a semester pass from the business office for approx $30.00.
29. Child Care - Students must obtain their own child care. Children are not allowed in the classroom. Check out ARC Child
Development Center. For information call 484-8651.
30. Transportation: Student must provide own transportation to class and to clinical. To purchase a Universal Transit Pass,
go to the business services counter at the administration building.
-4-
This page is done as a courtesy for students. Some of the following fees are approximated and may change. Updated information may be found
at: http://www.arc.losrios.edu/ 0u|ck L|nks AR6 webs|te |ndex
How Does a Roster or Waitlist Student
Secure a Seat in the NURSE 100 Class?
Students must:
1. Sign In and submit the required English prerequisite.
English requirement information is located on page 7 of the NURSE 100 Course Information Packet
English prerequisite is due on the day of the mandatory orientation.
One hour before the orientation, a table will be set up in the lab room adjoining HEED Room 710 for
sign-in and English prerequisite submission.
Submit copies only. Never submit your originals. Make copies before you come to the orientation.
Look for direction signs as you approach HEED Room 710.
Students who arrive late may not be admitted to the orientation meeting.
2. Attend the full NURSE 100 Mandatory Orientation Meeting Be on Time!
NOTE: There is no admittance to the orientation meeting after it starts.
Date: Tuesday, July 17, 2012
Time: 1:00 pm: Doors open for English submission and orientation sign-in
Time: 2:00 pm 3:30 pm: Mandatory Orientation
Location: HEED Room 710
Bring: A printed copy of the NURSE 100 Course Information and Medical Packet
How Can a Student Lose Eligibility to Be
in the NURSE 100 Class?
A roster or waitlist student who fails to submit the following requirements will lose eligibility to enter the
NURSE 100 CLASS:
1. Failure to submit complete and correct English prerequisite requirement(s) on time and/or
2. Failure to sign in before the mandatory orientation, and/or
3. Failure to attend the full mandatory orientation, and/or
4. Failure to provide correct or updated contact information to instructor, and/or
5. Failure to submit complete medical clearances on time
6. Failure to be present and on time for the first class
Students must activate their ARC iMail account. Prior to beginning of class, instructor communication with student
will be by email. Students are expected to check their iMail account regularly for messages and reply to the instructor
in a timely manner. If you have questions, it is best to email the instructor.
-5-
Professor J. Young, BHS, MHA, RN
Office Phone Number: (916) 484-8206
Email: youngj@arc.losrios.edu
EXPLANATION OF REQUIRED PREREQUISITES FOR NURSE 100
Submissions Will Not be Returned to the Student.
Submit Copies Only. Do Not Submit Originals.
1. English Competency
Submit a photocopy of completed English prerequisite.
See English Prerequisite table in this packet to determine what you need to submit.
If you are submitting transcripts, highlight your name and the courses that meet the NURSE 100 English
requirement. The English prerequisite is due on the day of the mandatory orientation. See page 3 for submission
information.
2. Health Clearance Checklist
Print the Health Clearance Checklist and complete the upper section only. Student will turn in this form along with health
requirements.
3. Physical Exam (PE)
Student must print the Nurse Assistant Program Health History. Complete form in its entirety. Sign and date.
Print the Physical Exam. Complete the upper section. Sign and date.
Medical health care provider will complete the physical exam section and review students completed Health History.
Medical provider must sign and stamp both the physical exam section and the students completed Health History.
Students must be mentally and physically willing and able to fully participate in the class.
There are no accommodations for restricted or limited participation.
Physical exam must be within the last one (1) year prior to the beginning of the class.
4. Tuberculin Skin Test (PPD) Clearance
TB skin test (PPD) must be done within the last 6 months prior to the beginning of the class.
TB skin test (PPD) results must be documented as negative.
Student must submit copy of written PPD report that is signed and dated by the medical health provider
OR
Chest X-ray
Chest X-ray test must be done within the last 1 year prior to the beginning of the class.
Chest X-ray test results must be documented as negative or no evidence of active disease
Student must submit copy of written Chest X-ray report that is signed by the medical health provider
Need to clarify information? Email the instructor at youngj@arc.losrios.edu before the deadline. -6-
Medical Paperwork Submission for Roster Students Date and Time:
1. Roster students are encouraged to submit copy of Physical Exam [PE] and/or copy of Tuberculin [TB] clearance with
copy of English prerequisite on the day of the orientation, if completed.
2. Medical prerequisites are due no later than 12:00 pm on Wednesday, August 1, 2012.
3. Take submissions to HEED Nursing Dept Room 731. Have your copies ready to submit. Office staff will not make copies
for you. NEVER submit your original forms. Retain them in your home files.
4. Call to confirm office hours and staff availability at 484-8873 before coming on campus. Medical forms will be stamped
with date and time when submitted.
Medical Paperwork Submission for Waitlisted Students:
1. Waitlisted students must submit medical clearances within 2 weeks of being offered an open seat. The instructor will
assign the due date.
2. To submit medical paperwork, follow Steps 3 and 4 above.
3. Submissions will be accepted no later than 12:00 pm on the due date assigned to the student by the instructor.
4. After medical requirements are submitted, the student will be issued a class add permission number from the instructor.
NOTE: Any prerequisites submitted for NURSE 100 are for this class only. Students registered for NURSE 101 are required to
turn in a separate set of copies at a later date. See NURSE 101 on nursing website.
ENGLISH PREREQUISITE TABLE FOR NURSE 100
Students must submit written proof of the following English prerequisites or assessment test results before
they can be considered for the NURSE 100 Nurse Assistant course.
Students may meet the English prerequisite by either:
Section A - Completing the Acceptable English course(s) OR
Section B - Placement through the ARC Assessment Process
A.
ACCEPTED ENGLISH COURSES
B.
PLACEMENT THROUGH ASSESSMENT PROCESS
Student selects 1, 2, 3, OR 4 below and
Student must submit unofficial transcripts
highlighting completed English prerequisites or
AA/AS degree
Students selects 1, 2, OR 3 below, and
Students must submit copies of test results from
ARC Assessment Center (484-8423), and
Assessment recommendations must reflect
eligibility/placement into the courses listed below.
1. ESLR 40 and ESLW 40 and ESLL 40 1.
Eligibility for ESLR 50 and ESLW 50 and
ESLL 50
2. ENGWR 51 and ENGRD 15 2.
Eligibility for ENGWR 102 and ENGWR 103 and
ENGRD 116
3.
ENGRD/ENGWR 56 or
Higher Reading/Writing level class
4.
AA/AS degree diploma or higher degree
diploma
-7-
ASSESSMENT CENTER
The Assessment Center provides a variety of testing services. Basic skills testing is recommended for prospective students.
The Chemistry test is recommended for students who wish to enroll in CHEM 400. Test results, along with other
criteria, are used by counseling to determine readiness for specific courses and programs. Competency testing for the
AA/AS Degree and Ability-to-Benefit testing are also available through the Assessment Center. There is no fee for
testing. Results are available immediately after the test. ESL results are available in 3 working days.
Students must complete the online college application process and have a student ID number prior to testing or
assessment.
Testing is on a walk-in basis. No appointments are necessary. Please see the Testing Calendar for testing dates and
times. Assessment Center telephone number (916) 484-8423.
Students needing special accommodations for testing should call the DSP&S office at (916) 484-8382.
Basic Skills Testing
Basic skills tests/assessments are recommended for all first-time college students and those who plan to enroll in
reading, writing, ESL (English as a Second Language) or math courses.
English The English test measures reading and writing skills. The first section is composed of passages
followed by questions regarding the content. In the second section, students will identify sentence and
grammar errors and identify logical sentence choices. In the last section, students are given sentences
with words missing and are asked to fill in the blanks with the correct answer. All three sections must be
taken for either reading or writing courses. It is administered on the computer and is timed. Only ONE
attempt is permitted. English sample test.
English as a Second Language The ESL test is for students whose native language is not English and
who wish to enroll in ESL classes. It is composed of four sections. Listening, reading, and grammar are
administered on the computer and are not timed. Writing (essay) is timed for 30 minutes. Students
should allow approximately 3 hours. Only one attempt is permitted. ESL sample test.
Documents/Support_Services/Assessment/EslSampleTest.pdf
Office Location: Student Services Bldg.
Hours: Fall, Spring and Summer Semester:
M, Th, F 8:00 am 5:00 pm
Tu, W 8:00 am 7:00 pm
The First Week of the Fall and Spring Semester:
M - Th 8:00 am 8:00 pm
F 8:00 am 5:00 pm
College Vacation Periods and Semester Break Periods:
M - F 8:00 am 5:00 pm
Note: Testing times vary from office hours.
