You might also like
- Ability of Procalcitonin To Predict Bacterial MeningitisDocument20 pagesAbility of Procalcitonin To Predict Bacterial MeningitisGeorge WinchesterNo ratings yet
- PCT FeverDocument6 pagesPCT FeverAndi BintangNo ratings yet
- Emergencias-2012 24 5 348-356 EngDocument9 pagesEmergencias-2012 24 5 348-356 EngJarvis WheelerNo ratings yet
- Procalcitonin Levels Diagnose Systemic Infections in ED PatientsDocument7 pagesProcalcitonin Levels Diagnose Systemic Infections in ED PatientsAndi BintangNo ratings yet
- Serum Procalcitonin in Bacterial & Non-Bacterial Meningitis in ChildrenDocument5 pagesSerum Procalcitonin in Bacterial & Non-Bacterial Meningitis in ChildrenrayhantaswinNo ratings yet
- White Paper CPD Sepsis AJCP 2005Document5 pagesWhite Paper CPD Sepsis AJCP 2005jtmchughNo ratings yet
- The Use of Procalcitonin As A Marker of Sepsis in Children: Abst TDocument3 pagesThe Use of Procalcitonin As A Marker of Sepsis in Children: Abst TAsri RachmawatiNo ratings yet
- Diagnostic Value of CSF C-Reactive Protein in Meningitis: A Prospective StudyDocument4 pagesDiagnostic Value of CSF C-Reactive Protein in Meningitis: A Prospective StudyHabibur RahmanNo ratings yet
- 58 JMSCRDocument4 pages58 JMSCRhumayun kabirNo ratings yet
- Serum Procalcitonin Levels in Bacterial and Abacterial MeningitisDocument5 pagesSerum Procalcitonin Levels in Bacterial and Abacterial MeningitisSaul Gonzalez HernandezNo ratings yet
- 2165-Article Text-2597-1-10-20200105Document7 pages2165-Article Text-2597-1-10-20200105IKA 79No ratings yet
- Marcadores Sericos para Cole AgudaDocument6 pagesMarcadores Sericos para Cole Agudajessica MárquezNo ratings yet
- Xia 2016Document29 pagesXia 2016Dewi PrasetiaNo ratings yet
- Validity of CSF Tests for Diagnosing Tuberculous MeningitisDocument5 pagesValidity of CSF Tests for Diagnosing Tuberculous MeningitismelisaberlianNo ratings yet
- PCT 2006 Read For DiscussionDocument8 pagesPCT 2006 Read For DiscussionArnavjyoti DasNo ratings yet
- 2 - Adult Meningitis in A Setting of High HIV and TB Prevalence - Findings From 4961 Suspected Cases 2010 (Modelo para o Trabalho)Document6 pages2 - Adult Meningitis in A Setting of High HIV and TB Prevalence - Findings From 4961 Suspected Cases 2010 (Modelo para o Trabalho)SERGIO LOBATO FRANÇANo ratings yet
- Diagnostic Accuracy of Procalcitonin, Neutrophil-Lymphocyte Ratio, C-Reactive Protein, and Lactate in Suspected Bacterial SepsisDocument25 pagesDiagnostic Accuracy of Procalcitonin, Neutrophil-Lymphocyte Ratio, C-Reactive Protein, and Lactate in Suspected Bacterial SepsisMelissa Indah SariNo ratings yet
- Procalcitonin and C-Reactive Protein During Systemic Inflammatory Response Syndrome, Sepsis and Organ DysfunctionDocument9 pagesProcalcitonin and C-Reactive Protein During Systemic Inflammatory Response Syndrome, Sepsis and Organ DysfunctionAsri RachmawatiNo ratings yet
- Evaluation of PCV, Cd4 T Cell Counts, ESR and WBC Counts in Malaria Infected Symptomatic HIV (Stage 11) Male HIV/ Aids Subjects On Antiretroviral Therapy (Art) in Nnewi, South Eastern NigeriaDocument5 pagesEvaluation of PCV, Cd4 T Cell Counts, ESR and WBC Counts in Malaria Infected Symptomatic HIV (Stage 11) Male HIV/ Aids Subjects On Antiretroviral Therapy (Art) in Nnewi, South Eastern NigeriaIOSR Journal of PharmacyNo ratings yet
- Carraro 2013 RSBMTV 46 N 2 P 161Document5 pagesCarraro 2013 RSBMTV 46 N 2 P 161Emerson CarraroNo ratings yet
