You might also like
- Diabetic KetoacidosisDocument16 pagesDiabetic Ketoacidosisjoyshe111100% (2)
- DKADocument64 pagesDKAAravindhan Gunasekaran PaediatricianNo ratings yet
- Diabetic Ketoacidosis Case PresentationDocument37 pagesDiabetic Ketoacidosis Case PresentationNathan Vince Cruz100% (2)
- Diabetic Ketoacidosis: Presented by The Students From Roll Numbers 31 - 40Document20 pagesDiabetic Ketoacidosis: Presented by The Students From Roll Numbers 31 - 40HUSSAIN NAZEESHANo ratings yet
- GlomerulonephritisDocument8 pagesGlomerulonephritisMatthew Ryan100% (1)
- Diabetic KetoacidosisDocument3 pagesDiabetic KetoacidosisJanna FavilaNo ratings yet
- Diabetic Ketoacidosis (Dka)Document16 pagesDiabetic Ketoacidosis (Dka)yazid100% (5)
- Nursing Care Plan For "Diabetes Mellitus - Diabetic Ketoacidosis"Document17 pagesNursing Care Plan For "Diabetes Mellitus - Diabetic Ketoacidosis"jhonroks97% (36)
- DialysisDocument5 pagesDialysisAnusha Verghese100% (1)
- Case Study: Diabetic KetoacidosisDocument66 pagesCase Study: Diabetic Ketoacidosisllaychin100% (2)
- DKA (Diabetic Ketoacidosis)Document3 pagesDKA (Diabetic Ketoacidosis)Hassan.shehri83% (6)
- Nursing Care Plan of CataractDocument3 pagesNursing Care Plan of CataractDimzmonyo100% (1)
- Myocardial InfarctionDocument18 pagesMyocardial Infarctionporing500No ratings yet
- Diabetic Ketoacidosis Case StudyDocument6 pagesDiabetic Ketoacidosis Case StudyHomework Ping100% (2)
- Hyperosmolar Hyperglycemic Nonketotic Syndrome (HHNS)Document8 pagesHyperosmolar Hyperglycemic Nonketotic Syndrome (HHNS)amiraNo ratings yet
- Acute Renal FailureDocument34 pagesAcute Renal Failureaibaloca67% (9)
- Acute Liver FailureDocument3 pagesAcute Liver FailureElisabeth F. OjhaNo ratings yet
- Chronic Renal FailureDocument54 pagesChronic Renal Failuresanjivdas100% (3)
- Acute Kidney FailureDocument8 pagesAcute Kidney FailureRaidis PangilinanNo ratings yet
- Acute Glomerulonephritis: Mohd Zamir Ghouse 060100848Document40 pagesAcute Glomerulonephritis: Mohd Zamir Ghouse 060100848zamirsg100% (1)
- CopdDocument60 pagesCopdRizqy Shofianingrum100% (1)
- DKA ManagementDocument59 pagesDKA Managementnatalieshirley100% (1)
- Chronic Renal FailureDocument37 pagesChronic Renal Failuredorkiebaby100% (10)
- Fulminant Hepatic FailureDocument8 pagesFulminant Hepatic Failuremiz uNo ratings yet
- Cardioversion and DefibrillationDocument18 pagesCardioversion and DefibrillationJannah Marie A. Dimaporo100% (4)
- Diabetic Ketoacidosis Case StudyDocument5 pagesDiabetic Ketoacidosis Case Studyjc_albano29100% (7)
- Hepatic EncephalopathyDocument3 pagesHepatic EncephalopathySuhas KandeNo ratings yet
- Renal FailureDocument33 pagesRenal FailureDeniela Jamaicy Herbert100% (6)
- Angina PectorisDocument11 pagesAngina Pectorisjialin80% (5)
- Nephrotic SyndromeDocument61 pagesNephrotic SyndromeRanah Julia Garchitorena AyoNo ratings yet
- Chronic Renal FailureDocument13 pagesChronic Renal FailureAnusha VergheseNo ratings yet
- Diabetic KetoacidosisDocument4 pagesDiabetic KetoacidosisHasan A. AsFourNo ratings yet
- Angina PectorisDocument17 pagesAngina PectorisRacel HernandezNo ratings yet
- 8 Liver Cirrhosis Nursing Care PlansDocument4 pages8 Liver Cirrhosis Nursing Care PlansAngie MandeoyaNo ratings yet
- Diabetes InsipidusDocument21 pagesDiabetes InsipidusMoni RethNo ratings yet
