Professional Documents
Culture Documents
High Yield Embryology
Uploaded by
Khadim ShahOriginal Description:
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
High Yield Embryology
Uploaded by
Khadim ShahCopyright:
Available Formats
~ .. _..
._.. _4_
. __........ _-_..-..
._-----
WWI ,.. & Wilkin
__'... 5<_01- .
igh-YedEb yology
Ronald W. Dudek Ph.D.
Dep;"irrrnen ( Anawmy :md Cl.'ll Biol(x:y
Ea<.:t Carotin:1 Universiry
()f Medicine
Greelwllle, North Car;l[in;J
WillianlS & vVilkins
A Wi\YERLY COMl',\h .
Bill-llll RF' 1'f'IL\Df.lI'flI.\ 1 f), DOl, P\Rls ,INloWI
1.11 I.NUI ..\ I.IOM, 1.0 11> .\1l'N:t II' \III.NL > HlKiIJ .1V1t1l('[J\\\'
1996
igh-Ye E___
Ronald W. Dudek, Ph.D.
Dep;"irrrnen of Anawm'y ::md Cdl Rinl(x:y
Carotin:) Universtry
of Medicine
LJrte!1\'IJle, North Canlm;J
I'ia\
WillianlS & vVilkins
A Wi\YERLY COMl'XN .
BALll\1 RF' 1'f'IL\Df.lI'HI.\ 11), DO:,' PARIS " ,'''<GWI
ill 110 (, kO t,' Ml N:r 'II II I !m:\IJ \vIlU! 'l'IIV
1996
Prefertilization Events
I. OVERVIEW. Gametes (oocytes and spermatozoa), descenJants l)f primordial germ cells,
are produced in the adult hy either oogenesis or spermatogenesis, that involve
meiosis. PnmorJl<l1 genn. cells originate in the wall of the yolk sac of the cmLryo ,mJ
mlgrarc tn the gon,idal re ion.
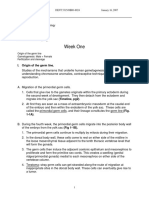
II. MEIOSIS (Figure 1-1), which occurs only during the productio of gametes, of
twO cell divisions (meiosis 1 and meiosis II) anJ results in tile fannation of four gametes
ontilining 23 <...hrumu1Jomes and IN amount of DN (23,lN). Meiosis:
A. Reduces the number of 1tomosomes within gametes to ensure that the human species
number of chromosomes (46) is maintainc from gen ration 10 generation
B. Redistribute maternal and paternal chromosomes to insure 'enetic ariabihty
C. Promotes the xchange of small amOlmts of maternal and paterna D A via crossover
III. FEMALE GAMETOGENESIS (OOGENESIS; able 1-1)
A. Primordial germ cells (46,2N) arrive in the ovary at week 4 of embryunic development
and differentiate mto oogonia (46,2N).
B. Oogonia enter meiosis I and undergo DNA replication to form primary oocytes
(46,4N). All primary oocytes are formed by the fifth month of fetal life and remain
dormant in prophase (dictyotene) of meiosis I until puberty.
C. During a woman's vari cy Ie, a ptimary ol1cyte completes meiosis I to form a second-
ary ocyte (23,2N) and a first polar body, which probably degenerares.
D. The secondary oocyte enter' meiosis II and ovulation occurs when the chromosomes
align at metaphase. The :;econdary oocyre remains arrested in metaphase of meiosis II
until fertilization occurs.
E. At fertilization, the secondary oocyte completes meiosis 11 w farol a mature oocyte
(23,lN) and a second ar body.
IV. MALE GAMETOGENESIS
A. Spermatogenesis
1. Primordial germ cells (46,2N) arrive in the testes at week 4 of embryonic develop-
ment and remain clonnanr until puberty. At puberty, primordial germ cells differen-
tiate into type A spermatogonia (46,2N).
1
:J.
Prefertilization Events
I. OVERVIEW. Gametes (oocytes and spermatozoa), c$cenJants uf primordial genll cells,
are produced in the adult hy oogenesis or spermatogenesis, that involve
meiosis. PnrnorJl(Il genu cells odginatc 111 the wall of the yolk sac of the eml.ryo unJ
mlgr<lre tn the gon,lJal ion.
II. MEIOSIS (Figure 1-1), which occur' only during the productiol of gametes, of
two cdl Jivtslons (meiosis 1 anJ meiosis II) anJ results in Ute formation of four gamete.
ontaming 23 ChrUlllUSomc' and IN amount of ON (23,lN). Mciosi::
A. Reduce.,> the num er of c romosomes within gamere ro en.... ure thar me human
number of chrom ames (46) is maintainc from gen rotion to generation
B. Rcdlstribute maternal and paternal chromosome.... t( Insure 'cnetic ariabtllty
C. rhe xchangc ot small amounts of materna anJ paterna 0 A vi:'! crossover
III. FEMALE GAMETOGENESIS (OOGENESIS; able 1-1)
A. Primordial germ cells <46,2N) amve in the vary at week 4 of embryunic Jevdllpnwm
and differentiate mto oogonia (46,2N).
B. Oogonia enter meiosis 1 and undergo DNA replication to form primary oocytes
(46,4N). AIL primary oocyte, <'lre formed by the fifth month of fetal life and remain
dormant in prophase (dictyotene) of meiosis I until puberty.
C. During a woman's varia LY Ie, a 1J11mary oocyte completes meiosis 1to form a second-
ary ocyte (23,2N) and a first polar body, which probably degenerates.
D. The secondary oocyte enters meiosis lJ an.d ovulation occurs when the
align at metaphase. The secondary oocyte remains arrested in metaphase of meiosis II
until fertilization. occurs.
E. At fertilization, the secondary oocyte completes meiosis 11 to fuml a mature oocyte
(23,lN) and a second ar body.
IV. MALE GAMETOGENESIS
A. Spermatogenesis
1. Primordial germ cells (46,2N) arrive in the testes at week 4 of embryonic develop-
ment and remaIn dormant until puberty. At pu erty, primordial germ cells differen-
tiate into type A spermatogonia (46,2 ).
1
2 Chapter 1
Dog""'a 0' ,peooalogoo', (46, 2N)
DNA replication
Meiosis 1
gam"""yte (46, 4N) @
t
@sy,..,.,
t
@crossover
+
Alignment and disjunction
Centromeres do not split
rw/cell rY\
Secondary gametocyte (23, 2N)
Gamete (23, 1N
MeiosIs II
(MX:: Alignment and disjunction
Centromeres split
J/
c
II . ""
Qj d'"'''oO)
Figure 1-1. Non' r toni\' one p81r of . or.101 gODS chromosomes is shown (whIte = mat.ern;!!
Ilgu ; !>luck -= paternal origin). SynapsIs IS the proces" of pamng of hOlno)llgnus chromosomes. The raint at
whl h the DNA molecule crosses over, the chiasma, is wlwrc t.hc exchange of :-.mallllmounts of maternal and
pat mal DNA takes pIa e. (Mudifid with peomssion trOllt Fix jOimd Dudek RW: BRS Emtnyo!vgy, altimore,
Williams & Wilkim, 1995, p 4.)
Preferlilization Events 3
............................................................................................................................................................., .....
2. Type A spermatugonia undergo mitosis to form eirher more type s ermatogonia
(to maintain the ,up Iy) or typ B spermatogonia (46,2N).
3. Type f\ spermalOgonl<1 enter meiosis I and undergo DNA replication to (orm primary
spcrmatocytes (46,4N).
4. Pnmarv :>pcrmarocyte meiOSIS I to for two secondary spermatocytE'S
(23,2N).
5. Second'lry ,permcltucyre:> complete JIt:> [nnn four spermatids (23, IN).
B. is;) post-meiotic series of morphological ch::mge. withm rh' spermatid
that results in the formation of the head, booy. and t(lil of the sperm (23,lN).
C. Capacitation. Newly cj<lcldatcd sperm arc inGlpabk of fertiUz:3l!on unril they ndergl)
c.:lr;H-:ir::lt!lln, which occurs in the female reproJuctivc rraLr anJ tbe mmask!ng
01 Sf' I'm and elllO 'cd of the proteins tha[ (llU[ thc 5unacc of thl;
Table 1-1
Numher (If Chromos(Jmcs <lnd Amount of DNA Contamed In Cell., During the :)ta 'es of
Gamerogenesis .
CelJ
Primordial germ cell, oogonia.spennatogonia (types A and B)
Primary oocyte. primary spermatocyte
Secondary 0 cyte. secondary spermatocyte
Oocyte (ovam). spermatid. sperm
Number of Chromosomes
Amount of DNA
46.2N
46,4N
23,2N
23,lN
Week 1 (Days 1-7)*
I. OVERVIEW. Figure 2-1 summarizes the events that lJCCUr during week.l, fClllowing fen diza-
rion.
II. FERTILIZATION Ol.:curs in the ampulla of the uterine tube.
A. The sperm binds to the zona pellucida ofthe secondary u<)cyt e and the aCrOsome
reaction, causing the release of aCH\somal enzymes (e.g.. acrosin.
B. Aided by t l' :lcr enzymes, the Spero1 penetrates the zona pellucida. I enetration
of the zona elluciJa elicits the cortical reaction, rendering the secondary oocyte im-
pemleablc to other sperm.
C. 11112 sperm and secondary oocyte cell membranes fuse, and the wntents 0f the speml
t'llter the cytoplasm of clw oocyte.
1. The male genetic material forms the male pronucleus.
2. The tall and mirochon ria of the sperm degenemte. Therefore, all mi[()chc)J dria
within. the Vgote are of maternal origin (i.e., all mitochondriClI ONA is of maternal
origin).
D. The sec< ndar f oocyte complete;, mei(\si.: II, lorrnlllg' a mature ovum. he nucle-us of
d ( ovum is the female pNllUcleus.
E. Th milk and female pronuclei (use lO fon 1 :-l zygote.
III. CLEAVAGE is a series of mitotic of rhe zygote.
A. 111(' zygote cytoplasn1 is successively cleaV\:d to form a blastula CQosistm' of tncre(lsinglv
mailer (e.g., the first blastomere stage of 2 cells; the ne. '1, 4 cells;
the next, 8 C lis).
B. A r.he H-cell stage, the blastometes fom1 a morula consisting of Oln inner cell mass
and an outer ceU mass.
The' ge of tbe developing concepeu.s can he ci .her from the e.mmateJ day of kmlizatioll (fcrtil.i=a-
tion age) (it from the day of the last normal menstrual period (LNMP). !n thts bx.,k, ages arc presented as
the fcrttllzati.on age.
4
Week 1 (Days 1-7) 5
IV. BLASTOCYST FORMATION occurs when fluid secrered within the morula forms the
blastocyst cavity.
A. The inner cell mass, which will eventually become the embryo and IS c!esign(lred
the cmbryoblast.
B. h outer celi mass, which part of the placenta, is designated the trophoblast.
V. IMPLANTATION
A. The zona pellucida must degenerate for uupl::tnratlon EO C ur.
B. The blastucyst 1l0P Llms within rite functional layer or the enc!<.lmetrium during the
secretory phase of tJ1C menstrual cycle.
1. Implaontion II l;ll1y ()Cellrs on the posterior superior wall (\f [ht' Ulerus.
2. Ectopic tubal pregnancy occurs when the blasmcyst iIll .lants wi hi n rhe n('
tube.
C. The IT,.phoblast differentiates IOto the cytotrophoblast and syncytiotropboblast.
/
Blastocyst
.oflII(-------
----.,,q--- Blastocyst cavity
Morula
Embryoblast
4-Cell
blastula
Blastomer
Zona pelluclda
2-Cell
blastula
Day 7
B
Cytotrophoblast
Syncytiotrophoblast
Fertilization
A
Zygote ---tt
Secondary
oocyte
arrested in
metaphase
Figure 2-1.. (A) The oj 1uman development dunng week 1. (8 A day 7
5
3
Week 2 (Days 8-14)
l. EMBRYOBLAST (Figur 3 1), The dlffercmiates into wo disrinc cell layers,
the epiblast and hypobla:>t, fUlllli.llg a bilaminar embryonic disk.
