You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Nursing Care Plan AnemiaDocument2 pagesNursing Care Plan Anemiaderic89% (133)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- PELOD2Document13 pagesPELOD2hawinnurdianaNo ratings yet
- Standardized Nursing TerminologyDocument5 pagesStandardized Nursing TerminologyDaniel WainainaNo ratings yet
- Management of Childhood Onset Nephrotic SyndromeDocument13 pagesManagement of Childhood Onset Nephrotic SyndromeJavier ArteagaNo ratings yet
- Hubungan Antara Merokok Dengan Penyakit Parkinson PDFDocument6 pagesHubungan Antara Merokok Dengan Penyakit Parkinson PDFNovita Anggun Permata SariNo ratings yet
- Antenatal Lamivudine To Reduce Perinatal Hepatitis B Transmission PDFDocument7 pagesAntenatal Lamivudine To Reduce Perinatal Hepatitis B Transmission PDFNovita Anggun Permata SariNo ratings yet
- Jenis Batu TerbanyakDocument4 pagesJenis Batu TerbanyakNovita Anggun Permata SariNo ratings yet
- Nidcap Vol 11 No1-FinalDocument26 pagesNidcap Vol 11 No1-FinalDaniel MarvasoNo ratings yet
- Anaesthesia For Neurosurgery PDFDocument6 pagesAnaesthesia For Neurosurgery PDFAnderson LondoñoNo ratings yet
- Mechanical Ventilation: Physiology and Practice, Second EditionDocument2 pagesMechanical Ventilation: Physiology and Practice, Second EditionAnyone ElseNo ratings yet
- Efektivitas Aromaterapi Lemon Untuk Mengatasi Emesis GravidarumDocument8 pagesEfektivitas Aromaterapi Lemon Untuk Mengatasi Emesis Gravidarumsri yulinar pakuNo ratings yet
- Asda Floss - Google SearchDocument1 pageAsda Floss - Google SearchMohammed Al-AminNo ratings yet
- CortisolDocument2 pagesCortisolkitu_alagappan4720No ratings yet
- CASE REPORT - Bronkopneumonia InggrisDocument39 pagesCASE REPORT - Bronkopneumonia InggrisGea AdindaNo ratings yet
- Academy For Healthcare Science: XXXXXXXXDocument25 pagesAcademy For Healthcare Science: XXXXXXXXHidajeta ĐedovićNo ratings yet
- Canadian Contraception Consensus PDFDocument92 pagesCanadian Contraception Consensus PDFMacarena RijoNo ratings yet
- WI-HSD-01 MALVAR Medical ConsultationDocument2 pagesWI-HSD-01 MALVAR Medical ConsultationVictor BaluyotNo ratings yet
- Medicine Matters - January 2018Document11 pagesMedicine Matters - January 2018Kim Kelley-WagnerNo ratings yet
- Ich Safety Guidelines: Presented By: Guided byDocument17 pagesIch Safety Guidelines: Presented By: Guided bysameer22388No ratings yet
- Timeline For Lecture OnlyDocument1 pageTimeline For Lecture OnlyeyesontheskyNo ratings yet
- 100 Item ObstetricsDocument28 pages100 Item ObstetricsTon Ton100% (2)
- Shock ExamDocument3 pagesShock ExamMilagros Fuertes Yosores100% (1)
- Operational Plan Form 2023Document7 pagesOperational Plan Form 2023سحر احمدNo ratings yet
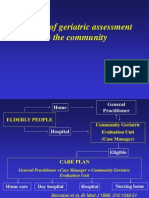
- The Use of Geriatric Assessment in The CommunityDocument16 pagesThe Use of Geriatric Assessment in The Communityhendra2darmawanNo ratings yet
- Iosh Ms Sample MaterialDocument9 pagesIosh Ms Sample MaterialElçin ElçinNo ratings yet
- Types of CataractsDocument1 pageTypes of CataractsMj Baltazar ArtamiaNo ratings yet
- Drug Study Table OkDocument29 pagesDrug Study Table OkRifa'atul Mahmudah100% (1)
- A Comparative Study of European Rare DisDocument7 pagesA Comparative Study of European Rare DisFabiana RaynalNo ratings yet
- Facet Joint Pain-Advances in Patient Selection and TreatmentDocument16 pagesFacet Joint Pain-Advances in Patient Selection and TreatmentthiagoNo ratings yet
- Chapter 8 Drug Administration Throughout The LifespanDocument45 pagesChapter 8 Drug Administration Throughout The LifespanDiane VillegasNo ratings yet
- Care Plan TemplateDocument8 pagesCare Plan TemplateXosweetbebeNo ratings yet
- Poster Presentation - Delayed BathingDocument1 pagePoster Presentation - Delayed Bathingapi-544322316No ratings yet
- Marigold Phase-1 Co-Operative Housing Society LTD: Kalyani Nagar, Pune 411 014Document2 pagesMarigold Phase-1 Co-Operative Housing Society LTD: Kalyani Nagar, Pune 411 014ARCHANNAANo ratings yet
- Orthodontics-Gurkeerat Singh, 2nd EditionDocument704 pagesOrthodontics-Gurkeerat Singh, 2nd Editionkeralaapple85% (34)