-8-
AMERICAN RIVER COLLEGE
4700 College Oak Drive
Sacramento, CA 95841-4217
NURSE 100 - NURSE ASSISTANT
COURSE INFORMATION & SYLLABUS
COURSE UNITS: 6 Units
COURSE INSTRUCTOR: Professor J. Young, BHS, MHA, RN, Nursing Professor, American River College
THEORY: Theory time is 12:00 pm 4:50 pm
See class schedule for theory days.
Theory classes meet on campus in classroom HEED 716 unless student is otherwise notified.
CLINICAL: Clinical time is 12:00 pm 8:05 pm
See class schedule for clinical days.
INTENDED STUDENT BODY
1. Student seeking course work to prepare and qualify for California state certification as a Certified Nurse Assistant (CNA).
2. Student age 18 or older.
3. Student without recorded felony conviction. Minor traffic violations are acceptable. Students with a previous conviction
must obtain and show documented proof of rehabilitation clearance obtained through the Department of Health Services
(DHS) before beginning the course. Disqualifying Penal Code Sections available in orientation packet.
4 Student who is free from tuberculosis. TB test clearance within last 6 months or chest x-ray clearance within last 12
months required.
5. Student who is physically and emotionally able to meet theory and clinical course objectives. Physical examination within
the last 12 months is required. Student must be able to meet course objectives without limitations.
6. Student who is able to speak (converse), read, write, comprehend, listen and respond to English appropriately at a
minimum 6
th
grade level.
MAJOR GOALS OF THE COURSE
This course is designed to fully prepare the student for the State of California Certified Nurse Assistant (CNA) certification
examination.
Goals are:
1. To provide information on the provision of nursing care at the nurse assistant level with focus on safety, communication,
rehabilitation, dignity, privacy, independence, infection control, and the elements of physical and psychosocial needs of
the senior adult resident.
2. To provide student with a basic understanding of illness and the effect of illness on the adult individual and the family.
3. To provide opportunity for supervised practice of skills to assist the patient with the activities of daily living.
4. To provide a variety of teaching methods to assist student to learn and retained the required CNA units of instruction.
CLINICAL UNIFORM (ALL WHITE)
1. Uniform may be purchased at any uniform shop, as well as Wal-Mart, K-Mart, Target, etc.
2. White short sleeve scrub top. A long sleeve or short sleeve white tee shirt may be worn underneath top (no print or logos
on undershirt).
3. White long pants or white skirt (A-line, below the knee skirt). Long pants are advisable. Uniform must be clean and without
wrinkles for clinical.
4. White closed-toe and closed-heel shoes. No pumps or high heels. Shoes should be washable.
5. Nylons with skirt or white stockings or socks with long pants.
-9-
CLINICAL REGULATIONS THAT PROMOTE PROFESSIONALISM
1. Hair must be clean and neatly fixed, secured up and off of the uniform collar.
2. No perfumes or strong-perfumed body lotions.
3. No jewelry other than wedding band and wrist watch. Wrist watch with a second hand is mandatory.
4. Earrings are limited to two (one each ear lobe) and they must be studs.
5. Fingernails must be short (finger tip length) smooth and clean. Artificial nails are prohibited. Fingernail polish is prohibited.
6. Name badge must be worn to every clinical session. Your student access card is your name tag.
7. White, blue, or black fanny pack is required to hold clinical supplies.
8. Student must sign a pre-clinical agreement before caring for residents.
ASSIGNMENTS: Reading assignments are required for each module and can be found on the course calendar.
MAJOR UNITS OF INSTRUCTION
Introduction Safe Environment The Resident in Long Term Care
Nutrition Rehabilitative Nursing Death and Dying
Residents Rights Medical and Surgical Asepsis Weights and Measures
Body Mechanics Emergency Procedures Observation and Charting
Interpersonal Skills Vital Signs
INSTRUCTIONAL STRATEGIES
Students will learn through lecture, demonstration, class discussions, small group study, media presentations, skill lab practice,
and clinical experiences.
COURSE REQUIREMENTS
1. Complete and submit pre-exam study guides per written instruction. Failure to meet the requirement will result in the
student being is allowed to take corresponding exam and result in course failure.
2. Earn 70% or greater on each exam. Four (4) multiple choice exams and one (1) medical abbreviation exam are given.
Less than 70% on any one exam will result in course failure. Cheating is not allowed. A student who cheats on an exam
will be terminated from the class immediately.
3. Successfully complete clinical experience. Provide resident with safe, private, dignified care. Meet infection control and
effective communication measures, and encourage resident's independence. Clinical is evaluated as a Pass-Fail
experience. Students must pass both clinical and theory to successfully complete the course.
REQUIRED COURSE MATERIALS (All required items may be purchased at the college bookstore).
1. Mosby's Textbook for Nursing Assistants, 8
th
Ed, Soft Cover,
Sorrentino & Remmert, Mosby, 2011
2. Binder: 2"- Three-ring binder
3. Highlighter pen: any color
4. Note taking material
5. Black ink pen (non-erasable)
6. One box of disposable exam gloves (non-latex)
7. #2 pencil with eraser
8. Four Scantrons 100 # 882-E
9. "Quick release" gait belt
10. ARC Student Access card (name card)
ACTIVE PARTICIPATION
To successfully complete NURSE 100 the student will actively participate in all of the following:
1. Classroom theory days (1 absent day allowed) and
2. Clinical experience days (1 absent day allowed) and
3. Campus skill labs. Skill labs are mandatory - No student will be allowed in clinical who has not met this requirement.
NOTE: No greater than 3 late occurrences overall (for both theory and clinical)
-10-
A = 90 - 100% of total points
B = 80 - 89% of total points
C = 70 - 79% of total points
F = 69% and below of total
ATTENDANCE POLICY - LATE / ABSENT
There is no scheduled make-up time for missed Theory or missed Clinical classes. This is a work preparatory course. Timeliness,
attendance, and active participation are essential. Plan your personal obligations on non-class hours. Class = both theory and
clinical classes
Late means:
a. Failure to be in class by scheduled start time and up to 10 minutes past start time = 1 late event
b. Failure to be in class between 10 to 20 minutes after scheduled start time = 2 late events
c. Leaving class 1 minute to 10 minutes before scheduled stop time (without instructor dismissal) = 1 late event
d. Leaving class from 10 minute to 20 minutes before scheduled stop time (without instructor dismissal) = 2 late events
e. Not returning to class on time at end of break time = 1 late event (break times will be announced in class)
Absent means:
f. Not in class within 20 minutes after scheduled start time = 1 absent day
g. Leaving class 20 minutes or more before scheduled stop time (without instructor dismissal) = 1 absent day
Late and Absent Policy:
h. Clinical absence is counted as one full class day only (no partial day absent time)
i. Theory absence is counted as one full class day only (no partial day absent time)
j. Student must notify instructor of intended absence.
Administrative withdrawal I drop from the course may occur - Clinical and Theory:
k. At beginning point of 4
th
late event
l. At the beginning point of 2
nd
theory or clinical absent day
NOTE: If 4
th
late event or 2
nd
absent day occurs after last date to drop course without penalty, the student will
receive an F grade.
SLEEPING IN CLASS
Sleeping or appearing to sleep in class is not acceptable. Eyes must remain open and student must actively participate in class.
Students who sleep or appear to sleep in class will be dismissed for the remainder of the class day and an absent day will be
assigned.
AT SUCCESSFUL COMPLETION OF NURSE 100
1. Student will have earned the opportunity to take the California State Certified Nurse Assistant exam.
2. Student will receive an ARC certificate of successful course completion.
CELL PHONES
Use of cell phone is prohibited in the theory classroom and in the clinical facility even in the vibrate mode. Cell phones MUST be
kept in the "OFF" mode. Cell phones may be used outside of the classroom and outside of clinical facility during scheduled
breaks. Program termination will result if student does not adhere to cell phone regulations.
CLASS RE-ENTRY
A student may have one re-entry into the NURSE 100 class.
STUDENT LEARNING OUTCOMES
The course content that the student is expected to learn will be given and explained on the first day of class.
STUDENT CONTACT
Students must activate their ARC iMail account. Prior to beginning of class, instructor communication with student will be by
email. Students are expected to check their iMail account regularly for messages and reply to the instructor in a timely manner.
Email the instructor with questions or concerns.
-11-
Professor J. Young, BHS, MHA, RN
Office HEED 740 Phone Number: (916) 484-8206
Email: youngj@arc.losrios.edu
Theory days: A schedule of the instructor's office hours for theory days will
be given to students on first class day.