A. Epiblast. Clefts de clop Ilthin the epiblasr 1'0 form th amniotic cavity.
B. Hypoblast cells migrate ailing tl1l cytotrophnhlast, forming the yolk sac.
C. The prochordal plate. formcd (n..lIll the fUI.'ion ot hypohlasr and e ihl:tst cells, marks the
sire of the future mouth.
II. TROPHOBLAST
A. The syncytiotrophoblast continues Its growth n(O [h endometrium make contact
WIU1 cndl'metrial 1:'>lood ve sets and gland-.
1. The syncytiotTophohla. t does not divide mitotically.
2. nle $ 'ocytiotror oblast pI' human chorionic gona otropin a glyco
pmtein thar'timlilates the production of wgesterone In the corpus luteum. heG
c;:In be assayeJ m maternal blood (11' urine at day 0 and is r.hl" hasis (;f (,;:tIly pre .nancy
diagnoSIS.
B. 'n1e cytotrophoblast does divide miwriGllly, a ding tn the gr()\ t 1 (t 1.C;y .cyriottopho-
biast. Primary chorionic villi protrude into the
III. EXTRAEMBRYONIC MESODERM is (l new la.yer of cclb Jcrivcd from the epiblast.
A. Extraembryonic SOtrultic mesoderm lines the cytutrophuhl<olst, tC}mlS the umnecting
stalk, and cover. the anu1ion (see Figure }.1).
1. the conce is upended y the connecting wIthm t1e \.horioni(; cavity.
2. The waH of he chOrionic Glviry is called the chorion anJ cnnsisrs of I he extraembry-
onic somdtic mc:-;oJenn, the cytotrophohlast, nnd the
B. xtracmbryonic visceral mesoderm cove . the olk sac.
Week 2 (Days 8-14) 1
IV. CLINICAL CORRELATIONS
A. Hydatidiform mole. A blighted bLastocyst lea s to dearh...Qf the emhryo, which is
followed by hYPt'rpla'ltic of the trorhoblast within the lIterine wall.
B. Choriocarcinoma is a malignant tumor of the uuphoblasl Ihat may occur ("llllwing a
pr<:gnancy, abortion, or a hydatidiform lw)k.
0/-0 Iro('hoblGot
.
Connecting stalk
Prochordal plate
Chorion
-
TYl-!,;&d",.."
Primary chorionic villi
Extraembryonic
somatic
mesoderm
Extraembryonic /
visceral
mesoderm
Endometrial
gland
Endometrial ------t'J
blood vessel
Synr.ytiotrophobla5t
Amniotic caVity
Yolk sac -----+H
Cytotrophoblast
Chorionic ----+--f-==+-(&;H--
cavity
Figure 3-1.
implanraLio(l
A ,Jdy 14 blasw<:ys[. .A.t thb swge, ormation of the bilamin<tr embryonic disk occurs, anJ
id1111 the 'ndomctrium 's completcJ.
8
4
Embryonic Period (Weeks 3-8)
I. INTRODUCTION. All major orga systems hegin LO develop during the embryonic period,
causing a cranLOcaudal and lateral body folding )f the embryo. By tht' end oj the embryonic
period (week 8), the embryo has a di tinct human appeamncc.
II. GASTRULATION (Figure 4,l) is the process that establishes the three primary genu layers:
ectoderm, mesoJerm, and endoderm.
A. Gastndation is initiated by the formation of the primitive streak wIthin the epi l<lsI.
B. All eelli and tissues of the adult can be traced back to the three primary germ layers.
1. Ectoderm
a. Surface ectodeml
(1) Len of the eye
(2) Adenohypophysis
(3) tride, semicircular ducts, anJ vestibular ganglion of cranlal nerve (CN)
III
(4) SaccuIe, cochlear duct (organ l f Com), and spiral gangl i0 of 'N VIl1
(5) Epithelial lining of the external audilory meatus
(6) lfactory lacode, including eN 1
(7) Epithdiallining of the i1merior two rhirds of the t( nguc, the hard paJat(',
sides of the mouth, Jnd paroti(l glands and duct;
(8) Mammary glands
(9) Epithelial lining of the lower anal canal
(10) Epithelial lining of the distal penile urethra
(1:1) E idermis, hair, nails. SWC<Jt dnd cutaneous glands
b. Neuroectoderm
(1) All neurons within the central nervo s system (CNS), mcluding the pre-
ganglionic sympm}wtic ; od preganglionic rarasymrathclic neurons
(2) Asrrocyres,oligoden,drocytes, pendymocytes, tany\.ytes, haroid rlexus
cells
(3) Rellnil
(4) Pineal gbnd
(5) Neurohypophysls
c. Neural crest
(1) Postganglionic syrnpatheLlC neurons within the Sy11lpat 1et\c chain ganglia
i1nd prcvertehral gangl.ia
Embryonic Period (Weeks 3-8) 9
(2) P(1slgang!lonic parasympathetic neurons within t..he ciliary, pterygopala-
line, :ubmandihllir-lr, otic, enteric ganglia, rmd ganglia of the abdominal
and pelvic Glvlties
(3) Sen ory wit.hin the dorsal root ganglia
(4) Schwarm cells
(5) Pia mater and anJChn\)ld membrane
(6) Chromilffin cells of th. adrenal medulla
(7)
(8) Maxilla, zygomatic on\', lemporal bone, palatine bone, vomer, mandible,
hard palate, inCUS. malleus, stapes, sphenomandibular ligam.enl,
JOCf>SS, srylohYOId Iigament, hYOid bune, frontal one, parietal bonl',
sphenoid bone, and ethmoid bone
Level and view of
sectIons A and B
A Pnmitive pit
Primitive
node
Caudal
end
Cloacal
membrane
(future anus
Notochord
c
Caudal
end Primitive groov
Figure 4-1. Gascrulapon. The emhrynblast in the upper left-hJnd comer is provtJed for orimtation. (A)
Dorsal view of the epibla:.t. The primiuve streak consISts of me primitive gnxwe, node, and Plt. (8) Am)ws
how the mlgran n of cells rhrough the primItive TIle norochorJ (i.e., mesoderm located bc(wc '0 rhe
primitIve node anu the prochordal plate) induces the formati,m of the neural tube. The cardiogenic area is
rbe future heart. (e) Epiblast cells migrate t rhe primitive ,me<lk and insert rhernsdvcs berween the epiblast
anJ the hypoblast. Some epiblast cellsdi,place the hypohlast to (orm cndockrm; rhe r mailloer migrate cranially,
latemlly, and along the midline to foml mesodetm, After gastrulation, rhe 'plhlast is called ectcxlerm. (Modified
with permissIon from Fix JD and Dudek RW; D/t' Embryology, RalrmlOre, Williams & Wilkins, 199 ,r 30.)
1.0 Chapter 4
(9) )dol1LOblast
(10) Al)nicopulmonary seprum
(1.1) Parafollicular cells
(12) Dilaror sphincter pupilbe
(13) CJ1iary muscle
(14) Carotid body
2. Mesoderm
a. l'ard, iar (35 alI, of Slmite: and somiromeres)
(1) Skeletal muscles of rnmk
(2) Skeletal muscles of head and nCL.k
(3) Extraocular muscles
(4) Intrinsic muscles of the tongue
(5) and ribs
(6) eei ita] bont:
(7) Dem1ls
(8) Dura mCiter
b. lntennediatto
(1) KIdney'
(2) T and ovaries
(3) Genital uct. and accessory sex glands
c. Lateral
(1) Skeletal muscles llf the limhs
(2) Sternum, clavicle, scapub, pelvis, an the bones of the limbs
(3) Scrous membranes of j"xly cavities
(4) Lamina propria, muscularis mucosae, submucosa, muscularis cxtemac, anJ
advemitia of the gaslwinkstutallwll.
(5) 81\1 d cells, microglia, Kupffer cells
(6) ardlovascular system
(7) Lymphatic
(8) Spleen
(9) drem11 CQrtex
(.10) Laryngeal cartilage'
3. Endoderm
a. Epithelial lining of the auditory tube anu middle ear GWI!0'
b. Epithelial lining of rhe posterior ( f the Longue', tlour of the mouth,
palatoglossal and palatopharyn cal folds, soft p;:t1ale. of the palatine tonsil,
and, uhlingual and sub01anJibuhlr ghmds and ducts
c. Principal and oxyphil cells of the arathyroid glands
d. Epithelial reticular cells and thymic corpuscle'
e. ThyrOld follicular cells
f. Epithelial lining and glands of th trachea, lro .1Chi, and lungs
g. Epithelial lining of the gastrointesTinal tract
h. Hepall1cytes amI epirhelial lining of tht;' biliary tree
I. Acinar cells, islet cell., and :1e epit dial lining of t. e ancreatic ducts
J. Epithelial lining of the urinary I. IaLlcler
k. Epithelial lining of the vagina
I. Epithelial linmg of the fcmal urerhra and most of rJ:1e male urethra
Placenta, Amniotic Fluid,
a d Umbilical Cord
I. PLACENTA
A. Formation Figure 5-1)
1. Component"
a. Th maternal component of he plaeenm nnsises of eh decidua basalis, :J
porrion of the endometnum.
b. The fetal component (If th 'placenta 'on:,istJ, of lhe villous chorion.
2. Clinical correlations
a. Placental previa occurs when Lhe placenta atraches In the lower part of the
:-\11 lovers lhe internal os. Uterine blood vessels may rupture during eh
stage, 0 pregnancy, causing a potenl ially fatal hemorrhage in the
mother and placing the fetus U) jeopardy as 11 result of the compromised blood
supply.
b. Twinning (Figure 5,2)
(1) Monozygotic (identical) twins develop from one zygote.
(a) In 65% of cases, the have une lacenta, one Ch,)nnn, ;,nd
two amniotIC sacs.
(b) In the remaining 35(1'0 of cases, the fetuses have two placentas (sepa-
rate or fused), two chorion;;, and two amniotic sac-s.
(2) Dizygotic (fraternal) twins dey lop from tWO zygotes. The feruse have
twO placenr3.'i, two chortons, and two amniotic sacs.
B. Placental membrane (fetal-maternal barrier)
1. Layers
a. In early pregnancy, the placental membrane consists of the syncytiotropho,
blast, cytotrophoblast, connective tissue, and he endothelium of the fetal
capiJIaries.
b. In late pregnancy, the cytotrophoblast cells degenerate and the ec nnective
tissue is di.5placed by the growth of fetal blood vessels. !cav'ng the syncytiotro-
phoblast anu he fetal capillary endothelium.
2. Function. The placenral membrane separate marernal blood from fetal blood. Some
'ub ranees (both beneficial and harmful) cross the placental membtane freely,
whereas it is impermeable to others (Tables 5,1,5-2, and 5-3).
11
12 Chapter 5
Cytotrophoblastic shell
Intervillous space
A
I L Cytotrophoblast Chorion
L. Syncytiotrophoblast
Maternal blood vessels
Decidua basalis
Villous chorion
'\
Umbilical blood vessels
Placenta
Figure s,1. Placenta fonmwC1n. (A) Primary ch()riolllC villi fonn dunng w ek 2 when d1e cytorrop oblast
celb Invade th(' (B) Sccomlary chortlJnk villi form during week 3 when exrraemhryonic
mesodenn eV<lginar(''s into the cyl.()Irophoblasr. (C\ Tertiary Ch0rJOlliC illi f"rm when the umhlliclll hkJ<..d
vessel clevel,)!, in the extraembryoniL mesoderm. Tertiary chorionic villi collectively comprise me
chorion. The X 'nJic:llcs mmernal lood Within th, intervIllous 'Pace, and the (l'lT()tl.. indicates the layers that
must p<J5' through during fetal maternal hlc.ll)d c.elw.nge. In late pregnarlcy, the placental rnembrane
(feta1- materna] barrier) j, reduced [() two layers.
