k aic osmemri s s i o n on
medicaid
and the
uninsured
K E Y F A C T S
January 2005
MEDICAID SECTION 1115 WAIVERS: CURRENT ISSUES
Medicaid finances health coverage for many low-income with HIV. There are other more targeted waivers under
families and elderly and disabled people. Often poorer Medicaid such as Section 1915 waivers that permit states
and sicker than the privately insured, Medicaid enrollees to enroll Medicaid beneficiaries in mandatory managed
rely on the program for preventive, medical, and long-term care or to provide home and community based services to
care services. The federal government and the states people who would otherwise need nursing home care.
jointly fund Medicaid, with the federal government paying
50% to 77% of Medicaid program costs, depending on the Section 1115 waivers are intended to test and evaluate
state. States administer the program within a combination innovative coverage approaches. By law, Section 1115
of federal standards and state options. waivers are to be used for “research and demonstration”
projects that “further the objectives” of the program. Over
Section 1115 waivers provide a mechanism for states to the years, states have used Section 1115 waivers to test
use federal funds in ways that do not conform to federal new coverage and delivery approaches. For example, in
standards. Section 1115 waivers have been used the 1990s, some states used waivers to test whether
throughout the 40-year history of the Medicaid program. managed care worked well for Medicaid enrollees and led
They can serve as useful tools for states to demonstrate to cost savings; some then used savings to expand
new ways to provide coverage and deliver services to the coverage. These waivers were accompanied by large
low-income population. formal evaluations and paved the way for legislative
changes that gave states the option to implement certain
In recent years, there has been a growing amount of managed care arrangements without seeking a waiver.
waiver activity reflecting a combination of new federal
waiver initiatives and state fiscal pressures. Increased In 2001, the Administration released a new Section
flexibility available through waivers has been promoted as 1115 waiver initiative. The Health Insurance Flexibility
a way for states to cover more people without increasing and Accountability (HIFA) waiver initiative encouraged
program costs. Recent waiver expansion efforts have states to seek Section 1115 waivers to expand coverage
been quite limited and some recent waivers have altered within existing resources and offered states increased
core elements of Medicaid affecting enrollment, benefits, waiver flexibility. At the time HIFA was established, states
and affordability of coverage and care. Increasingly, began facing serious fiscal problems. This combination of
waiver activity has focused on reducing coverage to new flexibility and increasing fiscal pressures has led
relieve state fiscal pressures. some states to use recent waivers as tools to reduce
program spending rather than to expand coverage.
WHAT IS A SECTION 1115 WAIVER?
WHAT KINDS OF CHANGES REQUIRE WAIVERS?
The broadest source of federal waiver authority is
Section 1115 of the Social Security Act. Section 1115 Section 1115 waivers allow states to use federal
gives the Secretary of Health and Human Services broad Medicaid and SCHIP funds in alternative ways. Under
authority to waive statutory and regulatory provisions of waivers, states can change eligibility, benefits and cost-
health and welfare programs under the Social Security Act, sharing in ways that do not meet federal standards and still
including Medicaid and SCHIP, without a statutory change. receive federal matching funds. A state does not need a
States can obtain “comprehensive” Section 1115 waivers waiver to expand Medicaid to children, parents of
to make very broad changes in eligibility, benefits, or cost dependent children, pregnant women, or elderly or
sharing in Medicaid. Currently, 27 states and DC have disabled people; it can do so under regular program
approved comprehensive Section 1115 waivers. Some options. However, waivers are needed to:
have not been implemented, many were adopted primarily Cap enrollment in Medicaid,
to move beneficiaries to mandatory managed care (which
Reduce benefits or increase premiums or cost sharing
states can now do for certain beneficiaries under program
beyond federal standards,
options without a waiver), and others make more
fundamental program changes. Cover adults without dependent children who are not
elderly, disabled, or pregnant through Medicaid,
There are also more narrowly drawn waivers. Some Cover groups other than uninsured children using
Section 1115 waivers focus on specific services or SCHIP funds.
populations such as family planning services or people
1330 G STREET NW, WAS , DC 20005
H I N G T O N
PHONE: 202-347-5270, F A X : 202-347-5274, P U B L I C A T I O N S : 1-800-656-4533
W W W . K F F . O R G
K E Y F A C T S
k aic osmemri s s i o n
HOW ARE WAIVERS FINANCED? waivers to reduce spending have had to pursue additional
Longstanding federal policy requires Section 1115 program cutbacks to address their budget problems.