Clinical days: Office hours for clinical days are embedded into the clinical
day. Instructor will not be on campus.
NURSE 100 NURSE ASSISTANT SCHEDULE
FALL 2012 CLASS SCHEDULE
Instructor: Professor Judy Young, MHA, RN
(916) 484-8206
Email: youngj@arc.losrios.edu
Students are required to notify the instructor of absence or late arrival to theory or clinical.
No call or No show = Drop from class
Theory = Theory Class 12:00 pm 4:50 pm
13 Theory days
Theory classes are held in HEED Room 716
Clinical = Clinical Lab 12:00 pm 8:05 pm
14 Clinical days
Skills Practice Lab: HEED Room 714
Clinical Experience Site: Manor Care, Citrus Heights
Monday Tuesday Wednesday Thursday Friday
1 8-27 Theory - 1 8-28 Theory - 2 8-29 Theory - 3 8-30 Theory - 4
2 9-3 Holiday 9-4 Theory - 5 9-5 Clinical - 1 9-6 Clinical - 2
3 9-10 Theory - 6 9-11 Theory - 7 9-12 Clinical - 3 9-13 Clinical - 4
4 9-17 Theory - 8 9-18 Theory - 9 9-19 Clinical - 5 9-20 Clinical - 6
5 9-24 Theory - 10 9-25 Theory - 11 9-26 Clinical - 7 9-27 Clinical - 8
6 10-1 Theory - 12 10-2 Clinical - 9 10-3 Clinical - 10 10-4 Clinical - 11
7 10-8 Theory - 13 10-9 Clinical - 12 10-10 Clinical - 13 10-11 Clinical - 14
-12-
-13-
TBC = Textbook Chapter
pg(s) = Textbook Page(s)
PRE - CLASS ASSIGNMENT #1
Required Textbook:
Mosbys Textbook for Nursing Assistants Softcover
Sorrentino & Remmert, 8
th
Edition, 2011 ISBN 9780323080675
This is the first of the pre-class assignments to be completed by the first day of class. Students are required to read the assigned textbook chapter (TBC) pages
(pgs) for Days 1 to 7 before the first day of class. As there is a considerable amount of reading, be sure to give yourself plenty of time to complete the assignment.
Be Sure to Answer Questions At the End of Each Chapter!
DAY 1
Module 1 Introduction TBC 1, 3 - 5 pgs 1 - 11 & 21 - 62
A. Role and Responsibilities of the Certified Nurse Assistant
B. Title 22, Division 5, California Code of Regulations
C. Requirements for Nurse Assistant Certification
D. Professionalism
E. Ethics and Confidentiality
F. Harassment
Module 6 Medical & Surgical Asepsis TBC 15 pgs 212 - 243
A. Micro-Organisms
B. Universal Precautions
C. Basic Principles of Asepsis
Module 9 Patient Care Procedures TBC 19 pgs 304 - 319
A. Bedmaking
Module 3 Interpersonal Skills TBC 6 & 8 pgs 63 - 78 & 89 - 104
A. Communications
Dealing with Conflict
Verbal and Non-Verbal
B. Defense Mechanisms
C. Socio-Cultural Factors
D. Attitudes: Illness/Health
E. Family Interaction
REMINDER: Vital Sign Memorization (Pre-Class Assignment #4). Memorize VS exactly as written including pulse and respiratory characteristics and unit of
measurements for all VS.
DAY 2
Module 4 Safe Environment TBC 12 - 14 pgs 149 - 211
A. General Emergency
Safe setting and Accident Risk Factors
B. Safe Environment:
Workplace Violence
Incident Report
Hazardous Substance
MSDS
Wheel Chair Safety
Electrical Equipment
Hand Rails
Gait Belts
Resident=s Unit / Room
C. Fire Safety
Oxygen Safety
Disasters
Falls
Assistive Devices: Cane, Walker
Restraints
Module 4 Safe Environment (Cont.)
D. Heimlich Maneuver
E. Client Safety Codes
Module 14 Rehabilitation Nursing TBC 11 & 38 pgs 135 - 149 & 640 - 648
A. Promoting Resident=s Potential - Promoting Independence
Restraints & Alternatives
B. Devices and Equipment:
W/C, Cane, Walker, etc.
Ambulation
C. Activities of Daily Living
Rehabilitation and Restorative care
D. Family Interactions
Rehabilitation Nursing TBC 28 pgs 509 - 519
A. Comfort, rest, sleep
DAY 3
Module 14 Rehabilitation Nursing TBC 27, 32, & 34 pgs 491 - 508 &
pgs 569 - 571, 593 - 604
E. Complications of Inactivity:
Range of Motion (ROM)
Orthostatic Hypotension
Pressure Wounds
Positioning and Protective Measures
Stimulating Circulation
Benefits of Leg Exercises
TED Hose (Elastic Stockings)
Thrombi and Emboli
Module 5 Body Mechanics TBC 16 - 17 pgs 244 - 286
A. Basic Rules of Body Mechanics
Anatomy & Physiology
B. Transfer Techniques
Positioning Techniques
C. Ambulation
D. Body Mechanics
Ergonomics
Work-Related Musculoskeletal Disorders
Module 2 Patient Rights TBC 2 pgs 12 - 33
A. Resident Rights:
Ombudsman Program
B. Health & Safety Code: OSHA
Environmental Requirements
C. Code of Federal Regulations, Resident Rights
Module 10 Vital Signs Requirement (VS) TBC 26 pgs 466 - 488
In class: Vital Sign Memorization Test
Student must earn 100% to pass. No partial credit
Module 16 Death & Dying TBC 52 pg 830
C. Rights of the Dying Patient
-14-
TBC = Textbook Chapter
pg(s) = Textbook Page(s)
Pre-Assignment #1 (Continued)
Be Sure to Answer Questions At the End of Each Chapter!
DAY 4
Module 8 Patient Care Skills: Personal Hygiene TBC 20, pgs 320 - 330
C. Oral Hygiene
Conscious and Unconscious
Denture Care
Module 11 Nutrition TBC 24 - 25, pgs 425 - 465
A Proper Nutrition
B. Feeding Techniques
C. Diet Therapy
Alternate Feeding
Aspiration
Module 9 Patient Care Procedures TBC 24 - 25
C. Intake & Output
Fluid Balance
Special Procedures TBC 35, pgs 605 -612
A. Heat and Cold Application
DAY 5
Module 12 Emergency Procedures TBC 51, pgs 799 - 821
(See also individual pages listed)
Rules of ER Care: Know Your Limits pg 800
B. Immediate & Temporary Intervention
Recovery Position pg 809
Choking pgs 162 - 164
Hemorrhage pg 816
Hypovloemic Shock
Toxic Shock
Fainting (Syncope)
Stroke pg 681
Seizure pg 813
Burns pgs 157 & 819
Heart Attack pg 700
Respiratory Distress pgs 616 & 702
Module 8 Patient Care Skills: Grooming TBC 21 & pgs 363, 361, & 354
D. Nail Care
D. Shaving
D. Hair Care
Non-Medicinal Shampoo
Medicinal Shampoo
Module 8 Patient Care Skills TBC 20 pgs 331 - 333, 346 - 350, 344 - 345
A. Bathing
Complete and Partial Bed Bath
Medicinal Baths
Peri Care
Shower
Back Massage
DAY 6
Module 15 Observation & Charting TBC 5 p 66 - 70
A. Observation & Reporting Responsibility
B. Resident Care Plan
C. Documentation
D. Legal Issues of Charting
Module 8 Patient Care Skills TBC 21 p 366 - 374
B. Dressing (and Undressing)
Module 8 Patient Care Skills TBC 29 p 526 - 529
I. Height & Weighing Measurement
Measure Length of Bed Bound Resident
Module 7 Weights & Measures TBC 5 p 69
C. Military Time: 24 Hour Clock
In class lecture and practice
DAY 7
Module 8 Patient Care Skills: Elimination Needs TBC 22 & 44,
pgs 375 - 405 pg 719
G. Urination
Bladder Retraining
Urinary Disorders
Module 8 Patient Care Skills: Elimination Needs TBC 23 & 43,
pgs 406 -424 & pg 710
H. Bowel Movement Ostomy Care
Bowel Retraining Digestive Disorders
Module 23 Patient Care Procedures Pgs 414 - 420
E. Cleansing Enemas
Laxative Suppositories
EXAM 1
is usually on Theory Day 6.
It covers the first 5 days of
theory content.
