You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Marcapasos Cardiaco Externo ST Jude Medical 3077 SpecsDocument2 pagesMarcapasos Cardiaco Externo ST Jude Medical 3077 SpecsJair Jesús Cazares Rojas100% (1)
- Systems of Psychotherapy A Transtheoretical Analysis 8th Edition Prochaska Test BankDocument13 pagesSystems of Psychotherapy A Transtheoretical Analysis 8th Edition Prochaska Test Bankmonicamartinezaekngtcimj100% (15)
- Liver Ki GarmiDocument8 pagesLiver Ki GarmidineshNo ratings yet
- ClexaneDocument2 pagesClexaneianecunar100% (2)
- Direct Post Composite09Document16 pagesDirect Post Composite09hmsatNo ratings yet
- Practice: Further Statistics in Dentistry Part 2: Research Designs 2Document6 pagesPractice: Further Statistics in Dentistry Part 2: Research Designs 2hmsatNo ratings yet
- Practice: Safe and Efficient Use of The InternetDocument12 pagesPractice: Safe and Efficient Use of The InternethmsatNo ratings yet
- 7Document9 pages7hmsatNo ratings yet
- Practice: Failures in Implant DentistryDocument7 pagesPractice: Failures in Implant DentistryhmsatNo ratings yet
- Practice: Lasers and Soft Tissue: Loose' Soft Tissue SurgeryDocument7 pagesPractice: Lasers and Soft Tissue: Loose' Soft Tissue SurgeryhmsatNo ratings yet
- 2 PDFDocument9 pages2 PDFhmsatNo ratings yet
- Managment of Wear2Document7 pagesManagment of Wear2hmsatNo ratings yet
- The Principles of Cavity Preparation (Lecture by DR - Wedad Etman @AmCoFam)Document38 pagesThe Principles of Cavity Preparation (Lecture by DR - Wedad Etman @AmCoFam)AmericanCornerFamily92% (24)
- Reasons For Restorative Therapy and The Longevity of Restorations in AdultsDocument5 pagesReasons For Restorative Therapy and The Longevity of Restorations in AdultshmsatNo ratings yet
- What Is Alzheimer's - Alzheimer's AssociationDocument6 pagesWhat Is Alzheimer's - Alzheimer's AssociationRatnaPrasadNalamNo ratings yet
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationCzafranciscoNo ratings yet
- Short Case Hydrocephalus: by Febrianto Haba Bunga, S.Ked Consultant DR .Donny Argie, SP - BSDocument29 pagesShort Case Hydrocephalus: by Febrianto Haba Bunga, S.Ked Consultant DR .Donny Argie, SP - BSErkoNo ratings yet
- 29a ΙΡΙΔΟΛΟΓΙΑ EGDocument28 pages29a ΙΡΙΔΟΛΟΓΙΑ EGO TΣΑΡΟΣ ΤΗΣ ΑΝΤΙΒΑΡΥΤΗΤΑΣ ΛΙΑΠΗΣ ΠΑΝΑΓΙΩΤΗΣNo ratings yet
- 1 - Series 2022Document9 pages1 - Series 2022Vijay U100% (1)
- FNB-Minimal Access Surgery: Competency Based Training ProgrammeDocument31 pagesFNB-Minimal Access Surgery: Competency Based Training ProgrammeAMBUJ KUMAR SONINo ratings yet
- MarijuanaDocument8 pagesMarijuanajohnkyleNo ratings yet
- Sweage Treatment Plant (STP)Document57 pagesSweage Treatment Plant (STP)pra311288No ratings yet
- Dispelling Myths About Drinking Distilled WaterDocument6 pagesDispelling Myths About Drinking Distilled WaterPau StraitNo ratings yet
- Mastery Question MDFDocument66 pagesMastery Question MDFshaaish100% (1)
- Gabel 2013Document12 pagesGabel 2013rahulNo ratings yet
- Simple Interrupted Suture (Silicon Skin Pad)Document11 pagesSimple Interrupted Suture (Silicon Skin Pad)Yusuf LawalNo ratings yet
- Mmvr19 / Nextmed Conference ScheduleDocument21 pagesMmvr19 / Nextmed Conference SchedulepvaldastriNo ratings yet
- What Are The Benefits of An Intensive Outpatient ProgramDocument2 pagesWhat Are The Benefits of An Intensive Outpatient ProgramDan MarkNo ratings yet
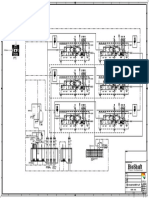
- P&ID - STP-Yanbu SWCC (6units)Document1 pageP&ID - STP-Yanbu SWCC (6units)Ashraf BayomiNo ratings yet
- Batiquin v. Court of AppealsDocument9 pagesBatiquin v. Court of AppealsEnzo PerezNo ratings yet
- Top 10 Stress Management TechniquesDocument5 pagesTop 10 Stress Management TechniquesMaryjane YaranonNo ratings yet
- Greywater RecyclingDocument9 pagesGreywater RecyclingLee Kok HuaNo ratings yet
- Letter To Mrs. Clinton-May 1993-By Trudy Attenberg-Face ForwardDocument2 pagesLetter To Mrs. Clinton-May 1993-By Trudy Attenberg-Face ForwardNeil GillespieNo ratings yet
- GowthamiDocument35 pagesGowthamiDR VENKATARAMANA MurthyNo ratings yet
- Volume3 Issue8 (4) 2014Document342 pagesVolume3 Issue8 (4) 2014iaetsdiaetsdNo ratings yet
- Stress Burnout - Georgeann RoudebushDocument45 pagesStress Burnout - Georgeann RoudebushVinnyYusrainiNo ratings yet
- Cyst Theory ClassDocument310 pagesCyst Theory ClasswakoNo ratings yet
- Tina Dobbs Health Department ReportDocument12 pagesTina Dobbs Health Department ReportAdamCareyNo ratings yet
- IndomethacinDocument17 pagesIndomethacinRajpal Singh KochharNo ratings yet
- Sex ChangeDocument17 pagesSex ChangesoberanoriofionaNo ratings yet