3. Clini.cal .'orrelaticl!1s. Erythroblastosis fetalis OCC'lr, l.'.'he-o fetal <:rythrocytes are
Rh-positive but the maternal erythrocytes :we Rh-negatIve. When the teral erythro-
cytes (fOS the placental m mhmnt' ,md eOCt:'r th. . matcmal circulation, the mother's
bo y fClfffiS antiRh antibodies that cross the placental membrane and destroy the
erythrocytes of the fetus.
II. AMNIOTIC FLUID
A. Production. Amniotic Huid i" produced by dialysis of maternal and fetal blood through
hlood veSl>cls in the placenta and by excretion of fcrnl urine into tl1e <'lmnlotlC sac.
B. Resorption. After being swallowed by the ferus, the ammatic fluid is absorbed into the
feral blooJsneam_ Excess amniotic fluid is removed by the placenta an:! passed into the
maternal blood.
C. Clinical correlations
1. Oligohydramnios occurs when amniotic flui is deficient (hs d1an 400 m! 10 late.
pregnancy) Oligohydramnios may he associated with the inability of the fetus to
excrete urine Into the amniotic sac as a result of renal agenesis.
A
1 Placenta
B
2 Chorions
2 Ammotic sacs
Placenta, Amniotic Fluid, and Umbilical Cord 13
2 Placentas
2 Anliliotic sacs
Agure 5-2. Arrangetn nr of rill' placenra, chofton, mJ 'lmltlOI ic "lC (,f (A) 65% ('( !non(lzyuol it. I'W111'
anJ (8) 35'16 o( n <lfhl-Y;':Olic twim ClI1J all [WillS.
Table 5-1
Ben.dlcwi Submmces Thelt Cross the Placcnt;:d Memhran'
Oxygen, carbon dioxide
Nutnents (e.g., glucose, amino acids, free fatty aCids, vitamins)
Electrolytes (e.g., sodium, potassium, chloride, calcium, phosphate)
Water
Fetal waste products (e.g., carbon dioxide, urea, uric acid, bilirubin)
Fetal and maternal erythrocyte
Maternal serum proteins
Steroid 110rmones
Immunoglobulin G (lgG)
Table 5-2
I [armful That Cross the Placental Merubrcme
Carbon monoxide
Viruses {e.g.. HIV, cytomegalovirus, rubel/a, Coxsackie, variola, varicella, measles, poliomyelitis}
TrepOflel7l8 palladium, Toxoplasm- gOfldli
Drugs (e.g., oeaine, alcohol, caffeine, nicotine, warfann, trimethadione, phenytoin, cancer hemothera-
peutic agents, anesthetics, sedatives, analgesIcs)
AntiRh antibodies
HIV = human Immunodeficiency virus.
14 Chapter 5
Table S-3
() Nor Cross the PIClcental Membr<.lI1c
Maternally-derived cholesterol. triglycerides, and phospholipid
Protein hormones (e.g., insulin)
Immunoglobulin M (lgM
Succinylcholine, curare, heparin. drugs similar to amino acids (e.g., methyldopa)
Most bacteria
Inferior vena cava ---I
Left umbilical vein -----..
(t 02)
Right and left umbilical arteries
(.j.2)
hunts:
A---- Ductus arteriosus
.----'\+t--- Foramen ovale
,-----jf--.---t--- Ductus e osus
Figure 5-3. foetal clrculation.
Placenta, Amniotic Fluid. and Umbilical Cord 15
............ , .
2. Polyhydramnios occur when amniOTic fluid are high (more than 2000 ml in
late pregnancy). TIllS condiTion may be aS50ciat<:J with anencephaly or esophageal
atresia.
3. a-Fetoprotein (AFP) assay is used to diagnose neural tube defects (e.g., spina bifiua,
.mencerha/y). ,p is found in a111 niori.. (luid !lnd maternal serum.
III. UMBILICAL CORD. The [dinitive umbiliCdl cord contains the right and left umhilical
arteries, the k t umbilical vein, and mucous connective tissue.
A. The umbiJ.cal arteries carry deoxygenated blood from the fetus to the placenta.
B. The lefr rnbilical vein carries oxygenated blood from the placenta to the fetus.
C. Clinical on:elations
1.. previa when the umbilical blood vessels cross the internal os of the
utems, preul posing them to mpture. Rupture of the umbilical hbod ve:;sels durin.g
pregnancy. lahor, or delivery can cau e the fetus 0 bleed TO death.
2. Presence of 00(' II00hilicai artery. 0Prosed to (Wo, ."Ilgges!. the presence of
cardiovascular
IV. ANGIOGENESIS AND HEMATOPOIESIS. Me odenn differentiates into angioblasts,
whlch foml angiogenic cdl clusters.
A. Angiogenesis. Angioblast.' around the periphery of the angiogenic cell clusrers give flS
to the endothelium of blood vessels. Angiogenesis occur: initially in extraembryonic
visceral mesoderm (located around tIte yllik sac), and later in the mcwdenn of the
fetus.
B. Hematopoiesis. Angioblas within the ccmer of the angiogenic cell clusters give rist';
to blood cells. Hematopoiesis occurs i itially in the extraembryonic visceral mesoderm
(located around tbe yolk "ac) and later in the fetal liver, spleen, thymlls, cHld bo e
marrow.
V. FETAL CIRCULATION II1V Ives rhree shunt. : the ductus venosus, ductus arteriosus. an,1
foramen ovale (Figure 5-3). A number of changes occur in the neonatal circulatlon when
ph cnral blooo flow and lung respiration begin. Table 5-4 summarize tht: remnants
rhar resulr (rom clo lire of the fernl stmcrures.
Table 54
Remnants Created by Closure of Fetal Circulalory Structures
Fetal Structure
Right and left umbilical arteries
Left umbilical vein
Ductus venosus
Ductus arteriosus
Foramen ovale
Adult,Remnant
Medial umbilical ligaments
Ligamentum teres
Ligamentum venosum
Ligamentum arteriosum
Fossa ovale
16
6
Cardiovascular System
I. DEVELOPMENT OF THE HEART
A. Primitive heart tu c. A pair 01 endocardial heart tubes (meso erolal in origin) {aon
within the carJiogcnic region.
1. lateral folding occurs, the hearr tubes fuse to form [he primitive
heart tube, which develops II1tn the endocardium.
2. Mesoderm surr(lllO<. ing rhe primII ivc flC::m tube develops into t .e myocardium and
epicardium.
3. Tlw primitive heart rube (orms five dilatations (Figure 6-1), the fates of which are
Jet.likJ in Tahle 6-1.
B. Aorticopulmonary (AP) septum. The AP septum divides the truncus arteriosus I11W
I he aorta ;)nd pulmonary trunk.
1. Formation (Figure 6-2). Neural cre r cell migrate inr the truncal an bulbar
ridges, whicn grow and twist around each nrher in Cl .piral fashion. fu. ing ro form
the AP septum.
2. Clinical con-elations
a. Traospusition of the great vessels (II-ems when the AP sepwn fail t develop
in a spiT<.;! fashion, caUSIng the aorra t- open intu be ri.ght enmclt, and che
pulmonruy rrunk LO open inlU he left vemttde. The resu1ranr right-to-Ieft
shunting f blood lead to cyano:.is.
b. Tetralogy of FaUot (Figure 6-3) o<-cur:, when the AP septum fails to align prop-
erly with the atrioventricular SL'ptum and results in pulmonary stenosis, overrid-
ing aorta, interventricular septal defect, rind right ventrkular hypertro fly.
Tetralogy of Failor is ch:lract-enzed by right-to-Ieft shunting of blood and cya-
nosis.
C. Atrioventricular (AV) septum. The AV septum p;mitions the AV canal intn the right
AV canal and left AV canal. Th.e dorsal and venwd AV cushion:- fi.15e to form the
AV septum (FIgure 6-4).
D. Atrial septum
1. Formation (Figure 6-5)
a. The septum primum grows toward the AV septum.
b. The foramen pdmum tS localed between Lhe edge {the septum primum ,mJ
Cardiovascular System 17
the AV septum; it is nbliterall: when the septum primum (uses with the AV
septum.
C. The foramen secundum forms in the center uf the septum primum.
d. The septum secundum forms to the right of the m pnmum and fI.lses (after
birth) With the 'eprum primUln to form the atrial sept.um.
e. The foramen ovale is the 0 cning between the up t'r dnd lower pans of the
septum ndum.
(i) During fetal life, hlood from the ri hl ::ltriurn to the left atrium
Vta the ioramcn v81e.
(2) elosun of the foramen ova1e normally t: kes pia soon after birth and
Agure 6-1. TI1C ft e ditatallnm llf the heart tube. A. = pr1lnlllve atrium; B = bulbw. cordts, SV = sinus
venOSLl ; T = truncus artenOSlIs; V = primitive ventricle; while area = arterial pCltCIon; shaded are.a - venous
portion. (Modified with permISSion (rom Fix JD and Dudek RW: BRS Embryulogy, Baltimure, Williams &
Wilkms, 1995, p 40.)
Table 6-1
Derived From the Em ryonic Dilatations
of tbe Primitive Heart Tube
Em ryonic Dilatation
Truncus arteriosus
Bulbus cordis
Primitive ventricle
Primitive atrium
Sinus venosus
Adult Structure
Aorta
Pulmonary trunk
Smooth part of right ventricle (conus arteriosus)
Smooth part of left ventricle (aortic vestibule)
Trabeculated part of right ventricle
Trabeculated part of left ventricle
Trabeculated part of right atrium
Trabeculated part of left atrium
Smooth part of right atrium (sinus venarum)*
oronary sinus
Oblique vein of left atrium
a) The smooth part of the left atrium is formed by incorporation of parts of the pulmonary
veins into the atrial wall.
b) The junction of the trabeculated and smooth parts of the right atrium is called the crista
term/nails.
18 Chapter 6
Truncal
ridge
Bulbar
ridge
Agure 6-2. Formarion. of the <lornwpulnhlllary (AP) <'plum. = hulbUl' cordIS; T = rnmcUl' arterio us.
wlh P'l"mlssion from Ex JD and Dudek RW: 5R. F:mbryology. J3almnore, Wilk-lms & Witkin>.,
199 , p 4J )
Pulmonary
stenosis
Richt ventriCUlar
hypertrophy
Overriding aorta
- interventricular
septal defect
Figure 6-3. The (our m;Jin defect' with rt'traiogy <If F"lIot. (Morhfled wIth permISSIon fTo 1m Fi"
J() and Dudl'k RW: BRS Emhrynlogy, Balmuore, Wlllmms' Wilkins, 1995, r 44.)
is facilitated by the increased left atrial pressure that results (n.m) changes
in the pulmonary crn:ulation.
2. Clinical correlations. Foramen secundum defect is caused by excessive cesorption
of the septum primum <)J' secundum and results in ,J patent foramen ovale.
E. Interventricular (IV) septum (Figure 66)
1. Fonnation
a. The muscular IV septum develops in t.he fluor uf the. vel1lride an' grows toward
t.he AV sc tum, stopping short to cre::tte the IV foramen.
Cardiovascular System 19
A Ventral AV
cushion
SingleAV
canal
Dorsa AV
cushion
B c
AV septum
Right AV canal Left AV canal
Figure 6-4. Formauon of the amnv nrricuJar (AV) septum. A = (ltrium; \i = vennide. (R primed wIth
pennission from Fix JD and Dudek RW: 81\5 Embryology, Baltimore, Williams & Wdkins. 1995, p 42.)
Septum primum Septum prlmum Foramen secundum
B
primum
Foramen
pcimum
primum
Foramen secundum Septum secundum
Right
atrium
Foramen ovale
secundum
Left atrium
D E F
Agure 6-5. mffiation of the atrial sepWffi. The arrows in F indicate rhe dj,,::crion of bloo flow across
the fully developed septum. from the nght atrium to the lefl atrium. (ModIfied with from Johnson
KE: NMS Human Develupmental Anatomy, Baltimore, Williams & Wilkins, 1988, p 149.)