- Pone 0062323Document10 pagesPone 0062323Malik IbrahimNo ratings yet
- G G Scholar: Pubmed CentralDocument6 pagesG G Scholar: Pubmed CentralIkhsan FebriansyahNo ratings yet
- Attenuation of Sepsis-Related Immunoparalysis by Continuous Veno-Venous Hemofiltration in Experimental Porcine PancreatitisDocument8 pagesAttenuation of Sepsis-Related Immunoparalysis by Continuous Veno-Venous Hemofiltration in Experimental Porcine PancreatitismanuelantoniomenaNo ratings yet
- RT Real-Time PCR Detection of HRVDocument8 pagesRT Real-Time PCR Detection of HRVNashiely RdzNo ratings yet
- Onco 1559mDocument7 pagesOnco 1559mOkki Masitah Syahfitri NasutionNo ratings yet
- Increased Expressions of Integrin Subunit β1, β2 and β3 in Patients with Acute InfectionDocument5 pagesIncreased Expressions of Integrin Subunit β1, β2 and β3 in Patients with Acute InfectionClaudia JessicaNo ratings yet
- Vidas Brahms PCT Procalcitonin Brochure 1Document4 pagesVidas Brahms PCT Procalcitonin Brochure 1swbartlinNo ratings yet
- C-Reactive Protein, Severity of Pneumonia and Mortality in Elderly, Hospitalised Patients With Community-Acquired PneumoniaDocument5 pagesC-Reactive Protein, Severity of Pneumonia and Mortality in Elderly, Hospitalised Patients With Community-Acquired PneumoniaLoserlikemeNo ratings yet
- Septic MarkerDocument10 pagesSeptic MarkerDesti NurulNo ratings yet
- Utility of Cytometric Parameters and Indices As Predictors of Mortality in Patients With SepsisDocument6 pagesUtility of Cytometric Parameters and Indices As Predictors of Mortality in Patients With SepsisPablo VélezNo ratings yet
- J Clin Virol 2020Document4 pagesJ Clin Virol 2020Alejandro Jiménez BlasNo ratings yet
- Cytometry Part B Clinical - 2018 - Garcia Prat - Extended Immunophenotyping Reference Values in A Healthy PediatricDocument11 pagesCytometry Part B Clinical - 2018 - Garcia Prat - Extended Immunophenotyping Reference Values in A Healthy PediatricSabina-Gabriela MihaiNo ratings yet
- Evaluation of Serum Levels of Interleukins 6, 8, 17 and 22 in Acne Vulgaris - A Cross-Sectional Study - PMCDocument10 pagesEvaluation of Serum Levels of Interleukins 6, 8, 17 and 22 in Acne Vulgaris - A Cross-Sectional Study - PMCtisadermaNo ratings yet
- CC 12918Document59 pagesCC 12918Romica MarcanNo ratings yet
- Img#Document5 pagesImg#AngelNo ratings yet
- Chaves 2005 PDFDocument5 pagesChaves 2005 PDFWa Nur Arlin RahmadhantyNo ratings yet
- Early Diagnosis of Sepsis Using Serum Bio MarkersDocument5 pagesEarly Diagnosis of Sepsis Using Serum Bio Markersalemarques16No ratings yet
- Ijpedi2021 1544553Document6 pagesIjpedi2021 1544553Naresh ReddyNo ratings yet
- Carey 2005 CD4 Quantitation HIV + Child Antiretroviral TXDocument4 pagesCarey 2005 CD4 Quantitation HIV + Child Antiretroviral TXMaya RustamNo ratings yet
- Wood-2016-Cytometry Part B: Clinical CytometryDocument7 pagesWood-2016-Cytometry Part B: Clinical CytometryWalter Jhon Delgadillo AroneNo ratings yet
- Predictors of Spontaneous Bleeding in DengueDocument4 pagesPredictors of Spontaneous Bleeding in DengueSawettachai JaitaNo ratings yet
- Clinical Features and CD4+ T Cells Count in AIDS Patients With CMV Retinitis - Correlation With MortalityDocument6 pagesClinical Features and CD4+ T Cells Count in AIDS Patients With CMV Retinitis - Correlation With MortalitysyenadamaraNo ratings yet