- SHOCKDocument17 pagesSHOCKChithra Saju100% (1)
- DkaDocument83 pagesDkaRajaKumar Ponnana100% (1)
- Renal FailureDocument41 pagesRenal Failure12046No ratings yet
- 14.malabsorption SyndromesDocument5 pages14.malabsorption SyndromesPriyaNo ratings yet
- Nephrotic SyndromeDocument65 pagesNephrotic SyndromemejulNo ratings yet
- Nursing Care Plan For Heart Failure ChronicDocument26 pagesNursing Care Plan For Heart Failure ChronicbrantNo ratings yet
- 2 NCP Chronic Heart FailureDocument5 pages2 NCP Chronic Heart FailureLovely CacapitNo ratings yet
- Acute Renal FailureDocument35 pagesAcute Renal FailureKaelyn Bello Giray100% (1)
- Syndrome of Inappropriate Secretion of Anti Diuretic HormoneDocument39 pagesSyndrome of Inappropriate Secretion of Anti Diuretic Hormonefarmasi_hmNo ratings yet
- Diabetic KetoacidosisDocument22 pagesDiabetic KetoacidosismartinNo ratings yet
- Complications of Diabetes Mellitus-UpdateDocument48 pagesComplications of Diabetes Mellitus-UpdateAnditha Namira RS100% (1)
- Copd Health TeachingDocument2 pagesCopd Health TeachingMel Sevilla100% (1)
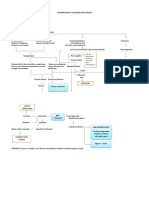
- Pathophysiology of Diabetic KetoacidosisDocument2 pagesPathophysiology of Diabetic KetoacidosisGeevine CansinoNo ratings yet
- Pyloric StenosisDocument3 pagesPyloric Stenosismagisasamundo100% (1)
- Diabetic KetoacidosisDocument6 pagesDiabetic KetoacidosisRain Catan Gagarra Saquin100% (1)
- 13.acute Respiratory FailureDocument34 pages13.acute Respiratory Failurekarim hassan100% (1)
- Acute Renal FailureDocument17 pagesAcute Renal FailureDina Rasmita100% (1)
- Case StudyDocument6 pagesCase StudyApoorv Jain100% (1)
- Diabetic Ketoacidosis Case StudyDocument6 pagesDiabetic Ketoacidosis Case StudyJohn AlcantaraNo ratings yet
- 128 Diabetic KetoacidosisDocument9 pages128 Diabetic KetoacidosisDite Bayu NugrohoNo ratings yet
- DKADocument5 pagesDKAMariel BernabeNo ratings yet
- Disorders of Carbohydrate Metabolism.: Abdelmoniem Saeed Mohammed Er SpecialistDocument49 pagesDisorders of Carbohydrate Metabolism.: Abdelmoniem Saeed Mohammed Er SpecialistYousef Al-AmeenNo ratings yet
- Dka and HHSDocument25 pagesDka and HHSMouhammad Dawoud100% (2)
- Metabolic EmergenciesDocument53 pagesMetabolic EmergenciesWengel Redkiss100% (1)
- Dka 1Document16 pagesDka 1Dina M ElbakaryNo ratings yet
- Carpentry ToolsDocument2 pagesCarpentry ToolsJill Catherine CabanaNo ratings yet
- Chest Tube ThoracostomyDocument17 pagesChest Tube ThoracostomyJill Catherine CabanaNo ratings yet
- NCP Activity IntoleranceDocument2 pagesNCP Activity IntoleranceJill Catherine CabanaNo ratings yet
- Trizole, PrevacidDocument1 pageTrizole, PrevacidJill Catherine CabanaNo ratings yet
- Gestational DiabetesDocument2 pagesGestational DiabetesReyniel Pablo ElumbaNo ratings yet
- Diabetes y Embarazo ADA 2023Document13 pagesDiabetes y Embarazo ADA 2023Efrain FernandoNo ratings yet
- Pharmacon Poster 2021Document1 pagePharmacon Poster 2021api-592676308No ratings yet
- Case StudyDocument4 pagesCase StudyCecil AguilarNo ratings yet
- Diabetes Freedom Reviews - Does It Really Work or Scam?Document7 pagesDiabetes Freedom Reviews - Does It Really Work or Scam?Diabetes FreedomNo ratings yet
- April: Application of Nursing Theory "Orem's Self-Care" Into PracticeDocument33 pagesApril: Application of Nursing Theory "Orem's Self-Care" Into PracticeAli AlmarzoogeNo ratings yet