20 Chapter 6
Membranous
IV septum
Agure 6-6. The lnterventncular (IV) SCpWIlI. a ;0 right bulbar rid I ; b ;0 left bulbarridge; c = atrioventriC-
ular (AV) sepnlm. (Modlfied with permiSSion from FLx )0 and Dudek RW: BRS Embryology, Baltimore, Wil
Iiams Wilkins, 1995, p 43.)
Table 6-2
Devdopment of the Arterial System
Embryonic Structure
Aortic arches
1
2
3
4
5
6
Dorsal aorta
Posterolateral
branches
Lateral branches
Ventral branches
Vitelline arteries
Umbilical arteries
Adult Structure
*
*
Right and left common carotid arteries
Proximal right and left Internal carotid artenes
Proximal right subclavian artery
Part of the aortic arch
**
Proximal right and left pUlmonary arteries; the ductus arteriosus
Ductus arteriosus
Intercostal, lumbar. lateral sacral, median sacral. vertebral. deep cervical,
ascending cervical, Internal thoracic, superior and Inferior epigastric arter-
ies, and arteries to the upper and lower extremities
Renal, suprarenal, and gonadal arterie
Celiac, uperior mesenteric, and inferior mesenteric arteries
Part of the internal iliac arteries, superior vesical arteries, and medial umbili
cal ligaments
* Minimal contribution in the adult.
U Aortic arch 5 degenerates in humans.
Cardiovascular System 21
Table 6-3
Development of rhe VenoLis System
Embryonic
Structure
VitellIne veins
Right
Left
Umbilical veins
Right
left
Cardinal veins
Anterior cardinal
Posterior cardinal
Subcardinal
Supracardlnal
Adult Structure
Hepatic veins and sinusoids, ductus venosus, paft of the IVe, and portal,
superior mesenteric, inferior mesenteric, splenic veins
Hepatic veins an slnusoids, ductus venosus
Degenerates
Ligamentum teres
Internal Jugular veins, sve
Part of IVe, common iliac veins
Paft of IVe, renal veins, gonadal veins
Paft of lye, intercostal vein ,hemiazygos vein, azygos vein
IVC = inferior vena cava; SVC supeno vena cava.
b. The membranous IV septum forms following fusion of the and left bulbar
ridges anJ the AV septum. The membranoLis IV septum closes the 1V foramen.
2. Clinical correlations. Membranous ventricular septal defect (VSD) is caUSed by
failure n( I he membranous V septum to develop, resulting in I>h unting
of blood th.rough t e IV foramen. Left-to-right shunting of blood increases blooU
Row to the lungs, resulting in pulmonary hypertension. Patients with lefroto-right
shunting cnmrl"in of excessive on 'xert ion.
II. DEVELOPMENT OF THE ARTERIAL SYSTEM
A. Formation. The arterial sybtem Jevdops [Tum the aortic arches an branches d" The
dorsal aorta (Table 6-2).
B. Clinical correlations
1. Postductal coarctation of the aorta occurs when the aorta is abmlMnally constricted
just inferiur to the ductus artenoSllS. ThLS condition IS 11Ilically associated with
increased blood pressure ill the upper exm:milies, lack of a femoral arterial pulse,
and a high isk of cerebral hcmonhagc anJ bacrerial ndocarditis.
2. Patent ductus arteriosus (PDA) occurs when the ductu arteriosus fails to close
after birth.
a. Normally, the ductus arteriosus doses within a few hours via smooth musdt:
contraction, forming the ligamentum arteriosum.
b. rDA is common in premature infants ami those born to motheTh infected wid
rhe rubella virus dUring the course of their pref:,'11anc)'.
III. DEVELOPMENT OF THE VENOUS SYSTEM. The venous system develops from the
vitelline, umbilical, an cardinal veins (Table 6-3). .
7
Gastrointestinal System
I. PRIMITIVE GUT TUBE. The primitive gut tube is divided into the foregut, midgut, and
hindgut (Figure 7-1).
A. formation. rhe l'rimitive gUl ttne i rt.lmleJ by the incorporation of the yolk sac into
LIt!.: embryo Juring craniocauJal and folding of the emhryo,
1. The epithcliallining and glands of the gut tube mucosa are derived from endoderm,
whereas the lamina propria, muscularis mucosae, submucosa, muscularis externa,
and or serosa are derived from mesoderm.
2. The eptlheliallining of the tit tube proliicralC-'> rapiJI and obliterates the lumen.
Canalization then occurs.
B. Foregut derivatives arc supplied by 1e celiac artery.
1. Esophagus
a. Formation. The tracheoesophageal septum divides the foregut imo me 'sopha-
and trachea.
b. Clinical correlations. hageal atresia occurs when tile esophagus ends as
a blind rube as a result of malfoffilation of the tracheoesophageal septum,
2. Stomach
a. Formation. The. tomach develops from a fusiform dilatatton thal forms in the
foregut during week 4. The primitive st,)mach wt::J.tes 90 lockwisl" during its
fomlation, causing the (ormation of t e lesser peritoneal sac,
b. Clinical correlations. Hypertrophic pyloric stenosis occurs when the museu-
bris externa hypertrophies, na1T0wing the pyloric lumen. This condition is asso-
ciated with projectiic vomiting ,md a small, palpable mass at the right costal
margin.
3. Liver
a. An endoderm;)1 olltg1'Owth of the foregut (the hepatic diverticulum forms in
the surrounding me$odcrm (Le., the septum transverswn). (The septum
transvetsu also plays OJ role in the formation of the diaphrdgm, which explains
the proximity of the liver and diaphragm in adutrs.)
b. The hepatiC diverticulum send. hepatic cell cords into the septum transversum.
The hepatic cell cord surround the vitelline 'ems, which tom1 hepatic siuu-
soids.
4. Gallbladder aud bile ducts
a. Formation. The conneclion between the hepatic diverticulum and foregut nar-
rows to form the bile dUCL Later, an outgrowth from the btle duct gives rise to
the gallbbdder and cystic duct,
GastrOIntestinal System 23
Foregut
Hindgut
Midgut
, tomach
----/---- tnferior
mesenteric
artery
Esophagus
()
Cecal bud ---\- Superior
:. mesenteric
artery
Atlantois
Cloaca --+---I-f-
Ventral pancreatic bud
Yolk sac
(vitelline duct)
t
Urogenital sinus
Perineal body ----\
-- -..".
Lower anal canal
Agure 71. Development of the "astrotntesiinal tract showmg th" foregut, midgut, aml hmdgul. The
morecm partitions the clnota into ,he upper anal c:m;ll rmd the urogenlwl 5! (boxed llrea), The
curved llTTuW IndIcates the Jirectlnn ()f growth of thE' uwn:cral ,'cptum towmd the buJy ,urtace, It
at tlle perineal body. TIl' ectoderm invugm3tes, formll1g the proctodeum, an' meers the tipper an:tl carlal at
the pectinate line 10 f,lrm ule lower <lnal canal..
24 Chapter 7
b. Clinical considerations. Extrahepatic biliary atresia occurs whcn incnmplete
camdiz<-1l1on LO olclusion of [he hillary dUCI lumina, This condinon is
:lssociated with j<lUnJlcc, pale feces, ,md dark Lnne
5. Pancreas
a. Formation
(1) The ventral pancreatic bud the uncJni'lte p . and parr of the
he:Jci of the pancreas.
(2) Th.e dorsal pancreatic bud f(lrmS the remainlltg part of rhe head. body,
and ratl uf the pancreas.
b. Clinical correlations. Annular occurs whe the ventra and dorsi'll
pancreatic bud' form a ring around the dU(ldenurn, thereby ubstructing It
6. Upper duodenum. The cranial portion of the duodenum devc1n s (rom the cau al
porrinn. (1( the foregut. The Junction of the foregut and midgut is jllSl distal to the
opening of tbl: common bile duct.
C. Midgut derivatives'lr suppli,'d hy t1w superior MIt'')'.
1.. Lower duodenum
a. Formation. The lower Juooenum originates from the cmmal pClrtion of the
midguL.
b. Clinical correlation!>. Duodeffill atresia occurs when t .c lumen of the duode-
num is occluded as a of failed recanalizalwn. Th[:; condition is
with potyhydramnio', bite-cont<lining omiws, and Jistent ion of the stomach.
2. Jejunum, ileum. cecum, appendix, ascending colon, and the prox.imal two-thirds
of the transverse colon
a. Form;)tion
(1) The midgulloop herniates through the umbilicus dunng a known
physiologic umbilical herniation.
(a) The cranial limb of the midgut loop forms lhe jejunum and cranial
portion of the ileum.
(b) ll,c cauJallimb fonns the cecum, appendix, caudal portion of the
ileum, ascending c l)on. 8J.1d proximal two-thirds ()f the transverse
colon.
(2) The midgtLt !O<.lp rotate,,; 270
0
counterclockwise arounJ the superior mes-
entetic arlt>ry :IS il r<>,tllms m the abdom;n:11 (,wiry, feducing the physiologic
herruatlO[l.
b. Clinical correlations
(1.) Omphalocoele >ccurs when the midgur loop fails to return to the
cavity. In the newborn, n ILght gray, hiny sac is visihle at tht' base of
the umbilical cord.
(2) UcaJ diverticulum occurs when a remnanl L)f the yolk sac (or
viteUine dun) ersists, forming an opening between the lumen of the
ileum and the umbilicus. This conditi.on is associated with drajnage of
meconium from the umhiliclls.
(3) Malrotation of the midgut OCCLmi when the midgut undergoes only partial
rotatior, rcsultm in abnormal positioning of the' abdominal viscera. This
condition may be associated with olvulm;.
(4) Intestinal atresia or stenosis oc ur:s as a result of f(lilecl recanal ization.
D. Hindgut Jerivatives (i.e., lhe distal third of the transverse colon, descending colon,
sigmoid colon, and upper anal canal) are supplieJ by the inferior mesenteric
artery.
Embryonic
Mesentery
Ventral
Dorsal
Gastrointestinal System 25
Table
Derivation of Adulr Mesenteries
Adult Mesentery
Lesser omentum (hepatoduodenal and hepatogastric ligaments), falciform ligament,
coronary ligament. triangular ligament
Greater omentum (gastrorenal. gastrosplenic, gastrocolic, and splenorenalligaments).
mesentery of small intestine, mesoappendix, transverse mesocolon, sigmoid meso
colon
Formation
a. The cranial end of the hindget fonm the distal third of the transverse colao,
the descending colon, anti the sigmoid colon.
b. The terminal tnJ of the hmJgut (the cloaca) IS partitioned by th uroreclal
tnn. rhe pper aoal ca"nal and rhe urogenit<11 sinus (Sl:C Flgun: .1)
2. Clinical correlations
a. Colonic aganglionosis (Hirschsprung's disease) resulrs from bilure of neura
"rest cells to fonn the mycmcric In the sigmoid coic'n and rectum. This
ondition is associated with loss of peristalsis. fecal retemion, and abdominal
distenrion.
b. Anorectal agen.esis occurs vhen the rectun end, as a hlind .. c above the puho-
rcctalis muscle f abnormal formation of the urorecral septum. Thb
condition may be accompanied by a rectovesical fistula, rcctourethral fistula,
or rectovaginal fistula.
c. Anal agenesis .ccurs when r!w 8nal canal ends a, a blind ,ac below the rub<,rec-
calis muscle ;1S a r suit of abnormal farmatlo) of the urorectal septum. This
CClnJition may be accompanied by a rcctovcskal fistula, rcctourethral fistula,
or rectovaginal fistula.
II. PROCTODEUM. The lower anal canal develops fwm an invagm:l("ion of surface ectoderm
called th" proctodeum (see Figure 71).
III. MESENTERIES. The primitive gtH wbe lS suspended withIn the reritoneal caviry of tne
embryo by the ventral and dorsal from whidl all adult mesenterie, are derived
(Table -1).
Respiratory System
I. UPPER RESPIRATORY SYSTEM. The IIpper respiratory system 's dIscussed m. Chap-
ter 9.
II. LOWER RESPIRATORY SYSTEM. The trachea, bronchi. and lungs compnse tht:: lower
re-piratory system.