- Interpreting PCR Results: Distinguishing Old From Recent COVID-19 InfectionsDocument5 pagesInterpreting PCR Results: Distinguishing Old From Recent COVID-19 InfectionsHitesh MutrejaNo ratings yet
- Simon 2004Document12 pagesSimon 2004mr_curiousityNo ratings yet
- Automated Immature Granulocyte Count in Patients of An Intensive Care Unit With Suspected InfectionDocument7 pagesAutomated Immature Granulocyte Count in Patients of An Intensive Care Unit With Suspected InfectionnissashiblyNo ratings yet
- Cellular immune response to SARS-CoV-2 in uninfected healthcare workersDocument14 pagesCellular immune response to SARS-CoV-2 in uninfected healthcare workersAlexis Guevara QuijadaNo ratings yet
- Kol Ditz 2016Document3 pagesKol Ditz 2016Lanna HarumiyaNo ratings yet
- Enteroviral Meningoencephalitis Case SeriesDocument4 pagesEnteroviral Meningoencephalitis Case SeriesRonald Ivan WijayaNo ratings yet
- Imp bn1Document5 pagesImp bn1Karito FloresNo ratings yet
- Journal SDocument6 pagesJournal SLyla SandyNo ratings yet
- Serum Procalcitonin For Differentiating Bacterial Infection From Disease Flares in Patients With Systemic Lupus ErythematosusDocument29 pagesSerum Procalcitonin For Differentiating Bacterial Infection From Disease Flares in Patients With Systemic Lupus ErythematosusHadi SusilaNo ratings yet
- PCT biomarker accurately diagnoses pediatric appendicitisDocument6 pagesPCT biomarker accurately diagnoses pediatric appendicitisGilang IrwansyahNo ratings yet
- Diagnosis of C.difficile v7.1 + Table and FiguresDocument12 pagesDiagnosis of C.difficile v7.1 + Table and FiguresJuan RecioNo ratings yet
- Plasma Cytokine Profile On Admission Related To Aetiology in Community Acquired PneumoniaDocument9 pagesPlasma Cytokine Profile On Admission Related To Aetiology in Community Acquired Pneumoniahusni gunawanNo ratings yet
- Diagnostic Value of Procalcitonin For Acute Complicated AppendicitisDocument10 pagesDiagnostic Value of Procalcitonin For Acute Complicated AppendicitisAnonymous 4K2TOtpfNo ratings yet
- Consideration of Some Other Specific Indications: BacteremiaDocument18 pagesConsideration of Some Other Specific Indications: BacteremiaMOHAMMAD JOFA RACHMAN PUTERANo ratings yet
- 05 Investigations For PneumoniaDocument4 pages05 Investigations For Pneumoniause4meNo ratings yet
- Analytical Evaluation of a Procalcitonin ImmunoassayDocument5 pagesAnalytical Evaluation of a Procalcitonin ImmunoassayneofherNo ratings yet
- Medical Hypotheses: Yixian Li, Juan Zhou, Ian Burkovskiy, Pollen Yeung, Christian Lehmann TDocument3 pagesMedical Hypotheses: Yixian Li, Juan Zhou, Ian Burkovskiy, Pollen Yeung, Christian Lehmann TAndi BintangNo ratings yet
- Subarachnoid Block For Caesarean Section in Severe PreeclampsiaDocument6 pagesSubarachnoid Block For Caesarean Section in Severe PreeclampsiaAndi BintangNo ratings yet
- Procalcitonin As A Biomarker of Severity Degree in Sepsis Due To PneumoniaDocument5 pagesProcalcitonin As A Biomarker of Severity Degree in Sepsis Due To PneumoniaAndi BintangNo ratings yet
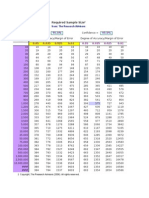
- Required Sample Size: From: The Research AdvisorsDocument3 pagesRequired Sample Size: From: The Research AdvisorsAbhishek Sharma100% (1)
- Anestesia General para Césarea PDFDocument7 pagesAnestesia General para Césarea PDFAgnese ValentiniNo ratings yet
- 1 s2.0 S1052305714000561 MainDocument6 pages1 s2.0 S1052305714000561 MainAndi BintangNo ratings yet