General Exam Information
1. Provide your own exam scantron form for each exam. Scantron form must be smooth, clean, and
without marks. May be purchased at ARC bookstore.
2. Have two sharp #2 pencils ready and a good eraser that will not leave any marks on the scantron.
3. Exam correction is via scantron mechanical correction device. Extra marks, tears, or folds detected
by the machine may be calculated as a wrong answer. The answer will thus remain wrong.
4. Cheating is inexcusable. A student who cheats will be dropped from the class and issued an "F"
grade in the class. As a violation of "Students Standards of Conduct", such action may be reported
to the ARC Disciplinary Officer.
PRE-CLASS ASSIGNMENT #2
View the skills CD that comes with the textbook:
Students will be introduced to the care giving skills in theory. However, the nurse assistant class is a fast
moving class. Therefore, it is required that students watch the skills CD before the class begins. By week
three, students will move to the campus skill lab to practice on other students. All students must reach a
competent level of practice in the skill lab before progressing to the long term care facility to gain
experience providing care to residents. Lab practice is mandatory. No student can progress to the clinical
facility who has not adequately demonstrated skill competence in the campus lab.
-15-
PRE-CLASS ASSIGNMENT #3
NURSE 100
Medical Abbreviation List
Instructions: Memorize the following abbreviations.
HOB head of bed NGT nasogastric tube NCP nursing care plan
FOB foot of bed GT gastrostomy tube wc wheel chair
OOB out of bed IV intravenous ROM range of motion
BRP bathroom privileges H
2
O water H/A headache
Amb ambulate O
2
oxygen c/o complains of
BR bed rest Q every wt weight
CPR cardiopulmonary resuscitation QD every day ht height
DNR do not resuscitate QOD every other day R right
AM morning Q2hr every 2 hours L left
PM evening or night BID 2 times in a day Ua urine
HS hour of sleep or bed time TID 3 times in a day BM bowel movement
I&O intake and output QID 4 times in a day SOB short of breath
tsp teaspoon hr. hour Stat immediately
Tbsp tablespoon min. minute PRN as needed
ml milliliter sec. second DC discontinue
L liter c with PPE
personal protective
equipment
liq liquid s without change
NPO nothing by mouth CMS
circulation, movement,
sensation
VS Vital Signs
PO by mouth PT physical therapy T
Temperature
O oral
Ax axilliary
R rectal
MD medical doctor OT occupational therapy RP Radial Pulse
RN registered nurse RT respiratory therapy AP Apical Pulse
LVN licensed vocational nurse DHHS
Department of Health &
Human Services
R Respiratory
CNA certified nurse assistant OBRA
Omnibus Budget
Reconciliation Act:
Federal Law
B/P Blood Pressure
increase or upper Dx. diagnosis HOH hard of hearing
decrease or lower Tx. treatment ADL activities of daily living
-16-
PRE-CLASS ASSIGNMENT #4
Memorize the following vital signs (VS) exactly as written:
There will be a VS memorization test on day three (3) of the class. There is no credit for partial memorization.
Students must correctly write the entire VS information to pass the test.
No student can go to the clinical facility who has not memorized the following VS. Memorize one section at a
time. Test yourself on a separate sheet of paper until you can remember all the VS. Students need only
memorize the VS information. Theory and VS practice will be done in class.
VITAL SIGNS
Temperature (T)
Normal Ranges
(F = Degrees Fahrenheit)
Duration of Insertion of Glass
Thermometer
Axillary (ax) 96.6 F - 98.6 F 5 - 10 min
Oral (o) 97.6 F - 99.6 F 3 min
Rectal (r) 98.6 F - 100.6 F > 3 min (> = Greater than)
Radial Pulse (RP)
60 - 80 beats / min (b/m)
normal characteristics: regular rhythm, strong beats
Apical pulse (AP)
60 - 80 beats / min (b/m)
normal characteristics: regular rhythm, strong beats
Respirations (R)
16 - 20 breaths / min (br/m)
normal characteristics: quiet, unlabored, even rise and fall of the chest
Blood Pressure (BP)
90 140 mmHG Systolic Pressure Blood Pumping Phase
60 90 mmHG Diastolic Pressure Blood Flowing Phase
-17-
COMMITMENT FOR SUCCESS
To be successful in the nurse assistant class the student must be able to read, write, listen, understand, and appropriately
respond in English at a minimum 6
th
grade level. A students actions must also appropriately reflect English comprehension.
Without this English skill you should not enter the class. Without this English skill you will not be successful in the class.
To be successful in the nurse assistant class the student must also make a commitment to the time needed to read the textbook,
view the skills CD, apply interactive handouts, write the information required on the study guides and study for exams and skill
labs.
Reading
Textbook, course handouts, study guides, clinical handouts and documentation forms
Four (4) multiple choice tests and one (1) medical abbreviation fill-in test
List of skills tested in California
Writing
Class notes
Clinical documentation
Interactive class handouts
Medical abbreviation fill-in test
Exam study guides
Listening - Understanding - Verbalizing
Listen to lecture and clinical instructions
Listen to needs, concerns, desires of residents
Seek assistance and ask question when unsure
Give verbal responses that reflect understanding of the English language
Behavior and Actions
Maintain a positive learning attitude
Be friendly and cooperative
Demonstrate and maintain self-correcting behavior
Actively seek new learning experiences in clinical
Demonstrate appropriate actions when given verbal or written information
Time in Class (Estimated time you will spend in class)
Theory Class: 12-16 hours per week in theory class. See current class schedule in this packet.
Clinical Experience: 7 hours each. See current class schedule in this packet.
Adhere to the late/absent policy: Read and understand the class late/absent policy found in the course syllabus in this
packet.
Homework, Study and Study Groups
Time estimates are for students with English as a first language. If you are a student with English as a second
language you may well need to spend greater than these hours.
Reading Assignments: 6-8 hours per week
Pre-exam Study Guide: 6-12 hours each (there are 4). A pre-exam study guide is typically given to students the weekend
prior to each exam.
Campus Skill Labs: 2-4 hours skills study prior to each lab and memorization of the skills listed for the California CNA test.
Small Group Study: There will be time in class to meet and develop study groups. A small study group is strongly advised and
greatly enhances success.
R.A.D (Reading Across the Disciplines): A 9-week lecture class to assist the student to best utilize study methods that
personally help improve classroom performance. Approx. hour per week for .5 unit of college credit.
-18-
ARC STUDENT ACCESS CARD
What is a Student Access Card? It is your:
Official College Photo ID Card
College Library Card
GoPrint Card
Regional Transit Pass Card
NURSE 100 Official Clinical Name Tag
(Your clinical name tag/Student Access Card is MANDATORY)
How will the Student Access Card be displayed during clinical?
Your Student Access Card must be worn with your clinical uniform for every clinical lab. A uniform access card
holder will be provided by your instructor.
When can a student obtain a current semester Student Access Card?
Students can get their Student Access Card beginning August 1 for the Fall semester and January 3 for the Spring
semester.
What does a Student Access Card cost?
There is no extra charge other than your class tuition. The fee is waived for students receiving BOG fee waivers;
students enrolled in the Criminal Justice Training Consortium; students enrolled in Apprenticeship programs; and
those UC Davis students taking classes on the UC Davis main campus. There is a replacement fee of $15.00 for lost
or damaged cards.
Where can a student pick up their Student Access Card?
There are three Access Card stations available to American River College students:
Information Services (Administration Building)
Monday Thursday: 8:00 am 6:30 pm
Friday: 8:00 am 4:30 pm
Portable Village, Room 605 (South of Davies Hall, near Campus Police)
Monday Thursday: 10:00 am 6:45 pm
Friday: 10:00 am 2:45 pm
Saturday: 9:00 am 2:45 pm
Natomas Education Center (2421 Del Paso Rd.)
Monday Thursday: 10:00 am 6:00 pm
Friday: 10:00 am 4:00 pm
What documentation must a student bring to pick up their Student Access Card?
To get the card, students must bring a photo ID and proof of course payment for the current semester (this can be
printed from eServices or obtained from the college Business Office) or a copy of their BOG fee waiver and proof of
enrollment.
For your card to be valid, it must have the current semester sticker attached.