A. Formation (Figure 8-1)
1. The laryngotracheal diverticulum forms .n rhe ermal wRll of the foregut.
2. TIll; tracheoesophageal septum uivides the fc.'r gut n t ~ the esophagus and rrachea.
3. The distal end of the laryn otrachcal diverticulum enlarges to form the lung bud.
Esophagus
Tracheoesophageal
septum
Trachea ~ ~ ~
5 Weeks
Visceral
mesoderm
ronchla! buds
~ ~ ~ Esophagus
4 Weeks
Laryngotracheal
diverticulum
6 Weeks
Figure 8-1. Development of the res irawry system. (Modified with permission from Johnson ICE: NMS
Human [eveloplTU.'nr Anatomy, Baltimore, WIlliams & Wilkins, 1988, p 228.)
26
Respiratory System 27
Table 8-1
StClges of Lung Devdnpmenr
Name Time Period Characteristics
Glandular
Canalicular
Terminal Sac
Alveolar
Weeks 5-17
Weeks 13-25
Weeks 24-birth
Birth-year 8
Respiration is not possible
Premature fetuses cannot survive
Respiratory bronchioles and terminal sacs form
VascularizatIOn increase
Premature fetuses born before week 20 rarely survive
Typ I and Type II pneumocytes are present
Respiration is possible
Premature fetuses born between weeks 25 and 28 can
survive with Intensive ,are
Respiratory bronchioles, terminal sacs, alveolar ducts,
an alveoli increase in number
4. TILl: lung bud dlviJes inro rwo bronchial buds, which branch into the primary,
secondary, and tertiary bronchi. The tertiary bronchI are related to the bronchopul-
monary segments in the adult lung.
B. Stages of development. The lungs undergo four stages of leve!opment ( able 8,]).
C. Clinical correlations
1. Tracheoesophageal fistula. 1\ tr:Jcheoes,'phageal Fistu a is an abnonnal cornmunlca-
tlon berw 'en the trachea and esophagus caused hy a malformation of til( tr,!C co-
esophageal sc tum. This condltion resulls in gagging and cyanosis afrer feedmg,
abel lTIln<:11 dlstemlorJ after ct}in
l
, ,mJ reflux of uw gastric contents inm th lun ,,.
2. Respiratory distress syndrome is causeJ by (1 deficiency ofsurfanant. TIlis condition
IS most common in pH'mature infants, those bom to diabetic mothers, an those
experiencing prolonged intrauterine asphy'\ia. Treat men, with thyroxme and corti-
sol can increase the pwduction of surfactant.
3. Pulmonary hypoplasia occurs when lung evelupment stunted Congenital dia-
phragmatic hernia (hernlatieJn of rhe abdominal contents imo the thorax leads \.ll
corn )rcssioll rA the lung) and bilalcral rena) agenesis
the pressure on the fetal thorax) arc pre.disposing factors.
9
Head and Neck
I. PHARYNGEAL APPARATUS (Figure 9-1 . The pharyngenl appar2tus consists of th
p[,;:tryngf"lI ;Itches, pouches, grooves, anJ membranes.
A. The pharyngeal arches (1 2,1,4,0)" arc cnmpnscu of mesoderm and neural crest Cl,!1S.
EdCh arch has a cranial nerve as;oClatcd with it. Table 9-1 summarIZes the adult deriva-
tives of the pharyngc..d arches.
B. Th pharyngeal pouches (1,2,3,4) are evaginations of the endoderm-lined foregut
Table 9-2 summarIZes the adult derivatives of the pharyngeal pouches.
C. The pharyngeal grooves (1,2,3,4) :m, inqginarions of surfilce e toderm.
1. Pharyngeal groove 1 gives risc to dw epithelial lining of the external auditory
meatus.
2. All l)f the other grooves are obliterated.
D. The pharyngeal membranes 0,2,3,4) are located at the junctinn of each pharvnge<l
groove and pouch.
1. Pharyngeal membrane 1 gives rise to lhe tympanic membrane.
2. All uf the other memhranes are obliterate .
II. THYROID GLAND. The thyroid gland develops from the thyroid diverticulum, whICh
fonns In lhe Hoor of the foregut. The thyroid diverticulum caudally to Its adult
anatomical position ut remains connected to the foregut via the thyroglossal duct, which
is later obliterated. The former site of the thyroglussal Juct is indICated In the adult by the
foramen cecum (see Figure 9-18).
III. TONGUE
A. The anterior two-thirds of lhe tongue fl)rm from the median tongue bud and two distal
tongue buds associated with pharyngeal arch 1.
Plulryngeal arch 5 degenerates in humans
28
Head and Neck 29
Auditory tube and
middle ear cavity
External
auditory meatus
(pharyngeal groove
Tympanic membrane
(pharyngeal membrane 1)
B
Foramen
cecum
Figure 9-1. (A) Overview of rhe pharyngeal app,u-,Itus. (B) Mlgrarion of the erior anJ inferiOI p<)r;)rhyrold
glnnds (Sr, IP), rhymu, (T), ultimobranchIaI body (UB), and thyroid gland. TIle foramen cecum cvagmares
ro form the 1hyrOlJ Jl eniculum, which migrares along rhe midlme (Jolted an-ow). In addlriou. pharyngeal
pouch I, pharYI\gefll membrane I, and pharyngtool groove I are ,hown. These structures give risc to stnJl;IUre'.
of the adult ear. 2 = pharyngeal pOlich 2; 3 = pharyngeal pouch 3; 4 = ph:Uyngc,11 pouch 4.
1. GenlO'ml I" carrieJ by cill' lingual. branch of eN v,
2. Taste sensation Ls canied hy the chorda tympani branch of CN Vll.
B. The posterior one-third of tht.' tonguIO' forms predominately frum Lhc hypobranchial
eminence associated With pharyngeal arches 3 and 4. Uenerat and taSle are
LaITleJ by eN IX,
C. The intrinsic muscles and the styloglossus. hyoglossus. and genioglossus (exrrinsic)
muscles are derived from myoblllsU> that migrate to the tongue region from occipital
MOWf llmervatkm by CN XII, excepl for, rhat of the pa awgloSl>us
muscle, hich IS inn Tvat.ed by CN X.
IV. PALATE (Figure 92)
A. The intermaxillary segment (orms whe the two medial nasal promLtlences fuse together
at the midline. The intermaxtllary segment gi es rise to the philtrum of the lip, four
incisor teeth. and primary palate of the adult
30 Chapter 9
Table 9-1
Adulr Derivatives of rhe Pharyngeal! rches
Adult Derivatives
Arch Nerve Mesoderm Neural Crest Cells
2 CN VII
3 eN IX
1 NY
4
6
eN x(superior
laryngeal
branch)
CN X
(recurrent
aryngeal
branch)
Muscles of mastication, mylohyoid
muscle, tensor eli palatini
muscle, tensor tympani muscle,
anterior belly of the digastric
muscle
Muscles of facial expression,
posterior belly of the digastric
muscle, stylohyoid muscle,
stapedius muscle
Stylop'1aryngeus muscle
Muscles of the soft palate (except
tensor veli palatini), muscles of
the pharynx (except
tylopharyngeus). cricothyroid
muscle, cricopharyngeu5
muscle, laryngeal cartilages
Intrinsic muscles of the larynx
(except cricothyroid). upper
muscles of esophagus,
laryngeal cartilages
Maxilla. zygomatic bone, temporal
bone, palatine bone, vomer,
mandible, incus. malleus.
sphenomandibular ligament
_esser horn and upper body of
hyoid bone, stapes, styloid
process, stylohyoid ligament
Greater horn and lower body of
hyoid bone
Pouch
1
2
3
4
Table 9-2
Adult c r i v t i v c ~ of the Pharyngeal Pouches
Adult Derivatives
Epithelial lining of auditory tube and middle ear cavity
Epithelial lining of palatine tonsil crypts
Inferior parathyroid gland, ttlymus
Superior parathyroid gland, ultimobranc ial body*
*' eural crest cells migrate Into the ultlmobranchial body to form the parafolilcular
cells of the thyroid.
B. The secumlary palate forms from outgrowths of the maxillary prominences called pala-
tine shelves. ThDC palatine shelves fuse at the midline.
C. The definitive palate is forme {ollowing fusIOn of the primary and sl.:conJary palates
at the incisive foramen.
V. CLINICAL CORRELATIONS
A. A pharyngeal fistula occurs when pouch 2 and groove 2 persist. The fistula is enerall)T
found along the anterior horJer )f the sternocleidomastOid muscle.
B. A pharyngeal cyst occurs w en pharyngeal grooves thaI ar . normally obliterated persist.
The cyst is usually located at the angle of the mandible.
Maxillary prominence
A
Intermaxillary segment
B
........ .......-
Nasal septum
Head and Neck 3:1.
,------1- Fused medial
lasal prominences
(intermaxillary segment
Level of sections Aand B
c
Nasal septum
I
ongue
Figure 9-2. nf The pllbte. (A,B) 10" \'cnrr;ll vlcw with the lowcr jaw end tongue rel1loved
show' the intermaxdlnry ",glllCnl "nd ,heh ('5 Clrr.:t) fusing <'It the ((lIdline (am)tl'I). (C)
The /romal view .,I,uw5 the p,tlatll1e shelvc:, (crosshatched ar ) u,mg i\( the the nasal scptum
(amlu'5).
C. First arch syndrome, hich is c.h3t<lCr .rized 'i factal. anomalies. ,Kcur' when faulty
migration f neural crest cells cause, ahnormal fnrmation of pharyngeal arch 1.
Two well described syndr me:; are Treache CoHin' syndrome and Pierre R\lbio
syndrome.
D. DiGeorge syndt:'ome occurs when phClryngcal rOllches 3 and 4 faillo differentiate mto
the parathyrOId glands and d ymus.
E. Ectopic thyrQid, parathyroid, nt thYOlm [1'';111 r<; from abnormal migrmion of l gland.
irom their embryoniC pnsi[il1o [() [heir "dulr ilnatomica posicion.
F. A thyroglossal duct cyst llCCltf5 when p:lm of the thyroglo.<;sil Juel generally
at th miJlme near the hyoitl bone. The cys may alsn be fOllnd at t11", hClse of 1h
wngllc (lingual cyst).
G. Cleft palate occur.- whcn the po!'Jtu'le shelvl:s fail to fuse with each lIther or the prirnaly
palate.
32 Chapler 9
H. Cleft Ii oeellf) whcn (h maxillary prommence fill15 tu fusc wil the medial nasal
prommence. lett pabt anJ cleft lip are Jistinn malformations, although they often
O(CUf toge he .
I. Ankyloglo3sia occur leo the mogul' lS no freed from rhe fluur l f the mouth. Mosl
c0mmonly, r e frenulum exrenill; () the fir of the rongue.
J. kramaJ OlenlOl{ocele) whcn r, I ti"sue. Jr bt.>lh her-
nlrlte 1 hrnugh defects in the _kulJ.
K. Cranim.ynostosis occurs as J n:sult of premature e1oStln: of one or more sutures of the
"kull.
1
Urinary System
J. OVERVIEW. intermediate mesoclf'rm forms a longitudmal elevation along t e (orsal body
wall, cClUed me urogenital ridge (Figure 10-1). A portion of the urogeniwl ridge, the nephro-
genic cord. forms he and metanephros.
A. Th' pronephros completely regresses.
B. The mesonephros forms the mesonephric (wolffian) duct.
C. The m tanephros develops fmm the ureteric bud, an flutb'T(Jwth of mesonephrIc
duct, and metanephric mesoderm (Table I -1 . The metClnernros eventually becomes
the definitive adult kidney.
1. The pcnnanent honey ascends during de e1upmenr from the sacral region to its
adult anatOlTIlcal Jm:allon at Tl2-L3 (figure 10-2). -
2. Embryonic arteries formed during Ule may persist as supcmumerary arteries
In the adult. These arteries :Ire end arteries; therefore damage to the vessels will
result in damage t<. rh tissues hey .,uprly.
Intermediate
mesoderm
Nephrogenic
cord .A"i:sS!crlJ1I:rh...