- DM GDMDocument40 pagesDM GDMPatiphan PeeyuhaNo ratings yet
- BMIDocument16 pagesBMIMarc Junuel Romen100% (1)
- Dolfi Herscovici, Jr. (Eds.) - The Surgical Management of The Diabetic Foot and Ankle (2016, Springer International Publishing)Document204 pagesDolfi Herscovici, Jr. (Eds.) - The Surgical Management of The Diabetic Foot and Ankle (2016, Springer International Publishing)Pranitha PaidiNo ratings yet
- Diabetes SobrebasalizaciónDocument7 pagesDiabetes SobrebasalizaciónComisión Académica FCM - UNAHNo ratings yet
- Surpass 1 Journal Club CritiqueDocument3 pagesSurpass 1 Journal Club Critiqueapi-589696674No ratings yet
- Human and Social Biology SBADocument12 pagesHuman and Social Biology SBATamoy Noble100% (1)
- Glucose Tolerance TestDocument11 pagesGlucose Tolerance TestDharmikPatelNo ratings yet
- 15-Item DMSES UKDocument2 pages15-Item DMSES UKkumalaselvia49No ratings yet
- Isglt2 Nefirits LupicaDocument2 pagesIsglt2 Nefirits LupicaAldo Amed Montaño SalinasNo ratings yet
- English Manual XceedDocument33 pagesEnglish Manual XceedNico IturbeNo ratings yet
- Yuwell Accusure 510 ManualDocument20 pagesYuwell Accusure 510 Manualrepolho1234No ratings yet
- Semaglutifes Sustaine ComparadoresDocument10 pagesSemaglutifes Sustaine ComparadoresIvan Dario Hernandez ErazoNo ratings yet
- Nefropatia DiabeticaDocument13 pagesNefropatia DiabeticagerardoNo ratings yet
- Urine Analysis in Community SettingDocument3 pagesUrine Analysis in Community SettingAdri SinclaireNo ratings yet
- Worksheet ANSWER KEY Chapter 7 BIO-CLASSDocument13 pagesWorksheet ANSWER KEY Chapter 7 BIO-CLASSUCL SportsNo ratings yet
- Assessment of Factors Influencing Adherence To AntDocument7 pagesAssessment of Factors Influencing Adherence To AntJob MarenNo ratings yet
- Group 1 PR2Document10 pagesGroup 1 PR2Hans Elliza BartocilloNo ratings yet
- Dr. Bernstein's Diabetes Solution - The Complete Guide To Achieving Normal Blood Sugars 1Document10 pagesDr. Bernstein's Diabetes Solution - The Complete Guide To Achieving Normal Blood Sugars 1Artack50% (2)
- The Effect of A Combination Treatment of Biomagnetic Therapy and A Low Glycaemic Influenced Diet On Nonfasting Blood GluDocument8 pagesThe Effect of A Combination Treatment of Biomagnetic Therapy and A Low Glycaemic Influenced Diet On Nonfasting Blood GluDiana DíazNo ratings yet
- Approach To Diabetes Mellitus in YoungDocument41 pagesApproach To Diabetes Mellitus in YoungLalrin ChhanaNo ratings yet
- Understand Diabetes and Take Control - BanglaDocument23 pagesUnderstand Diabetes and Take Control - BanglaInternational Diabetes Federation100% (2)
- Diabetes Cheat Sheet Copyright BNDocument2 pagesDiabetes Cheat Sheet Copyright BNJeshan Yanong BeltranNo ratings yet
- 6Document5 pages6ρενα μινορεNo ratings yet
- Diabetes PathophysiologyDocument2 pagesDiabetes PathophysiologyRyan MulanoNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (28)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (2)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)No ratings yet
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (58)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)
- Troubled: A Memoir of Foster Care, Family, and Social ClassFrom EverandTroubled: A Memoir of Foster Care, Family, and Social ClassRating: 4.5 out of 5 stars4.5/5 (27)