-19-
INFORMATION COLLECTION AND ACCESS: PRIVACY STATEMENT
SUPPLYING YOUR SOCIAL SECURITY NUMBER TO
DEPARTMENT OF HEALTH SERVICES
ASocial Security Number Disclosure: Pursuant to Section 666 (a) (13) of Title 42 of the United States Code and
California Family Code, Section 17520, subdivision (d), the California Department of Public Health (CDPH) is
required to collect Social Security numbers from all applicants for nursing assistant certificates, home health aide
certificates, hematolysis technicians certificates or nursing home administrator licenses. Disclosure of your social
security number is mandatory for purposes of establishing, modifying, or enforcing child support orders upon
request by the Health Integrity and Protection Data Bank as required by 45 CFR subsection '61.1 et seq. Failure
to provide your social security number will result in the return of your application. Your social security number will
be used by CDPH for internal identification, and may be used to verify information on your application, to verify
certification with another state=s certification authority, for exam identification, for identification purposes in
national disciplinary databases or as the basis of disciplinary action against you.@
The above statement is available on the California Department of Public Health website www.cdph.ca.gov
Student Copy
-20-
Disqualifying Penal Code Sections
If they have been convicted of any of the penal codes listed, CNAlHHA
applicants will be automatically denied certification or ICF/DD, DDH, or DDN
applicants will be denied employment.
All CNA/HHA applicants should review this list carefully to avoid wasting
their time, effort and money by training, testing and submission of
fingerprints since they cannot receive the required criminal background
clearance if they have been convicted of any of these violations.
Section
187
192(a)
203
205
206
207
209
210
210.5
211
220
222
243.4
245
261
262
264.1
265
266
266a
266b
266c
266d
266e
266f
266g
266h
266i
266j
266k
267
273a
273d
Murder
Manslaughter, Voluntary
Mayhem
Aggravated Mayhem
Torture
Kidnapping
Kidnapping for ransom, reward, or extortion or robbery
Extortion by posing as kidnapper
False imprisonment
Robbery (Includes degrees in 212.5 (a) and (b
Assault with intent to commit mayhem, rape, sodomy, oral copulation
Administering stupefying drugs to assist in commission of a felony
Sexual battery (Includes degrees (a) - (d
Assault with deadly weapon, all inclusive
Rape (Includes degrees (a)-(c
Rape of spouse (Includes degrees (a)-(e
Rape or penetration of genital or anal openings by foreign object
Abduction for marriage or defilement
Inveiglement or enticement of female under 18
Taking person without will or by misrepresentation for prostitution
Taking person by force
Sexual act by fear
Receiving money to place person in cohabitation
Placing a person for prostitution against will
Selling a person
Prostitution of wife by force
Pimping
Pandering
Placing child under 16 for lewd act
Felony enhancement for pimping/pandering
Abduction of person under 18 for purposes of prostitution
Willful harm or injury to a child; (Includes degrees (a)-(c
Corporal punishment/injury to a child (Includes degrees (a)-(c
-21-
Section
273.5
285
286(c)
(d)
(f)
(g)
288
288a(c)
(d)
(f)
(g)
288.5
289
289.5
368
451
459
470
475
484
484b
484d-j
487
488
496
503
518
666
Willful infliction of corporal injury (Includes (a)-(h
Incest
Sodomy with person under 14 years against will
Voluntarily acting in concert with or aiding and abetting in act of sodomy
against will
Sodomy with unconscious victim
Sodomy with victim with mental disorder or developmental or physical disability
Lewd or lascivious acts with child under age of 14
Oral copulation with person under 14 years against will
Voluntarily acting in concert with or aiding and abetting
Oral copulation with unconscious victim
Oral copulation with victim with mental disorder or developmental or physical
disability
Continuous sexual abuse of a child (Includes degree (a
Penetration of genital or anal openings by foreign object (Includes degrees (a)-
u
Rape and sodomy (Includes degrees (a) and (b)
Elder or dependent adultabuse;theft or embezzlement of property (Includes (b)-
(f
Arson (Includes degrees (a)-(e
Burglary (Includes degrees in 460 (a) and (b
Forgery (Includes (a)-(e
Possession or receipt of forged bills, notes, trading stamps, lottery tickets or
shares (Includes degrees (a) - (c
Theft
Intent to commit theft by fraud
Theft of access card, forgery of access card, unlawful use of access card
Grand theft (Includes degrees (a)-(d
Petty theft
Receiving stolen property (Includes (a)-(c
Embezzlement
Extortion
Repeat convictions for petty theft, grand theft, burglary, carjacking, robbery and
receipt of stolen property
Certification of applicants with convictions on this list MAY be reconsidered by ATCS
only if misdemeanor actions have been dismissed by a court of law or a Certificate of
Rehabilitation has been obtained for felony convictions. Any other convictions, other
than minor traffic violations, must also be reviewed by ATCS.
ATCS 98-4 (4/02)
-22-
Note: Certificate(s) of rehabilitation must be submitted with NURSE 100
course prerequisites.
LIVE SCAN FINGERPRINTS
All students in NURSE 100 Nurse Assistant class will be fingerprinted via a live scan process. Live Scan
technology allows digitally scanned fingerprints and related information to be submitted electronically to the
Department of Justice. Please read through the disqualifying penal codes. If you have a conviction of any code
listed, you cannot be in the Nurse Assistant class. If a student has had a conviction in the past of any code listed,
he/she cannot be in the Nurse Assistant class unless a letter of clearance or letter of rehabilitation from the courts
is submitted with the course prerequisites.
Students will pay $10.00 for the convenience of having the print company come to the classroom to do all student
prints at the same time. The instructor will arrange for the printing company to come during class time.
The Department of Justice (DOJ) process fee of $43.00 is NOT paid by the student. The clinical facility will pick up
the student fee for DOJ live scan print processing. Students must have a picture ID to show at the time of printing.
Please have a CA Driver=s License or CA Identification Card ready to present.
-23-
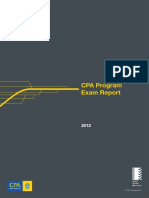
Stadium
Parking
Room Building
CDC 100s ................. Child Dev. Ctr. (west)
CDC 300s ..................Child Dev. Ctr. (east)
D100-D401 ...............................Davies Hall
ER 1-3 ................Environmental Resources
H100-H171 .............................Howard Hall
120-129 .............. Liberal Arts (CS&IT, Bus)
130-139 ............ Liberal Arts (CS&IT, Math)
150-159 .............. Liberal Arts (CS&IT, Bus)
160-162 ........................................ Raef Hall
163-170 ............Liberal Arts (Mathematics)
200-289 .......................KA (PE) & Athletics
300-399 ......................................... Tech Ed
400-499 ..........................................Science
500s ............................ Fine & Applied Arts
600s ................................. Portable Village
700-702 ........... Health & Education (north)
710-771 ........... Health & Education (south)
Service Building
Admissions &
Records ...... Administration
Assessment .... Student Services
Business
Services ...... Administration
Counseling ..... Administration
Disabled
Services .... Student Services
Financial
Aid ............ Student Services
Health
Center ......... Administration
Oak Caf .....Fine & Applied Arts
Police..... south of Davies Hall
Oces not on map
Oce Building
Behav/Soc. Sci. ........... Davies Hall, 3
rd
oor
Bus. & Comp. Science ....... Liberal Arts 133
English ....................... Davies Hall, 3
rd
oor
Health & Education ........ Health & Ed-South
Humanities ................. Davies Hall, 3
rd
oor
Mathematics ........................... Howard Hall
Planning, Research, Technology
& Professional Development ..................ITC
Portable Village Key (600s)
Temporary Cafeteria ............602-603 & 610
e-Services/Journey .....................................605
Student Development Ofce ................. 608
Campus Life Center ......................... 611-612
The Spot.................................................613
ENTERHERE
ENTERHERE
ENTERHERE
P = Daily parking permit machine
T = Public telephones
E = Emergency telephones
D = Paratransit loading zone
= Bike rack and/or locker
= Construction zone
= Automated external debrillator
DAVIES HALL
130s
SCIENCE
TECHED
RAEF HALL
160-162
163-170
RANCH
HOUSE
KINESIOLOGY&
ATHLETICS
BOOKSTORE
GYM
200s
HEALTH&
EDUCATIONSOUTH
710-771
COUNSELING
ADMINISTRATION
120s
AMERICAN RIVER COLLEGE
4700 College Oak Drive, Sacramento, CA 95841
SPRING 2012
BUSINESS
150s
ROSE
MARKS
QUAD
LIBRARY
RECEIVING
CDCWEST
100s
CDCEAST
300s
ENVIRONMENTAL
RESOURCES
ER 1-3
400s
ITC
DSP&S
D100-D401
COLLEGE
POLICE
HOWARDHALL
LIBERAL ARTS
HEALTH&
EDUCATIONNorth
700, 701, 702
300s
C
o
n
s
t
r
u
c
t
i
o
n
Z
o
n
e
(
R
e
l
o
c
a
t
e
d
t
o
6
0
0
s
)
MAPREVISED: JANUARY6, 2012
LEARNING
RESOURCE
CENTER
FINE &
APPLIEDARTS
500s
FINE &
APPLIEDARTS
OFFICES
PORTABLE
VILLAGE
600s
A
R
C
A
D
E
C
R
E
E
K
SCIENCE
OFFICES
Oak
Caf
Theatre
Box
Ofce
eServices
Center
Temporary
Cafeteria
Coffee
Kiosk
602-603
605
614
600
601
6
0
9
-6
1
3
6
0
6
-6
0
8
STUDENT
SERVICES
S
t
a
f
f
P
a
r
k
i
n
g
Staff Parking
Construction
Zone
(Tennis courts)
Construction
Zone
(Parking Garage)
HEED NORTH
700, 701, 702
Funeral Service/ECE/
Nutrition/SLPA
HEED SOUTH
710 - 771
Nursing Dept 731
- Business Office
- Enrollment Srvcs
- Health Center
- Counseling
Assessment
Center
R
T
L
ig
h
t R
a
il
Madison Avenue
G
a
r
e
l
d
A
v
e
n
u
e
Myrtle Avenue
Auburn Blvd.