-.38l..--- Neural tube
J--H'of-- Gut tube
Figure 10-1. FOTTn<Jtion of rht: nephrngc1'\Ic cllfd as the t:mbryo goes through LrJnioc<tuJal and lateral
folding.
33
34 Chapter 10
Table :1.0-1.
Develupment of rhe Kidneys
Embryonic Structure
Ureteric bud
Metanephric mesoderm
Allantois
Adult Derivative
Collecting duct
Minor calyces
Major calyces
Renal pelvi
Ureter
Renal glomerulus (capillaries)
Ronal (Bowman's) capsule
Proximal convoluted tubule
Proximal traight tUbUle}
Descending thin 11mb Loa
Ascending tllin limb
Distal straight tubule
Disti'll convoluted tubule
Connecting tubule (eT)
Hindgut
./
of Henle
---1--- Mesonephric
duct
: j ~ Metanephric
mesoderm
Uretenc bud
FIgure 10-2. Fonnarion of e pem1ancnt ktJney and unonry bladder. The arrow IOdicates the ascent of
[he kidney.
Unnary System 35
II. SUPRARENAL GLAND
A. he cortex form.s as a result of two episoJes of mesoderm proliferation.
1. The fir,l episode form I he fetal cortex, whi.ch regresses by the second r
month
2. Th cond episode forms the adult cortex (l.e.. the zona zona fuSCICU-
lala. and zona reticularis).
B. The medulla forms from neural crest cdls, which migrate to the fetal cortex: and differ-
entiate into chromaffin cells.
III. URINARY BLADDER. The urinary bladder develop> from the upper end of the urogenital
sinus, whicb is continuous with the allantois.
A. The allantois anu fomls a fibrous cord in the <\Jult called the urachus
(median umbilical ligament).
B. The trigone of the bladd r i' iormed by e incorporation of d1e lower en,l of the
mesonephric ducto into the posterior wall of the nus.
IV. CLINICAL CORRELATIONS
A. Renal agenesis )CCtm when the meteric bud fails to develop.
B. Horseshoe kidney ccurs when the inferior pole of both kidney fuse. During the
ascent, lhe kidney gets uapped behind the infcriLJr ffiCl>enteric artery.
C. Ncphroblastoma (Wilm's tumor) is ;;I common malignant tumor found in chJldren.
The neoplasm probably arises from embryonic nephrogenic tissue.
D. Urachal cyst (sinus) occurs when a remnant of lhe llllantois persists. This conJiliQO
i. associated with urine Jrainage from the
E. Pheochromocytoma is a chromaffin cell rumor. Phcllchromocywmas are generally founJ
along the migratory path of neurall-rest cells (e.g., rn the (et8l cortex).
36
11
Reproductive System
I. INDIFFERENT EMBRYO (Figure 11-1). Allhough the gcnNype of the embryo is estab-
lished Cll fertilization, fem, Ie and nlllie embryos are phcnotypicall'\'> rnd' 'n ishable helween
w k OJ 6,
A. By H:.:k 12 '001' felOale <Uld male c.haraCteTlSrlcs of the external genitalia Cln be
recognized.
B. By cck 20, phmotypi ' 'Crenti-a i n is compl e, The component., (the mel if(erenr
embryo that arc remodeled to f,mn the adult female ;toe! male reproduclive systems are
the gonalk, paramesonephric (miiUerian) uctl', mesonephric (wolffia) ets and
Jubules, urogenital sinUi', ph.lllus, urogenital f Ids. and labioscrotal swellings (Tabk
11-1).
II. DESCENT OF THE OVARIES AND TESTES. The and lestes develop within
the abdolllinalca ' y but later descend i to the elvlS an 'crOlUn+, respectively, The guber-
nacul (a band of fibrous tisue) and the prqcessUl> vaginaLi' (an evagination of perito-
neum) are involved in the Jescem n( buth r e ovaries and teste', The fates of the gubernilcu-
lum and vflginalis are summarized in Tahle- 11-2
III. CLINICAL CORRELATIONS
A. female occlIr;:. whl>n 0\ ilri(ln tissue if it u person With a
normal fcrnale karyotype (46, " but the eXlemalgenltalia havE' unJl:rgone maswUni-
zatian. h.is 'onditlon IS commonly caused by congenltal adrenal hyperplasia, which
results in 1.:, ces" prQJucuon or anJrogen by the fetus,
B. Male pseudointersexuali y occurs when tewcll[ar tissue is present in a peBon with a
normal male karyotype 46, Y, but development or Lhe male external genitalia is
stunted. T b condition is commonly c3uspd by inaJequcue production of
aud. factor (Mlf).
C. Testicularfeminization yndrome when a 46 Y (enls dl've 0rs 'stes and female
(insread of male) em' 1 genitalia. This condition i., by a lack of androgel
e ep or' in the tit genital' 1.1' nd lahioocrC1l;al 5W Ilil g . These inJividuals are consid
ered I Q1C -licall ' gall and ciallv.
D. Hypospadias occur when the urogenu:al folds fail to fuse completely. As <1 result, tht::
urethra opens onto the ventral surface of the penis,
Reproductive System 37
Table 11-1
Developmenr of the Adult Female and Male Rerroductive System
IndIfferent Embryo
Gonads
Paramesonephric ducts
Mesonephric ducts
Mesonephric tubules
Urogenital sinus
Phallus
Urogenital folds
Labioscrotal swellings
Adult Female
Ovary, follicles, re e ovari,
Uterine tubes, uterus, cervix, and
upper part o. vagina
Duct of Gartner (vestigial)
Epoophoron, paroophoron (vestigial)
Urrnary bladder, urethra, urethral
and paraurethral glands, greater
vestibular gland,s. lower part of
vagina
Clitoris
abia minora
Labia majora
Adult Male
Testes, seminiferous tubUles,
rete testes
Appendix or testes (vestigial)
Epididymis, ductus deferens,
seminal vesicles, ejaculatory
duct
Efferent ductules
Urinary bladder, urethra, prostate
gland, bulbourethral glands
enis
entral aspect of peni
enile raphe
Scrotum
Scrotal raphe
Indifferent Embryo
Table 11-2
Fate of the Gubemacufllm und Pro,-es"wi aginalis
Adult Female Adult Male
Gubernaculum
Processus vaglnalls
of the uterus
E. Cryptorchidis OCClIIS when the teste:, fad. to dc"ceno lOTO the scrotum. ibr ral crypt-
ord1idisrn may result in 'u',
F. Hydrocele of tilt: OCCIJrS wh n a 'mall pareney !If the lWlica 'agina)t,
so thar flui ean t1 lW rntl It', resulting in a fluiu;fill :d c .. r near ill, t :.tcs,
G. ongenita 'oguina) hernia ccurs 'hen large ale-ney ()f thi: tunit.,* vClgltl.lI", emains
so that aloof 0 intestine hcrniares into the scrotWll.
38 Cllapter 11
Ductus
deferens
Epididymis
Ejaculatory
duct
/' ._........../ Semina
vesicle
Mesonephric tubule
Mesonephnc duet
TDF
MIF
Testosterone
9
Hymen
A
Paramesone hric ----!j
duet
8
Ep
Par
Duot 0 Gartner
Figure 11.-1. (A) The InL ifferent emlryo. The pmZJ.l1le:<onephric duel" (l major role in female developo
ment. TIle meson phnc ducts and LUbules playa major role in male dcvd()pmenr (I). dulr female, trlKturcs
form from ,1, paramcsc'nt'phnc duct dnd vestigial rem :mt, 01 the mcsonephrk d"'5ts and lubules. (C) Adult
male structures form (((1111 the mesonephnc ducts anJ tuhules and t"-stigial [ mmllm ot the pm:amesonephric
Juets. The prochl lIon of [ ["".determining f<l<:tor miillerian-mhibiting adIF) awl 'sto terone
JjreLf the mJifferel1t embryo t )W"rd n Ie de lOf'm nr. lis helieveJ ma Tl (a 220-amino acid nonhistone
proLein) . - the g oe pr()(lIlCl Lh STY g ne, whidl is I . ted on rhe $horr : on of the Y he mosom .
:l
Body Cavities
I. INTRAEMBRYONIC COE OM. The mtr:tl"tnhryooic .oclorn is initially one' conrmu.ous
space. The formation \It lhe pleuropericardial membranes and the diaphragm partitions this
space into th pericardial, pleural, and perlloncal cavities of the adult.
A. Pleuropericardial membranes are sheets of mesoderm that separate the pleural caviry
from the pencarclial caviry and later fom, the fibrous pericardium. TIlls relationship is
evidenced by the fact that, to reach the dIaphragm, the phrenic nerves course throllgh
the plcuropericardial membranes In the embryo and the fibrous pericardium in the adult.
B. Diaphragm. The diaphragm separates the pleural cavity from the peritoneal cavity.
1. Formation. It is fonned hy t e fusion of tissue (rom four sources.
a. The septum transvcrsum gives rise to the central tendon of the diaphragm in
the LlJult.
b. The pleuroperitonea! membranes contribute tissue to the diaphragm.
c. The dorsal mesentery of the esophagus gives rise to the crura of the diaphragm
III the adult.
d. The body wall muscle W tbe pc;riphery of the diaphragm.
2. Descent. The septum transver-um initially at the level ur C3- 5. FollOWing
the rapid growth of the nemal rube, the iliaphmgm descends. carrying the phrenic
nerves along with it.
II. CLINICAL CORRELATIONS
A. Congenital diaphragmatic hernia is . protrusion of the abdominal cnntems mto the
pleura! cavity fullowing failure of the pleuroperitonea! membrans to develtlp properly.
The hernia 11> most commonly ruund Oil [he left posterolateral side and (auses pulmonary
B. Esophageal hiatal hernia js th prorrusion of the stoma h into the pleural cavity through
an large esophageal hiatus. This condition renders the esophagogastric
sphinder incompetent. cau,ing the reflu..x l ( stomach content inlO the esophagus.
39
40
Nervous System
NEURAL TUBE
A. Formation 15-1)
1. The notochord induces the overlying ectoderm to differenriate into neuroectoderm
to form the neural plate. In the adult, the notochord fixll1s the nucleus pulposus
of the intervertebral disk.
2. The neural plate folds to give rise to the neural tube.
a. As the neural rlate folds, some cells differentiate ioro pluripotent neural rest
.
b. The neural tu e i:, initially cormectcd ro the amniotic cavity via the anterior
and posterior neuropores. The lamina tenninalis marks the location of the
anterior neuropore in the adulr.
B. Vcsidcs. 111e neural tube develops three primary vesicles and five sec ndary vesicles.
- These esicles give rise to various adult structures (Table 13-1).
C. CeUs of the neural tube waU give rise to the foUuwing cells of the central nervous
system (CNS).
1. Neuroblasts form all neurons wlthin the brain andspmal cord, including the pregan-
glionic sympathetic and pregangItonic parasympathetic neurons.
2. are the supporting cells withIn the CNS.
a. Astrocytes surroWld capillaries.
b. Oligodendrocytes produc myelin.
c. Ependymocytes line the ventricles and central canal.
d. Tanycytes Hne the third ventricle and transport substances from the cerebrospi-
nal fluid (CSF) to the hypothalamic portal system.
e. Choroid plexus cells produce CSF. The tight jWlCtions between them form the
blood-CSF barrier.
f. Microglia, phagocytic cells of the CNS, are derived from monocytes.
II. POSITIONAL CHANGES OF THE SPINAL CORD
A. At week 8 of development, the spinal cord extends the entire length ()f Lhc bony
ertebral canal.
B. Ar birth, rhe coous medullaris extends tQ the L3 vertebra.
C. In the adult, the conus medullaris extends to the LI vertebra.
A
Nervous System 41
/ Neural crest cells
Neural plate
C Alar (sensory) plate
Neural crest cells
Sulcus limitans
Basal (motor) plate
Agure 13-1. Srages m the evclopmem of the neural rube and neural crest cells. (A) The notochord
induces rhe overlying ectadem1 ro form rhe n ural plate. (8) The rk'ural plate folJ, to gIve ri,to tr) the neur"l
ube. As the neural plate folds. it gives fISC to neural crest celb. ( .) The sulcus liotitans is a groove in rhe
lateral wall of the ventricle that separates the alar (sensory) plate from the basal (motor) plate. TI,e al:n plate
becomes the dorsal horn of the spina! cord and the basal plate becomes the ventral horn of the spllla] cord.