- Bar A Zanchi 2018Document17 pagesBar A Zanchi 2018Andi BintangNo ratings yet
- Parthasarathy2013 PDFDocument7 pagesParthasarathy2013 PDFAndi BintangNo ratings yet
- Anestesia General para Césarea PDFDocument7 pagesAnestesia General para Césarea PDFAgnese ValentiniNo ratings yet
- Cultural Sociology of Mental Illness n28Document5 pagesCultural Sociology of Mental Illness n28Andi BintangNo ratings yet
- Depresión e InmunidadDocument13 pagesDepresión e InmunidadgabisaenaNo ratings yet
- Overweight linked to increased risk of lower back painDocument8 pagesOverweight linked to increased risk of lower back painAndi BintangNo ratings yet
- Sacral Nerve Stimulation Reduces Elevated Urinary Nerve Growth Factor Levels in Women With Symptomatic Detrusor OveractivityDocument5 pagesSacral Nerve Stimulation Reduces Elevated Urinary Nerve Growth Factor Levels in Women With Symptomatic Detrusor OveractivityAndi BintangNo ratings yet
- Instruction For Author ClimactericDocument9 pagesInstruction For Author ClimactericAndi BintangNo ratings yet
- 1 s2.0 S0002937800704534 Main PDFDocument1 page1 s2.0 S0002937800704534 Main PDFAndi BintangNo ratings yet
- 1 s2.0 S0002937803001388 MainDocument3 pages1 s2.0 S0002937803001388 MainAndi BintangNo ratings yet
- 2013 Student Membership ApplicationDocument1 page2013 Student Membership ApplicationAndi BintangNo ratings yet
- 1 s2.0 S0002937803001388 MainDocument3 pages1 s2.0 S0002937803001388 MainAndi BintangNo ratings yet
- Association Between Constipation and Colorectal Cancer Systematic Review and Meta-Analysis of Observational StusdgdiesDocument10 pagesAssociation Between Constipation and Colorectal Cancer Systematic Review and Meta-Analysis of Observational StusdgdiesAndi BintangNo ratings yet
- Prevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationDocument6 pagesPrevalence of Diabetes and Impaired Fasting Glucose in Adults in The U.S. PopulationAndi BintangNo ratings yet
- Anthropometry: Ergonomics Additional ResourcesDocument5 pagesAnthropometry: Ergonomics Additional ResourcesAndi BintangNo ratings yet
- Hepatitis C APASLfghDocument27 pagesHepatitis C APASLfghAndi BintangNo ratings yet
- MK Giz Slide Infant Feeding PracticeDocument1 pageMK Giz Slide Infant Feeding PracticeAndi BintangNo ratings yet
- 1 s2.0 S0021755713002003 MainDocument6 pages1 s2.0 S0021755713002003 MainAndi BintangNo ratings yet
- Urologi PDFDocument237 pagesUrologi PDFAndi BintangNo ratings yet
- Cap Bts 2009 ComplitdgDocument139 pagesCap Bts 2009 ComplitdgAndi BintangNo ratings yet
- 1 s2.0 S0021755713002003 MainDocument6 pages1 s2.0 S0021755713002003 MainAndi BintangNo ratings yet
- Serviks DocjhjuDocument366 pagesServiks DocjhjuAndi BintangNo ratings yet
- PCT CAP ABiuytoDocument10 pagesPCT CAP ABiuytoAndi BintangNo ratings yet
- ATS Guidelines CAP ManagementDocument25 pagesATS Guidelines CAP ManagementMae Matira AbeladorNo ratings yet
- Vol3issue12018 PDFDocument58 pagesVol3issue12018 PDFpyrockerNo ratings yet
- Methodological Literature Review 1 1Document8 pagesMethodological Literature Review 1 1api-584018105No ratings yet
- Intro To Wastewater Collection and PumpingDocument84 pagesIntro To Wastewater Collection and PumpingMoh'd KhadNo ratings yet
- عقد خدمDocument2 pagesعقد خدمtasheelonlineNo ratings yet
- The Precious Little Black Book DownloadDocument226 pagesThe Precious Little Black Book DownloadAsanda YekiNo ratings yet