Exit Winding Way
O
ran
g
e
G
rove
C
o
l
l
e
g
e
O
a
k
D
r
i
v
e
W
a
t
t
A
v
e
n
u
e
E
d
i
s
o
n
A
v
e
n
u
e
W
a
l
n
u
t
A
v
e
n
u
e
A
u
b
u
rn
B
lv
d
C
a
p
C
it
y
F
r
e
e
w
a
y
to
D
o
w
n
to
w
n
to SF, I-5
& Airport
to Reno
AMERICAN RIVER COLLEGE
4700 College Oak Drive | Sacramento, CA 95841
For more information
(916) 484-8011
www.arc.losrios.edu
Los Rios Community College District
Parking Information
Visitor Parking
A visitor parking area with parking meters is
located by the Administration Building on College
Oak Drive. The cost is 25 per 15 minutes. (No
student parking is permitted in the visitors area.)
Visitor permits are available from the Information
Center in the Administration Building.
Parking Permits &
Daily Tickets
All vehicles on campus 7:00 a.m.11:00 p.m. must
display a permit or daily parking permit. Permits
are not required during non-school days and
weekends. For your protection, all vehicles should
be locked and all valuables stored out of sight.
uail, a||ia, |ic|:|s a|: :! aa1 a|: 1is:as:1
from machines located in each parking lot.
In case of machine malfunction, you may: 1)
Purchase a ticket from another machine; 2)
Contact a college police ofcer for a one-day
permit. Notes about machine malfunction will
not be accepted.
::a:s|:| :|ai|s. \ a||ia, :|ai| is
:, :| s :a:s | :| :! | e| s uaa:|
session. A permit entitles the student to day
or evening college parking, and is available
from the Business Services Ofce located in
the Administration Building. Remember that
a parking permit does not guarantee a parking
space. A parking permit entitles you to park on
campus where and when space is available.
Handicapped
Parking
Automobiles of students with disabilities (and
persons providing transportation services to stu-
dents with disabilities) must display a semester or
daily parking permit as do other students. However,
special parking spaces for disabled students are
provided in all student parking lots. A placard
issued by the Department of Motor Vehicles for per-
sons with disabilities, or a distinguishing license
plate for persons with disabilities, must be properly
displayed on the vehicle. Temporary disability
permits are available from the Health Center; if
you are issued a temporary permit you must also
display a valid semester or daily parking permit.
Motorcycles
Me|e|c,cl: :|ai|s a|: :! :| s:a:s|:|.
Motorcycles may only park in designated
motorcycle areas. Motorcycles may not park in
regular student spaces.
Tow-Away
Vehicles parked illegally in red zones and vehicles
parked so as to impede the flow of traffic on
campus streets, lot entrances and driveways, in
front of re hydrants or in other areas where
emergency vehicles might be hindered, may be
subject to being towed away at owners expense
and inconvenience. Vehicles parked in staff or
handicapped spaces are subject to tow-away.
Driving to Campus
If you need directions or have any
questions, feel free to contact us at
(916) 484-8011 or check our
website: www.arc.losrios.edu
Parking Citations
Permits are not required during non-school
hours. A list of common violations is shown below,
although other regulations are also enforced
[0\0 !!!!,].
Nature of Oense Code Bail
Ne ali1 :|ai| isi|l: ,\.! :,,.
l|au1ul:a| us: e| :|ai| ,\.+ :ee.
0u|1a|:1 :|ai| ,\.\ :,,.
l:|ai| ia|e:|l, 1isla,:1 ,\.e :,,.
la||:1 e:| |eua1a|, lia:s +\.! :,,.
ls:1 |e a||ia, sac:s +\.! :,,.
la||:1 ia 1|iia, laa:s +\., :,,.
\e| a||:1 ia 1:si,aa|:1 a|:a +b :,,.
laau||. us: e| |:s:|:1 leca|iea +0 :,,.
laau||. us: e| 1isa|l:1 .ea: +u.! :!,.
laau||. us: e| :|ai| +u.! :,,.
la||:1 ea s:|ic: |ea1 +u., :,,.
la||:1 ia |:1 .ea: +u.+ :,,.
la||:1 |lec|ia, ,a|:s +u. :,,.
la||:1 ia |us .ea: +u.e :,,.
la||:1 ia ae a||ia, .ea: +u. :,,.
la||:1 ia lea1ia, .ea: +u. :,,.
lxi|:1 a:|:|/.ea: +u.! :,,.
la||:1 ea s|eul1:| e| |ea1 +u.!! :,,.
la||:1 ia h|: laa: +u.!! :,,.
la||:1 ea |ea1a, +u.!, :,,.
\:|icl: a||:1 e:|ai,|| +l :,,.
College Police
The College Police ofce is located south of Davies
Hall (see reverse side).
s Ofce Hours
Mon-Fri, 8:00 am-5:00 pm
s 24-Hour Phone
(916) 558-2221
NURSE 100 - NURSE ASSISTANT
MEDICAL PACKET
Print out the following ARC Medical Forms
(4 Pages):
A. Health Clearance Checklist
B. Health History
C. Physical Exam
-26-
Health_Clearchk_NA (Revised 10/12/10)
AMERICAN RIVER COLLEGE
HEALTH CLEARANCE CHECKLIST
NURSE ASSISTANT PROGRAM
Upper Section To Be Completed by Student
Name Student ID No.
SEMESTER/YEAR: Fall
Spring
Medical Clearance Section To Be Completed by Program Nursing Instructor or Nursing Director
I. PHYSICAL EXAMINATION CLEARANCE
A. Health Care Provider's Signature and Stamp
AND
B. Physical Exam
$ Date physical exam completed ________________________
$ Obtained within one (1) year prior to program registration
$ Health care provider must check () #1. Can participate with no restrictions.
II. HEALTH HISTORY CLEARANCE
A. Completed by Student, With Student's Signature and Date
B. Health Care Provider's Signature and Stamp
III. TUBERCULOSIS CLEARANCE
A. PPD
$ Date Read_________________________
$ Obtained within last six (6) months prior to program registration
$ Copy of report form signed by medical staff who gave PPD injection. Skin results
documented as negative
OR
B. X-ray
$ Date Read_________________________
$ Obtained within last one (1) year prior to program registration
$ Chest X-ray results state: Negative CxR or no evidence of active (TB) disease
Nursing Instructor or Nursing Director will sign and date clearance.
DATE CLEARED BY
AMERICAN RIVER COLLEGE
Nurse Assistant Program
HEALTH HISTORY
The information on the health history form must be completed in its entirety and signed by the student. The
health care provider must also review and sign this form at the time of student's physical examination.
Student: All sections must be completed - upper section, questions, & signature.
Name LRCCD Student ID No.
Last First Middle
Health Care Provider
Health Care Providers Address
City, State, Zip
Health Care Providers Telephone Number
YES NO The following questions are to be answered by checking either "Yes" or "No".
Have you been under a doctor's care in the last 12 months?
Have you been in the hospital in the last 12 months?
Have you ever had any type of surgery?
Do you want to talk to a doctor about a health problem or any injury?
Have you ever been restricted from any activity or employment because of a health problem or injury?
Has anyone in your immediate family ever had:
Diabetes (high sugar in blood)?
Allergies (hay fever or asthma)?
Migraine headaches?