42 Chapter 1
Table 13-1
Dcvelupmcnr ot the Brain from the Neur<ll Tube"
Primary Ves cles
Prosencephalon
Mesenceohalon
Rhombenc phalon
Secondary
Vesicles
Telencephalon
Diencephalon
Mesencephalon
Metencephalon
Myelenceph-
alon
Adult Derivatives
Cerebral hemispheres, basal ganglia. lamina terminalis.
olfactory bulbs, hippocampus
Epithalamus, tholamus. hypothalamus, neurohypo-
physIs. pineal glano, retina, optic nerve, mamillary
bodies
Midbrain
Pons. cerebellum
Medulla
*The remainder of the neural tube forms the spinal cord.
Table 13-2
Ungimtrlon III the N<::rvuw,
Embryonic Structure Adult Derivative
Basal plate of neura ube
Neural crest cells
Preganglionic sympathetic neurons within the intermediolateral cell
column
Postganglionic ympathetlc neurons within the sympathetic chair
ganglia and prevertebral gang!la
Embryonic
Structure
Basal pia e of
neural tube
Neurai crest cells
Table 13-3
Onginati n of the P,uasympathetic Ncrvuus ystcm
Adult Derivative
Preganglionic parasympathetic neurons within the nuclei of the midbrain (III),
pons (VII), and medulla (IX, Xi
Preganglionic parasympathetic neurons within thf' spinal cord nucleus at 52-54
Postganglionic parasympathetic neurons within the ciliary (III), pterygopalatine
(VII), submandibular (VII), otiC (IX). and entenc (X) ganglia
Postganglionic parasympathetic neurons within the ganglia of the abdominal
and pelvic cavities
III. MENINGES
A. The dura mater arises from mesoderm thar surr0unds the neural rube.
B. The pia mater and ar<lchnoid membrane arise from neural Cfe$t cell .
IV. AUTONOMIC ERVOUS SYSTEM
A. The sympathetic nervous system \)(iginates from the basal plate of rhe neural tube and
neural crest cells Crable 13-2).
B. Th parasympathetic nervous system also onglOates frum the plate of the neural
tube and neural cresr cells (Table 13-3).
Nervous System 43
V. HYPOPHYSIS
A. The adenohypophysis develops from an evagination of ecwderm from the roof of the
rimitive mouth <Rathke's pouch).
B. The neurohypophysis deve ops from an evagination f neuroecroderm from The ien-
ceph::llon.
VI. CLINICAL CORRELATIONS
A. Spina biida
1. Spina bifida occulta occurs when there is only a defect of the vertebral
2. Spina bifida with meningocele occurs when the menmges prOjeCt thmug a erte-
bral defeer.
3. Spina bifiJa with meningomyelocele occurs when rhe meninges and spinal cord
projecr through a "crtebral defect.
4. Spina bifida with mycloschisi. occurs when the neural tune fatls tl close, resulting
In an open :1cural tube on the surfclce of the . ad. Newborn infants are paralyzed
disLaJ to the lesion.
B. Anenccph:aly occur; when the anterior neuropore fal s tt close, resulting in failure of
the brain to develop. Generally, only a rudimentary brain stem is present.
C. Arnold-Chiari malformation occurs when pam If the cerebellum herntate through the
foramen magnum.
D. Dandy-Walker syndrome is :J congel1ltal hydrocephalus a,sodated With atresia of the
furamcn uf Luschka and foramen of Magendie.
E. is most commonly caused by stenOSl$ of the er' ral aqueJuct dUl ing
evelopmenr. Excessive CSF acculllulates in the ventricles and subarachnOld space.
F. Fetal alcohol svndrome LS the most common cau,e of mental retfUdation. It includes
microcephaly and congcOltal heart disease.
G. Craniopharyngioma is H Longcnital cystic tum r resulting from remnants o( Rathke'
pouch.
4
Ear
I. EMBRYOLOGIC ORIGINS. Table 1 -1 summanzes the emhryologlc. origins of the internal
ar, lTIlddle ear, and, xtem;1! t'<lr.
II. FORMATION. Figure 14 he f"lmnati<1n of therructures of the adult mternal ear.
Table 14-1
Dcr;yation l)[ the Strucrutes of the Ear
Embryonic Structure
OtiC esitle-*
Utricular portion
Saccular portion
Phal'jngcal arch 1
Pharyngeal arch 2
Pharyngeal pouch 1
Pharyngeal membran 1
Pharyngeal groove 1
Auricular hillocks
"Derived from surface ectoderm.
Adult Derivatives
Internal ear
Utricle, semicircular ducts, vestibular ganglion of eN VIII
Saccule, cochlear duct (organ of Corti). spiral ganglion of CN VIII
Middle ear
Incus. malleils, tensor tympani mUSCle
Stapes, stapedius muscle
Epithelial lilling of auditory tube and middle ear cavity
Tympanic membrane
External ear
Epithelial lining of external auditory meatu
Auricle
Agure 14-1. Schemauc transverse ectlOm shoWIl1R the fonnarion of the otic placode and otic vesicle
from urface ectoderm. (AI The oric placode Ulto the me>;<x.lerm and becomes otic
(B) The vestibular and spiral g<lnglia arc derived from t.he otic veslde. ee) The adult ear. Pharyngeal arch I
am.! phdryngeal ;trch 2 form the tapes (St), incu ), and mall us (M). Ur = utricle; Sac = saccule.
44
Ear 45
A B
Pharyngeal
arch 1 and 2
Pharyngeal
groove 1
/
Pharyngeal pouch 1
Vestibular ganglion
"T'\'.,.,......__
OtiC
vesicle
Dorsal aorta
c
haryngeal
membrane 1
- - -
I
: Utricle
: Semicircular
I duets
,
I Vestibular
Ot
' : ganglion (eN VIII)
IC I
vesicle'" - - - - -
J
: Saccule
Cochlear duet
(organ of Corti)
Spiral ganglion
(CNVIII)
Tympanic
membrane
15
Eye
I. EYE. The eye is formed in part (rom ;'\ neuroecrodemlal t'vagination of the diencephalon
l:alleJ dlt:: optic cup and optic stalk (Figure 15-]). In addirion, surface ectoderm (the lens
placode), mesoderm, and neural crest cells contribute to the fomlation of a 1 umber ot struc-
rure5 of the adult eye (Tuhle 15-1)
II. CLINICAL CORRELATIONS
A. Coloboma iridis occurs when dlC hor lei fissure fails tv do e, causing a cleft in the ifl.'.
B. Persistent iridupupillary membram: ccurs w en strands of conneclive nssue cover the
pur l.
Table 15-1
Derivation of the StnlCture or tbe Eye
Embryonic Structure
Neuroectoderm (diencephalon)
Optic cup
Optic stalk
Surface ectoderm
Lens placode
Mesoderm
Hyaloid artery and vein
Neural crest cell
Adult DerIvatIve
Retina, iris, ciliary body
Optic nerve (CN II)
Lens, anterior epithelium of cornea
Sclera, ubstantia propria of cornea, corneal endothelium, vitreous
body, extraocular muscles
Central artery and vein of retina (branch of the ophthalmic artery)
Choroid, sphincter pupillae muscle, dilator pupillae muscle, ciliary
muscle
Rgure 15-1. (A) Tbe )ptic cup and optic stalk are evaginanons of rhe Jienc.:ephalon. The oplic cup
induces ectoderm to differentiate imc) th" lens placod . (B) Fomlanon uf rne () tic nerve (eN II) (rom
the optiC talk. The choroi.d fissure. which is locatcd on the of e opLic stalk, permits access ot
the hyal id artery anJ vein to the inn r ;)Speet of the eye. The choroid fissure eventually close. As ganglion
cells form in the retina, axons accumubte in the optic ,md cause the inner and outer layers of the optic
stalk to fuse, ohliterating the lumen and forming the uptle llerve. (C) The adult eye. Note thaI' the sclera IS
continuous with the dura and the choroid is continuous with the pia-am. Maid. The iridopupillary mcrnbranc
is normally obliterated.
46
Eye 47
A
J ~ ~ Diencephalon
L ns placode
B
Axons from re Ina
ganglion cells
Optic nerve
(CN II)
Central artery and
vein of retina
Outer and Innel layers
of the optic stalk
/
Choroid iissure
closure
lumen of the
optIC stalk
Choroid fissure
Optic cup
Optic sfalk
c
Iris,
Cornea ~
(3 layers) ..........-..