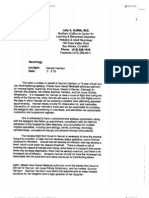
waivers be budget neutral for the federal government. Figure 1
Federal costs under a waiver cannot be more than Examples of Changes to Key Elements of
projected federal Medicaid costs without the waiver. Medicaid through Recent Waivers
States that use waivers to expand coverage must create
Waiver Features Implications
offsetting savings or redirect existing federal funds to Limited benefits and/or new •Limits access to coverage and/or care
finance the expansion. To assure budget neutrality, under or increased premiums •Potential increase in unmet needs and uncompensated care
and/or cost sharing •Reduces state/federal program costs
the terms of a waiver, federal funds for services financed
Different benefits & cost •Allows states to “target” benefit packages
under the waiver are capped for the period of the waiver. sharing for different groups •Increased administrative complexity
States must keep their spending below the caps or within a state •Confusion could dampen participation among people & providers
Enrollment caps •Eliminates guarantee to coverage
assume the full cost of services above the caps. •Enrollment based on first come first serve, not income or need
•Potential increase in number of uninsured and levels of
Some recent waivers use different financing uncompensated care
approaches than previous waivers. In the past, some •Allows states to quickly reduce program costs
Eligibility expansions to •Allow states to cover groups excluded from Medicaid under
states used managed care savings or redirected federal adults without dependent federal law
Disproportionate Share Hospital (DSH) funds to implement children •Size, scope, and implementation limited by availability of state
funds and budget neutrality requirements
coverage expansions to groups that cannot be covered •Coverage and/or care may be limited by enrollment caps,
premiums, limited benefits, and/or cost sharing
without a waiver. Some states also used savings realized
by refinancing fully state-funded coverage with federal
Medicaid matching payments. Today, savings from Some recent waiver changes have eroded coverage
managed care generally are not available to states since and protections for beneficiaries. Waivers permit states
most have already utilized these savings. Recent waivers to impose enrollment caps and to provide more limited
that have sought to expand coverage to new groups are benefits with higher out-of-pocket costs than allowed under
relying on redirected federal SCHIP or DSH funds and federal rules. In some cases the scope of benefits is very
refinancing mechanisms, as well as an approach endorsed limited, for example, without coverage for hospital care.
by HIFA that allows states to achieve “savings” by limiting Enrollment caps enable states to predict expansion
coverage and/or imposing new costs on existing expenditures and limit program spending, but they
beneficiaries. eliminate Medicaid’s guarantee to coverage, which
WHAT ARE CURRENT ISSUES AROUND WAIVERS? requires enrollment of all eligible people who apply.
Enrollment changes to a “first come, first serve” basis
Recent waivers have resulted in limited coverage rather than an entitlement based on income or need.
gains, reflecting the absence of additional federal Limited benefits and increased beneficiary costs reduce
financing. States have had limited ability to fund state and federal program costs, but they may not be
expansions given their difficult fiscal situations and the lack adequate or affordable for covered individuals given that
of additional federal funds under waivers’ budget neutrality they are often sicker and poorer than the privately insured
requirements. Of the 17 Section 1115 waivers approved population. Enrollment drop-offs and problems accessing
since January 2001, 12 included an expansion, but 2 were care due to limited benefits and increased costs can result
not implemented, 2 were only partially implemented, and 5 in unmet need and impose additional strains on providers.
that were implemented were later closed under waiver- CONCLUSION
authorized enrollment caps. In most cases, implemented Although waivers provide states with the opportunity to test
expansions covered a small number of people, sometimes alternative coverage approaches using federal Medicaid
with very restricted benefits. In a few cases, recent funds, recent waivers have focused more on reducing
waivers resulted in coverage losses rather than gains. As program spending. Waivers, however, are not the solution
of Fall 2003, recent waivers had resulted in a net gain in for addressing state fiscal pressures stemming from weak
coverage of about 200,000 people, far less than projected revenues, rising health care costs, and population needs.
coverage gains and a fraction of recent Medicaid Further, without additional financing, recent waivers have
enrollment growth. not been particularly effective vehicles for reducing the
Increasingly, states are using waivers to contain or number of uninsured. Waivers can be useful for testing
reduce spending by altering core program elements. innovation and can sometimes be used to expand
Under waivers, some states have altered many of coverage, but waivers can also have negative
Medicaid’s key elements affecting benefits, affordability of consequences for individuals and providers and may
coverage and care, and enrollment (Figure 1). Such create new fiscal pressures for states over time. Given
changes have generally not resulted in enough savings to that some recent waivers are making fundamental
finance substantial coverage expansions. Rather, states changes in Medicaid, the trade-offs for the low-income,
have increasingly used these changes as a way to reduce elderly and disabled population should be carefully
coverage and relieve state fiscal pressures. However, evaluated and considered and publicly debated.
waiver flexibility does not appear to be sufficient for Additional copies of this publication (#7234) are available on
addressing fiscal problems; some states that have used www.kff.org.