- Care Plan SummaryDocument5 pagesCare Plan Summaryapi-541785084No ratings yet
- Hvis Msds PDFDocument6 pagesHvis Msds PDFsesbasar sitohangNo ratings yet
- 1.2.1 Log 1Document3 pages1.2.1 Log 1linuspauling101100% (6)
- STP 1560-2013Document346 pagesSTP 1560-2013HieuHTNo ratings yet
- Maintenance Scheduling For Electrical EquipmentDocument82 pagesMaintenance Scheduling For Electrical Equipmentduonza100% (6)
- Prepositions of Time ExplainedDocument18 pagesPrepositions of Time ExplainedyuèNo ratings yet
- NurseCorps Part 8Document24 pagesNurseCorps Part 8smith.kevin1420344No ratings yet
- 11 - Comfort, Rest and Sleep Copy 6Document28 pages11 - Comfort, Rest and Sleep Copy 6Abdallah AlasalNo ratings yet
- OPD Network ListDocument354 pagesOPD Network ListSHAIKH ABDUL AZIZ salim bashaNo ratings yet
- Voyeuristic Disorder SymptomsDocument7 pagesVoyeuristic Disorder SymptomsgoyaNo ratings yet
- Nursing Assignment SampleDocument12 pagesNursing Assignment Sampleswetha swethaNo ratings yet
- Legal Medicine 2020 2021Document4 pagesLegal Medicine 2020 2021Zie DammiNo ratings yet
- Posters Whofic 2020Document107 pagesPosters Whofic 2020Kristel HurtadoNo ratings yet
- UV-VIS Method for Estimating Fat-Soluble Vitamins in MultivitaminsDocument6 pagesUV-VIS Method for Estimating Fat-Soluble Vitamins in MultivitaminsTisenda TimiselaNo ratings yet
- Research Paper About EpilepsyDocument4 pagesResearch Paper About EpilepsyHazel Anne Joyce Antonio100% (1)
- RNTCP - Wikipedia, The Free EncyclopediaDocument5 pagesRNTCP - Wikipedia, The Free EncyclopediaakurilNo ratings yet
- Safety Reports Series No. 13 (Radiation Protection and Safety in Industrial Radiography)Document69 pagesSafety Reports Series No. 13 (Radiation Protection and Safety in Industrial Radiography)jalsadidiNo ratings yet
- Boy Scouts Lipa City Investiture CampDocument1 pageBoy Scouts Lipa City Investiture CampAndro Brendo VillapandoNo ratings yet
- Psychological Impact of COVID-19 Pandemic in The Philippines PDFDocument13 pagesPsychological Impact of COVID-19 Pandemic in The Philippines PDFAndrea KamilleNo ratings yet
- Paul B. Bishop, DC, MD, PHD, Jeffrey A. Quon, DC, PHD, FCCSC, Charles G. Fisher, MD, MHSC, FRCSC, Marcel F.S. Dvorak, MD, FRCSCDocument10 pagesPaul B. Bishop, DC, MD, PHD, Jeffrey A. Quon, DC, PHD, FCCSC, Charles G. Fisher, MD, MHSC, FRCSC, Marcel F.S. Dvorak, MD, FRCSCorlando moraNo ratings yet
- The Cell Cycle and Cancer WorksheetDocument3 pagesThe Cell Cycle and Cancer WorksheetAngie Pyatt KarrakerNo ratings yet
- Q1. Read The Passage Given Below and Answer The Questions That FollowDocument2 pagesQ1. Read The Passage Given Below and Answer The Questions That FollowUdikshaNo ratings yet
- SC 2Document2 pagesSC 2Ryan DelaCourt0% (3)
- 1866 PSC Iasc Ref Guidance t2 DigitalDocument11 pages1866 PSC Iasc Ref Guidance t2 DigitalDama BothNo ratings yet
- Thesis-Android-Based Health-Care Management System: July 2016Document66 pagesThesis-Android-Based Health-Care Management System: July 2016Noor Md GolamNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- The Stress-Proof Brain: Master Your Emotional Response to Stress Using Mindfulness and NeuroplasticityFrom EverandThe Stress-Proof Brain: Master Your Emotional Response to Stress Using Mindfulness and NeuroplasticityRating: 4.5 out of 5 stars4.5/5 (109)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)