Heart trouble?
High blood pressure?
Has anyone in your family died suddenly?
Have you had or do you now have:
Brain concussion (head injury)?
Tendency to lose consciousness (faint)?
Skull fracture?
Convulsions or epilepsy?
Neck injury?
Impaired (poor) vision in one or both eyes?
Temporary loss of vision?
To wear glasses or contact lenses?
Hearing loss?
Perforated eardrum?
Discharge from ear(s) (recurrent infections)?
Sinus infections?
Broken nose?
Dental Plate (dentures)?
Orthodontia (teeth straightened)?
Have you had or do you now have?
Hernia?
Kidney problems?
Loss of function or absence of testicles (Men)?
Menstrual problems (Women)?
(OVER)
YES NO The following questions are to be answered by checking either "Yes" or "No".
Have you had or do you now have?
Bone fracture?
Joint dislocation?
Foot problems?
To wear a cast?
Back injury or frequent backaches
Knee injury (sprain) or recurrent pain?
Ankle injury (sprain) or recurrent pain?
Other joint problems, e.g., swelling pain, decreased range of motion?
Bone infection?
Have you had or do you now have?
Weight problem (under or overweight)?
Diabetes (high sugar in blood or urine)?
Tendency to bleed or bruise easily?
Anemia ("tired" blood)?
Heart trouble or murmur?
High blood pressure?
Persistent cough?
Chest pain with exercise?
Dizziness or faintness with exercise?
Asthma (wheezing)?
Hay Fever?
Hives or rash?
Bee sting reactions (allergy)?
Reaction to medicine (allergy)?
Have you had or do you now have?
Recurrent rash?
Fungus?
Athlete's foot?
Recurrent boils (skin infection)?
Do you....................
Smoke?
Take any medicine regularly?
If "yes", name of medication
Take medicine for emergency use?
If "yes", name of medication
If you answered "yes" to any question, please explain below.
I VERIFY THAT THE RESPONSES ON THIS QUESTIONNAIRE ARE CORRECT TO THE BEST OF MY KNOWLEDGE.
Student's Signature Date
HEALTH HISTORY REVIEWED BY:
Health Care Providers Signature Date
Verify Signature with
(Revised 08/24/10) Health Care Provider's Stamp
AMERICAN RIVER COLLEGE
PHYSICAL EXAM
NURSE ASSISTANT PROGRAM
Upper Section to Be Completed by Student Student ID Number
Last Name First Name MI
Address Phone
City & State Zip
Birth Date Age Sex Height Weight
To Be Completed by Health Care Provider
Blood Pressure Pulse Rate
Significant Medical History
Current Complaints of Disabilities Pertinent to Student=s Participation
EXAMINATION (SYSTEM REVIEW)
NORMAL
ABNORMAL
COMMENTS
1. General Appearance
2. Eyes
3. Ears, Nose & Throat
4. Mouth & teeth
5. Neck
6. Lymph Nodes
7. Respiratory
8. Cardiovascular
9. Abdomen
10 Genitalia-Hernia
11. Skin
12. Neuro
13. Musculoskeletal
Recommendations Regarding Participation in the Nurse Assistant Program
1. Can participate with no restrictions*
2. No participation until: *
3. No participation
*The health care provider verifies that the individual does not have any health condition that would create a hazard for himself/herself,
fellow employees, patients, and visitors.
NOTE: NO ACCOMMODATIONS ARE AVAILABLE FOR LIMITED, RESTRICTED, AND/OR PARTIAL PARTICIPATION.
Health Care Provider's Name: Please Review and Sign "Health History" Completed by Student
Verify Signature with
Health Care Provider's Signature Date Health Care Providers Stamp
Health Care Provider (Print) Telephone Number
Address, City, State, Zip (Print)
I hereby authorize release of pertinent medical records to American River College.
Students Signature Date
You might also like
- REPRODUCTIVE ENDOCRINOLOGY/INFERTILITY NURSING: Passbooks Study GuideFrom EverandREPRODUCTIVE ENDOCRINOLOGY/INFERTILITY NURSING: Passbooks Study GuideNo ratings yet
- Principles of Health Science SyllabusDocument6 pagesPrinciples of Health Science Syllabusapi-237835375No ratings yet
- Medical Microbiology SyllabusDocument7 pagesMedical Microbiology Syllabusapi-237835375No ratings yet
- Chapter 2Document14 pagesChapter 2Neil YoungNo ratings yet
- NUR 105 Basic Nursing Assistant Handbook 2013 2014Document48 pagesNUR 105 Basic Nursing Assistant Handbook 2013 2014Ronald AranhaNo ratings yet
- Health Science Technology Course Syllabus Rivera Early College High SchoolDocument5 pagesHealth Science Technology Course Syllabus Rivera Early College High Schoolapi-360457634No ratings yet
- NURS 3414: Health Assessment Course Syllabus: BSN Program Fall 2017Document16 pagesNURS 3414: Health Assessment Course Syllabus: BSN Program Fall 2017Trisha MarieNo ratings yet
- FNP Survival Kit (1) 700Document61 pagesFNP Survival Kit (1) 700api-285177380No ratings yet
- JH - Health Science 2021-22 Syllabus 3Document7 pagesJH - Health Science 2021-22 Syllabus 3api-521590840No ratings yet
- Syllabus Syllabus Syllabus: Last Revised: 8/1/2020 7:04 A8/p8Document22 pagesSyllabus Syllabus Syllabus: Last Revised: 8/1/2020 7:04 A8/p8KweenPin AsiaNo ratings yet
- AGEROSite Visitor Handbook 2020Document30 pagesAGEROSite Visitor Handbook 2020Borislav VulićNo ratings yet
- ClinicalSurvivalGuide 2012 2013Document62 pagesClinicalSurvivalGuide 2012 2013Zebram Zee100% (1)
- Stage 3 Handbook 2012Document21 pagesStage 3 Handbook 2012Nikhil KumarNo ratings yet
- Sydney Handbook Nursing PDFDocument41 pagesSydney Handbook Nursing PDFMarin AndreiNo ratings yet
- NUR 450 Medical Surgical Nursing II SyllabusDocument23 pagesNUR 450 Medical Surgical Nursing II SyllabusMohammad Malik0% (2)
- FNP Survival Kit FinalDocument60 pagesFNP Survival Kit Finalapi-28517154450% (2)
- Health Sciences Education Guide: As An International Organisation, IBLCE Uses British English in Its PublicationsDocument11 pagesHealth Sciences Education Guide: As An International Organisation, IBLCE Uses British English in Its PublicationsCatalina LucaNo ratings yet
- Essentials Nutrition: Instructor & Class InformationDocument5 pagesEssentials Nutrition: Instructor & Class InformationtherealbettyNo ratings yet
- Economic Botany - Biology 350.001: Spring Semester, 2011Document5 pagesEconomic Botany - Biology 350.001: Spring Semester, 2011KoyaaaMarkNo ratings yet
- NUR1022LDocument10 pagesNUR1022LyousefkhalifaNo ratings yet
- Medterm1415 SyllabusDocument4 pagesMedterm1415 Syllabusapi-292047514No ratings yet
- Course Outline For HLTH 301, University of CanterburyDocument8 pagesCourse Outline For HLTH 301, University of CanterburyArin BasuNo ratings yet
- Medical Terminology Course Syllabus Rivera Early College High SchoolDocument5 pagesMedical Terminology Course Syllabus Rivera Early College High Schoolapi-360457634No ratings yet
- Ans3421 - ActivityDocument11 pagesAns3421 - ActivityWynnie RondonNo ratings yet
- BIO 239 Summer 2016 SyllabusDocument4 pagesBIO 239 Summer 2016 SyllabuslovebearrawrNo ratings yet
- School of Medicine DIET451: Dietetics 2: Subject OutlineDocument15 pagesSchool of Medicine DIET451: Dietetics 2: Subject OutlineSarilXNo ratings yet
- Cosmetology SyllabusDocument4 pagesCosmetology Syllabusapi-419468711No ratings yet
- Culinary Arts Institute Clnart 101 - Culinary Fundamentals I Syllabus - Fall 2016Document10 pagesCulinary Arts Institute Clnart 101 - Culinary Fundamentals I Syllabus - Fall 2016gwendonNo ratings yet