The Kaiser Commission on Medicaid and the Uninsured was established by the Henry J. Kaiser Family Foundation to func-
tion as a policy institute and forum for analyzing health care coverage, financing and access for the low-income popula-
tion and assessing options for reform. The Kaiser Family Foundation is an independent national health care philanthropy
and is not associated with Kaiser Permanente or Kaiser Industries.
You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Power of Attorney in FactDocument7 pagesPower of Attorney in FactJohn Kronnick83% (6)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Finman V CADocument2 pagesFinman V CAAthanasia Zoe GonzalesNo ratings yet
- Doctrine of Proximate CauseDocument17 pagesDoctrine of Proximate CauseAvinash Tiwari100% (1)
- Comprehensive Topics With AnsDocument14 pagesComprehensive Topics With AnsGrace Corpo100% (3)
- Soliman, National Leather, EdralinDocument3 pagesSoliman, National Leather, EdralinjohnmiggyNo ratings yet
- Loadmasters v. Glodel BrokerageDocument3 pagesLoadmasters v. Glodel Brokeragemiles1280No ratings yet
- Rmo 31-2009Document0 pagesRmo 31-2009Peggy SalazarNo ratings yet
- PNRs Faxed 042312Document9 pagesPNRs Faxed 042312Disability MomNo ratings yet
- SDocument2 pagesSDisability MomNo ratings yet
- Hellein Wellcare ComplaintpdfDocument60 pagesHellein Wellcare ComplaintpdffraudblawgNo ratings yet
- 2009 To 2011 Medicaid Membership in For-ProfitsDocument2 pages2009 To 2011 Medicaid Membership in For-ProfitsDisability MomNo ratings yet
- DHS Technical Guidance Appeals - SRG - 06222011Document16 pagesDHS Technical Guidance Appeals - SRG - 06222011Disability MomNo ratings yet
- CIGNA CORP (Form/ 10-K, Received/ 02/23/2012 16/35/12)Document270 pagesCIGNA CORP (Form/ 10-K, Received/ 02/23/2012 16/35/12)Disability MomNo ratings yet
- Medicaid Coverage For Children On The Austism SpectrumDocument7 pagesMedicaid Coverage For Children On The Austism SpectrumDisability MomNo ratings yet
- 6 Company Comparisons AnnualDocument1 page6 Company Comparisons AnnualDisability MomNo ratings yet
- Qexa Prior Notification Request Form FillableDocument1 pageQexa Prior Notification Request Form FillableDisability MomNo ratings yet
- Florida Recovers $27 Million in Medicaid Fraud Settlement - Vital Signs Health Blog - Orlando SentinelDocument2 pagesFlorida Recovers $27 Million in Medicaid Fraud Settlement - Vital Signs Health Blog - Orlando SentinelDisability MomNo ratings yet
- 6 Company Comparisons AnnualDocument1 page6 Company Comparisons AnnualDisability MomNo ratings yet
- 1915i HCBS Fact Sheet 2010Document2 pages1915i HCBS Fact Sheet 2010Disability MomNo ratings yet
- 6 Company Comparisons AnnualDocument1 page6 Company Comparisons AnnualDisability MomNo ratings yet
- HMOs Dispute $34M in State Fines - Sun SentinelDocument2 pagesHMOs Dispute $34M in State Fines - Sun SentinelDisability MomNo ratings yet
- October 2010 Urban Institute Report On Uninsured KidsDocument10 pagesOctober 2010 Urban Institute Report On Uninsured KidsDisability MomNo ratings yet
- Summary of FL Over Payments To Amerigroup WellcareDocument2 pagesSummary of FL Over Payments To Amerigroup WellcareDisability MomNo ratings yet
- Taxpayers Against Fraud False Claims Acts Up To 120810Document24 pagesTaxpayers Against Fraud False Claims Acts Up To 120810Disability MomNo ratings yet
- OIG 2011 Medicare/Medicaid Fraud Fighting PlanDocument159 pagesOIG 2011 Medicare/Medicaid Fraud Fighting PlanDisability MomNo ratings yet
- 42cfr 440.345 EPSDT RequirementDocument36 pages42cfr 440.345 EPSDT RequirementDisability MomNo ratings yet
- Crowell & Moring Managed Care Lawsuit Watch - September 2008Document4 pagesCrowell & Moring Managed Care Lawsuit Watch - September 2008Disability MomNo ratings yet
- April 30 2010 Fed Register Cms 42cfr Part 440 Incl EpsdtDocument67 pagesApril 30 2010 Fed Register Cms 42cfr Part 440 Incl EpsdtDisability MomNo ratings yet
- Dec 2009 Progress of Enrolling in MedicaidDocument10 pagesDec 2009 Progress of Enrolling in MedicaidDisability MomNo ratings yet
- December 2010 Court Order WellCareHealthPlansInc-1Document2 pagesDecember 2010 Court Order WellCareHealthPlansInc-1Disability MomNo ratings yet
- Urban Institute July 2010 PPACA Affect ChildrenDocument5 pagesUrban Institute July 2010 PPACA Affect ChildrenDisability MomNo ratings yet
- Letter of Medical Necessity For Skilled NursingDocument3 pagesLetter of Medical Necessity For Skilled NursingDisability MomNo ratings yet
- Letter Verifying Medical Necessity For DynavoxDocument3 pagesLetter Verifying Medical Necessity For DynavoxDisability MomNo ratings yet
- Sample Doctor Letter For Out of State Specialist TreatmentDocument1 pageSample Doctor Letter For Out of State Specialist TreatmentDisability MomNo ratings yet
- Letter For Out of State TravelDocument2 pagesLetter For Out of State TravelDisability MomNo ratings yet
- Letter of Medical Necessity For Various TherapiesDocument4 pagesLetter of Medical Necessity For Various TherapiesDisability MomNo ratings yet
- Cms State Enrollees in McosDocument1 pageCms State Enrollees in McosDisability MomNo ratings yet
- K Municipal Plan. & Dev. Coordinator KDocument32 pagesK Municipal Plan. & Dev. Coordinator KMary Jane Katipunan CalumbaNo ratings yet
- 3750Document1 page3750Suresh SkvNo ratings yet
- Tax267 FormDocument3 pagesTax267 Form2021202082No ratings yet
- Code of Conduct For Corporate AgentsDocument4 pagesCode of Conduct For Corporate AgentsVijayNo ratings yet
- B2100148 - Dell EMC PowerScale A300Document17 pagesB2100148 - Dell EMC PowerScale A300Le ThienNo ratings yet
- Bluecross EmbezzlementDocument1 pageBluecross Embezzlementthe kingfishNo ratings yet
- InsuranceDocument40 pagesInsurancemanyasinghNo ratings yet
- Sri Lanka Insurance Corporation LTD.: Task 01Document11 pagesSri Lanka Insurance Corporation LTD.: Task 01Saman PathirathnaNo ratings yet
- INSURANCE Asss PrachiDocument3 pagesINSURANCE Asss Prachivbs522No ratings yet
- United India Insurance Company Limited: M/S Neeraj KumarDocument3 pagesUnited India Insurance Company Limited: M/S Neeraj KumarB&R HSE BALCO SEP SiteNo ratings yet
- Sandvik 365 - Crusher & Screening Service ProgramsDocument10 pagesSandvik 365 - Crusher & Screening Service ProgramsBureau d'Etudes et Marketing Sales & MarketingNo ratings yet
- Abhijit Ghosh Dastidar Arijit Ghosh Dastidar $50,000 8 YearsDocument5 pagesAbhijit Ghosh Dastidar Arijit Ghosh Dastidar $50,000 8 YearsPramodJhaNo ratings yet
- Administrative Asst. Resume 1Document3 pagesAdministrative Asst. Resume 1api-12371248No ratings yet
- Turkey Report 2018Document80 pagesTurkey Report 2018Menekşe UçaroğluNo ratings yet
- When Bad Things Happen To Good LawyersDocument77 pagesWhen Bad Things Happen To Good LawyersZeeshan IlyasNo ratings yet
- Rule: Income Taxes: Life-Nonlife Consolidated Returns Tacking Rule RequirementsDocument2 pagesRule: Income Taxes: Life-Nonlife Consolidated Returns Tacking Rule RequirementsJustia.comNo ratings yet
- Gacp Application TemplateDocument8 pagesGacp Application TemplatejackedddaNo ratings yet
- Lafcu Employerbrochure 0714Document2 pagesLafcu Employerbrochure 0714api-239798923No ratings yet
- Insurance C OutlineDocument3 pagesInsurance C OutlineStanley SitholeNo ratings yet
- Sub Contractor W.O. Shrinked FormatDocument2 pagesSub Contractor W.O. Shrinked FormatSourabh SharmaNo ratings yet
- Ordinary Annuity ProblemsDocument1 pageOrdinary Annuity ProblemsJake AustriaNo ratings yet
- Consumer RightsDocument88 pagesConsumer RightsMathangi JeyaramanNo ratings yet