- Terria Moore R.N. & Courtney Taylor R.N. Course Syllabus: Bryant Career Technical CenterDocument6 pagesTerria Moore R.N. & Courtney Taylor R.N. Course Syllabus: Bryant Career Technical CenterchhatraNo ratings yet
- Family PhysicianDocument4 pagesFamily Physicianapi-332070699No ratings yet
- Syllabus N2209 201530Document17 pagesSyllabus N2209 201530manjitNo ratings yet
- Phlebotomy CourseworkDocument5 pagesPhlebotomy Courseworkf5ddpge2100% (2)
- Child Life Internship Application 012016Document9 pagesChild Life Internship Application 012016Chelsea ChanceNo ratings yet
- Desktop n112 SyllabusDocument10 pagesDesktop n112 SyllabusRosemaryCastroNo ratings yet
- Biotech12syllabus PublicDocument3 pagesBiotech12syllabus Publicapi-353019866No ratings yet
- Rads 1010 Fall 2015Document7 pagesRads 1010 Fall 2015api-295740145No ratings yet
- Bio 103 SyllabusDocument10 pagesBio 103 Syllabuscsmith19No ratings yet
- NEW UMHS Clinical Student HandbookDocument25 pagesNEW UMHS Clinical Student HandbookAmit TamboliNo ratings yet
- CHC50113 Diploma of Early Childhood Education and CareDocument14 pagesCHC50113 Diploma of Early Childhood Education and CareSandeep KaurNo ratings yet
- 2020 2021 MECO 0070 Medical Coding Medical CodingDocument8 pages2020 2021 MECO 0070 Medical Coding Medical CodingLibi FarrellNo ratings yet
- Emergency MedicineDocument11 pagesEmergency MedicineJai SinghNo ratings yet
- Principles of Animal Science SyllabusDocument7 pagesPrinciples of Animal Science SyllabusFiorello AbenesNo ratings yet
- Centennial LetterDocument10 pagesCentennial Letter1oneiricNo ratings yet
- Biotech Syllabus Aug2015Document5 pagesBiotech Syllabus Aug2015api-275510930No ratings yet
- Developpement Humain Et Ntic-2: Initiation A La Langue AnglaiseDocument98 pagesDeveloppement Humain Et Ntic-2: Initiation A La Langue AnglaiseaminaNo ratings yet
- National College of Natural Medicine: Nscarlett@ncnm - Edu Kwindstar@ncnm - Edu Dkruschwitz@ncnm - EduDocument3 pagesNational College of Natural Medicine: Nscarlett@ncnm - Edu Kwindstar@ncnm - Edu Dkruschwitz@ncnm - EduAlexis FernandezNo ratings yet
- Eval 3Document7 pagesEval 3api-281109214No ratings yet
- Possible Questions For Oral DefesenseDocument5 pagesPossible Questions For Oral DefesenseAlexis Joy LimotNo ratings yet
- Weaver - Daniel 3339032001spring2020Document7 pagesWeaver - Daniel 3339032001spring2020jNo ratings yet
- Continuing Education ScheduleDocument40 pagesContinuing Education ScheduleAnonymous 7R6n0f9BYNo ratings yet
- 700 FNP Revised Survival Kit FinalDocument46 pages700 FNP Revised Survival Kit Finalapi-28529050467% (3)
- Paediatrics Child Health Application Handbook 2019 20 PDFDocument13 pagesPaediatrics Child Health Application Handbook 2019 20 PDFfunmilayo alagbeNo ratings yet
- Perio Clinic ManualDocument48 pagesPerio Clinic ManualPetia TerzievaNo ratings yet
- Culiinwcta2015 2016courseexpectationsculiiDocument8 pagesCuliinwcta2015 2016courseexpectationsculiiapi-295343976No ratings yet
- FMed Clerkship Handbook 2022-2023Document17 pagesFMed Clerkship Handbook 2022-2023jhhjjhNo ratings yet
- Chicago Review Press NCLEX-PN Practice Test and ReviewFrom EverandChicago Review Press NCLEX-PN Practice Test and ReviewRating: 4 out of 5 stars4/5 (4)
- Family Nurse Practitioner Certification Prep Plus: Proven Strategies + Content Review + Online PracticeFrom EverandFamily Nurse Practitioner Certification Prep Plus: Proven Strategies + Content Review + Online PracticeRating: 5 out of 5 stars5/5 (2)
- Essentials of Nursing Care: Chronicity: Passbooks Study GuideFrom EverandEssentials of Nursing Care: Chronicity: Passbooks Study GuideNo ratings yet
- The Chicago Review Press NCLEX-RN Practice Test and ReviewFrom EverandThe Chicago Review Press NCLEX-RN Practice Test and ReviewRating: 4 out of 5 stars4/5 (20)
- Annual Exam ReportDocument24 pagesAnnual Exam ReportFoo Yean NeeNo ratings yet
- PracticalityDocument6 pagesPracticalityMumtahina SuptiNo ratings yet
- Letter For Not Continuing SemesterDocument2 pagesLetter For Not Continuing SemesterD.m. Salah Uddin PavelNo ratings yet
- ESIC Recruitment of STENOGRAPHER and UPPER DIVISION CLERK For Maharashtra PDFDocument19 pagesESIC Recruitment of STENOGRAPHER and UPPER DIVISION CLERK For Maharashtra PDFPritiNo ratings yet
- Business Communication PLO CLODocument3 pagesBusiness Communication PLO CLOSaadia KhanNo ratings yet
- MOR 465 SyllabusDocument8 pagesMOR 465 SyllabussocalsurfyNo ratings yet
- 10 Tips in Taking The Let ExamDocument14 pages10 Tips in Taking The Let ExamJom Maglente BeltranNo ratings yet
- GMC Application Form For IMGsDocument24 pagesGMC Application Form For IMGsNOMOREHATEOKNo ratings yet
- TOG Youth Employment ResearchDocument48 pagesTOG Youth Employment ResearchToplum Gönüllüleri VakfıNo ratings yet
- DISC 212-Introduction To Management Science-Muhammad Adeel ZaffarDocument4 pagesDISC 212-Introduction To Management Science-Muhammad Adeel Zaffar16110299No ratings yet
- Instrumentation and ControlDocument121 pagesInstrumentation and ControlabbutalibbNo ratings yet
- Joint Entrance Screening Test (JEST) - 2015: (To Be Filled On OMR Sheet)Document1 pageJoint Entrance Screening Test (JEST) - 2015: (To Be Filled On OMR Sheet)deependraNo ratings yet
- Numbas Practice Test PDFDocument34 pagesNumbas Practice Test PDFBavique PuspacenoNo ratings yet
- AMS UG Student GuideDocument48 pagesAMS UG Student GuideRishi SinghNo ratings yet
- Lifelong LearningDocument10 pagesLifelong Learningrezki eriyandoNo ratings yet
- Medicine IMM SyllabusDocument53 pagesMedicine IMM SyllabusAamir HamaadNo ratings yet
- Cae Speaking GuideDocument11 pagesCae Speaking Guideelisadp83% (6)
- Angels of Emergency - True Life Rescue Stories From Americas Paramedics and Emts PDFDocument601 pagesAngels of Emergency - True Life Rescue Stories From Americas Paramedics and Emts PDFComputerDrNo ratings yet
- Employment Guide PDFDocument109 pagesEmployment Guide PDFConnieAllanaMacapagaoNo ratings yet
- NursesDocument36 pagesNursesGilbert BagsicNo ratings yet
- Fs 1 Ep 13Document7 pagesFs 1 Ep 13Marvie AmitafNo ratings yet
- Importance of ExaminationsDocument2 pagesImportance of ExaminationsDhiya Ajanz75% (4)
- ESEM5134-Curriculum, Instruction and Assessment in EducationDocument2 pagesESEM5134-Curriculum, Instruction and Assessment in EducationSARIPAH ABDUL HAMIDNo ratings yet
- 5154 Articles SBR Exam Techniques For SuccessDocument8 pages5154 Articles SBR Exam Techniques For SuccessSmag SmagNo ratings yet
- CCGP Candidate HandbookDocument21 pagesCCGP Candidate HandbookrxdocNo ratings yet
- Examination System in Pakistan: Unit-7Document22 pagesExamination System in Pakistan: Unit-7Muhammad BilalNo ratings yet
- Leed Ap Homes HandbookDocument19 pagesLeed Ap Homes Handbookrangarajan1989No ratings yet
- Chapter 1 Basic Concepts in AssessmentDocument34 pagesChapter 1 Basic Concepts in AssessmentMarry DanielNo ratings yet
- IBSC-TP-C Candidate HandbookDocument15 pagesIBSC-TP-C Candidate HandbookJuan Manuel Tiscareño GarciaNo ratings yet
- Oliver TwistDocument23 pagesOliver TwistSNAMISONo ratings yet