Iridopupillary ---1-1
membrane
Sphincter/
pupillae muscle
Ciliary body
Vitre lUS ody
/
Sclera
Retina
-'entral artery of retina
...___- Dura
~ ~ ~ ~ ~ ~ = ~ E 5 Pia arachnoid
f OlJliG nerve
(eN II)
Extraocular muscle
You might also like
- High Yield EmbryologyDocument156 pagesHigh Yield Embryologynancyreis100% (5)
- Becker's USMLE Step 1 - Lecture NotesAnatomy (2013) (UnitedVRG)Document422 pagesBecker's USMLE Step 1 - Lecture NotesAnatomy (2013) (UnitedVRG)Gps Pandette80% (5)
- Updated Step 1 Bible (2013)Document669 pagesUpdated Step 1 Bible (2013)Rameez JafriNo ratings yet
- High-Yield Histology 2d Ed - Ronald W DudekDocument232 pagesHigh-Yield Histology 2d Ed - Ronald W Dudekbogdan21tNo ratings yet
- Becker's USMLE Step 1 - Lecture NotesBiochemistry, Genetics (2013) (UnitedVRG)Document278 pagesBecker's USMLE Step 1 - Lecture NotesBiochemistry, Genetics (2013) (UnitedVRG)Gps Pandette100% (1)
- BiochemistryDocument18 pagesBiochemistryMedSchoolStuff50% (2)
- USMLE Step 1 Online Coaching Course TopicsDocument91 pagesUSMLE Step 1 Online Coaching Course TopicsQworld0% (1)
- Becker's USMLE Step 1 - Lecture NotesBehavioral Science, Epidemiology, Biostatistics (2013) (UnitedVRG)Document238 pagesBecker's USMLE Step 1 - Lecture NotesBehavioral Science, Epidemiology, Biostatistics (2013) (UnitedVRG)Gps Pandette100% (5)
- Biochem High YieldDocument106 pagesBiochem High YieldEvelyn Lee Russell100% (1)
- High Yield - Gross AnatomyDocument142 pagesHigh Yield - Gross AnatomyDabala Harish Reddy100% (2)
- ReproductiveDocument8 pagesReproductiveMedSchoolStuffNo ratings yet
- High-Yield Histopathology 2e PDFDocument346 pagesHigh-Yield Histopathology 2e PDFmary100% (1)
- Download Kaplan USMLE STEP 1 Notes and High Yield Medical Study MaterialsDocument9 pagesDownload Kaplan USMLE STEP 1 Notes and High Yield Medical Study MaterialsdtilaniNo ratings yet
- Physeo RuntimesDocument9 pagesPhyseo RuntimesRubayet Tasfin AlifNo ratings yet
- Biochemistry, Usmle EndpointDocument272 pagesBiochemistry, Usmle EndpointDoctor SalameNo ratings yet
- 6 Week Calendar: Usmle Step 1Document3 pages6 Week Calendar: Usmle Step 1Nathalie Freites GonzalezNo ratings yet
- Pub High Yield Cell and Molecular BiologyDocument120 pagesPub High Yield Cell and Molecular Biologyрафаэль рустамовNo ratings yet
- Goljan High Yield Pathology QuestionsDocument3 pagesGoljan High Yield Pathology QuestionsTim0% (1)
- CardiovascularDocument18 pagesCardiovascularMedSchoolStuff100% (1)
- Pregnancy and Lactation Flashcards - Guyton Physiology Chapter 82Document19 pagesPregnancy and Lactation Flashcards - Guyton Physiology Chapter 82MedSchoolStuffNo ratings yet
- Sketchy Pharm (Benzo) ReviewDocument2 pagesSketchy Pharm (Benzo) ReviewMitz JuneNo ratings yet
- 100 Gross Anatomy ConceptionsDocument231 pages100 Gross Anatomy ConceptionsChris Kristofferson100% (1)
- Brs Embryology Q&ADocument41 pagesBrs Embryology Q&ASURG BLOCK100% (1)
- DIT QuestionsDocument183 pagesDIT QuestionsJake ChuengNo ratings yet
- TBDocument163 pagesTBBlaquevagabond0% (1)
- PHYSIOLOGY OF HUMAN DEVELOPMENT FROM FERTILIZATION TO IMPLANTATIONDocument68 pagesPHYSIOLOGY OF HUMAN DEVELOPMENT FROM FERTILIZATION TO IMPLANTATIONانس ابوهيبةNo ratings yet
- Rapid Review of Embryology, First PDFDocument137 pagesRapid Review of Embryology, First PDFmayurdadhaniya100% (1)
- Normal Gastrointestinal Embryology: Intestinal MalrotationDocument159 pagesNormal Gastrointestinal Embryology: Intestinal MalrotationDaNy ChiriacNo ratings yet
- ABDOMEN & PELVIS NotesDocument12 pagesABDOMEN & PELVIS NotesNavaal AnjumNo ratings yet
- EmbryologyDocument31 pagesEmbryologyBiyologebNo ratings yet
- Becker's USMLE Step 1 - Lecture NotesAnatomy (2013) (UnitedVRG)Document422 pagesBecker's USMLE Step 1 - Lecture NotesAnatomy (2013) (UnitedVRG)Khan A RehNo ratings yet
- Medical Genetics 4th Edition Jorde Test BankDocument4 pagesMedical Genetics 4th Edition Jorde Test BankOdettesNo ratings yet
- USMLE Step 1 - ReproductionDocument65 pagesUSMLE Step 1 - ReproductionMatt McGlothlin100% (1)
- Goljan Lecture OrderDocument2 pagesGoljan Lecture OrderKweku Grant-AcquahNo ratings yet
- Anatomy Quizbook Volume 2 Head and NeckDocument92 pagesAnatomy Quizbook Volume 2 Head and NeckSakhile NdlovuNo ratings yet
- High Yield Biochemistry PDFDocument41 pagesHigh Yield Biochemistry PDFKyle Broflovski100% (2)
- 28-DAY MED STUDY SCHEDULEDocument13 pages28-DAY MED STUDY SCHEDULEgemazy123100% (3)
- Brachial Plexus MnemonicsDocument6 pagesBrachial Plexus MnemonicsTima Rawnap.No ratings yet
- Cracking the USMLE with 99th Percentile ScoresDocument55 pagesCracking the USMLE with 99th Percentile ScoresShawn Gaurav Jha100% (7)
- Steven Katz, MSIVDocument109 pagesSteven Katz, MSIVfrabzi100% (3)
- UsmleDocument26 pagesUsmleuwandfaNo ratings yet
- Infectious Disease Pathology p56-75Document20 pagesInfectious Disease Pathology p56-75zeroun24No ratings yet
- 237 Goljan Rapid Review Images FlashcardsDocument34 pages237 Goljan Rapid Review Images FlashcardsAhsan Tanvir100% (1)
- Color Atlas Histology Gartner PDFDocument454 pagesColor Atlas Histology Gartner PDFrafaelalmadapicardiNo ratings yet
- 10 Ways To Succeed With USMLE Step 1Document19 pages10 Ways To Succeed With USMLE Step 1Zunaira Abdul Ghaffar100% (2)
- NeurologyDocument14 pagesNeurologyMedSchoolStuffNo ratings yet
- Khan USMLE Pearls MicroDocument8 pagesKhan USMLE Pearls Microlourdesfercab75% (4)
- Renal - Goljan SlidesDocument29 pagesRenal - Goljan SlidesJoan ChoiNo ratings yet
- Test Bank Larsens Human Embryology 5th EditionDocument22 pagesTest Bank Larsens Human Embryology 5th EditionRichard1LauritsenNo ratings yet
- Sweet Biochemistry: Remembering Structures, Cycles, and Pathways by MnemonicsFrom EverandSweet Biochemistry: Remembering Structures, Cycles, and Pathways by MnemonicsNo ratings yet
- International Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessFrom EverandInternational Medical Graduate and the United States Medical Residency Application: A Guide to Achieving SuccessRaghav GovindarajanNo ratings yet
- A Text - Book of Histology: Descriptive and Practical. For the Use of StudentsFrom EverandA Text - Book of Histology: Descriptive and Practical. For the Use of StudentsNo ratings yet
- Week One: I. Origin of The Germ LineDocument67 pagesWeek One: I. Origin of The Germ LinerohitNo ratings yet
- 1Document223 pages1Isaac Tan100% (2)
- Unlock SGCh22Document8 pagesUnlock SGCh22SilaxNo ratings yet
- Gametogenesis, Gamete Transport & FertilizationDocument56 pagesGametogenesis, Gamete Transport & FertilizationvictorNo ratings yet
- Managing Nerve InjuriesDocument6 pagesManaging Nerve InjuriesKhadim ShahNo ratings yet
- Gunshot Wounds To FaceDocument11 pagesGunshot Wounds To FaceKhadim ShahNo ratings yet
- Examining Ulcers: Key Factors in 17 StepsDocument5 pagesExamining Ulcers: Key Factors in 17 StepsKhadim ShahNo ratings yet
- GLUCOPHAGEDocument6 pagesGLUCOPHAGEKhadim ShahNo ratings yet
- Health, Prevention, Strategies To Prevent The Plaque DiseasesDocument5 pagesHealth, Prevention, Strategies To Prevent The Plaque DiseasesKhadim ShahNo ratings yet
- Examining Ulcers: Key Factors in 17 StepsDocument5 pagesExamining Ulcers: Key Factors in 17 StepsKhadim ShahNo ratings yet
- Rubber dam usesDocument2 pagesRubber dam usesKhadim ShahNo ratings yet
- Statistical Approach To Predict The Ischemic Heart DiseaseDocument3 pagesStatistical Approach To Predict The Ischemic Heart DiseaseKhadim ShahNo ratings yet
- Oral Pathology McqsDocument3 pagesOral Pathology McqsAdel Abdel-Azim79% (19)
- Red blood cell developmentDocument12 pagesRed blood cell developmentKhadim ShahNo ratings yet
- Biomechanics of the Upper ExtremityDocument33 pagesBiomechanics of the Upper ExtremityKhadim ShahNo ratings yet
- Oral PathologyDocument3 pagesOral PathologyKhadim Shah0% (1)
- Periodontology MCQDocument12 pagesPeriodontology MCQIndah Simamora67% (3)
- Red blood cell developmentDocument12 pagesRed blood cell developmentKhadim ShahNo ratings yet
- BDS THIRD PROFESSIONAL EXAMINATION 2007 ORAL PATHOLOGY MCQsDocument0 pagesBDS THIRD PROFESSIONAL EXAMINATION 2007 ORAL PATHOLOGY MCQskainath0150% (2)
- 1000 MCQ Bank QuestionsDocument157 pages1000 MCQ Bank Questionsapi-2629165193% (59)
- Conversion of Galvanometer Into VoltmeterDocument1 pageConversion of Galvanometer Into VoltmeterKhadim ShahNo ratings yet
- MedDocument149 pagesMedKhadim ShahNo ratings yet
- 2010-08-06 Benseler Imaging PDFDocument36 pages2010-08-06 Benseler Imaging PDFKhadim ShahNo ratings yet
- BDS THIRD PROFESSIONAL EXAMINATION 2007 ORAL PATHOLOGY MCQsDocument0 pagesBDS THIRD PROFESSIONAL EXAMINATION 2007 ORAL PATHOLOGY MCQskainath0150% (2)
- Chapter 49: The Submandibular RegionDocument2 pagesChapter 49: The Submandibular RegionKhadim ShahNo ratings yet
- Antibiotics 10700203 PDFDocument12 pagesAntibiotics 10700203 PDFKhadim ShahNo ratings yet
- MID Bacteria Charts JkuoDocument17 pagesMID Bacteria Charts Jkuotsukino143100% (2)
- Emg Conceptos - Nerve Conduction StudiesDocument23 pagesEmg Conceptos - Nerve Conduction StudiesDeborah SalinasNo ratings yet
- Peri Implant Health: Mauricio G. Araujo - Jan LindheDocument7 pagesPeri Implant Health: Mauricio G. Araujo - Jan LindheCristian CulcitchiNo ratings yet
- Chapter 31 - Assessment and Management of Patients With Vascular DisordersDocument7 pagesChapter 31 - Assessment and Management of Patients With Vascular DisordersMichael Boado100% (1)
- Skenario 2 Saraf & PerilakuDocument30 pagesSkenario 2 Saraf & PerilakuPrima Eriawan PutraNo ratings yet
- Physical ExaminationDocument117 pagesPhysical Examinationsasmita nayakNo ratings yet
- Learning Theories of PersonalityDocument13 pagesLearning Theories of Personalitypavitra_madhusudanNo ratings yet
- The Tongue of Leopard Gecko (Eublepharis Macularius) LMDocument9 pagesThe Tongue of Leopard Gecko (Eublepharis Macularius) LMSandra Clavero ClopèsNo ratings yet
- JBS Haldane On Being The Right SizeDocument8 pagesJBS Haldane On Being The Right Sizeboygenius21_39464798100% (2)
- PsychSim 5 Quizzing - Chapter 6-Sensation and PerceptionDocument5 pagesPsychSim 5 Quizzing - Chapter 6-Sensation and Perceptionneecee126100% (1)
- 8 Curious Meridians Exercises for LongevityDocument6 pages8 Curious Meridians Exercises for Longevitypeter911x100% (2)
- Bioactive Lipid Mediators - (2015)Document424 pagesBioactive Lipid Mediators - (2015)MohammedAjebliNo ratings yet
- Holter SolutionsDocument4 pagesHolter SolutionsgimenNo ratings yet
- NPTEL Stress Management MCQ AssignmentDocument5 pagesNPTEL Stress Management MCQ AssignmentSnehaNo ratings yet
- Brewing Technology (2017)Document190 pagesBrewing Technology (2017)Јован АдамовNo ratings yet
- LP UapDocument18 pagesLP UapHat MutisalNo ratings yet
- ICU-Acquired Weakness and Recovery From Critical IllnessDocument9 pagesICU-Acquired Weakness and Recovery From Critical IllnessFebrian ParuraNo ratings yet
- Osmosis Diffusion Active - Transport+studentDocument35 pagesOsmosis Diffusion Active - Transport+studentMetaknight360 LiveNo ratings yet
- Mind Maps in Biochemistry - (Metabolism of Carbohydrates)Document23 pagesMind Maps in Biochemistry - (Metabolism of Carbohydrates)Gus LionsNo ratings yet
- FCA (SA) - Part - II - Past - Papers 10Document30 pagesFCA (SA) - Part - II - Past - Papers 10matentenNo ratings yet
- University of Phoenix Anatomy and Physiology Week 2 QuizDocument2 pagesUniversity of Phoenix Anatomy and Physiology Week 2 QuizSophia FHSNo ratings yet
- Histological Characteristics of the Lingual FrenulumDocument1 pageHistological Characteristics of the Lingual FrenulumajudNo ratings yet
- Byssinosis PDFDocument8 pagesByssinosis PDFFaza AlhinduwanNo ratings yet
- Introduction 1 Esoteric HealingDocument20 pagesIntroduction 1 Esoteric HealingChicowski Caires100% (1)
- Principles & Practice of First AidDocument298 pagesPrinciples & Practice of First AidJoshua100% (2)
- Bone Marrow A Practical Manual (2011)Document212 pagesBone Marrow A Practical Manual (2011)Victor Lage de AraujoNo ratings yet
- OSCHMANDocument7 pagesOSCHMANapi-3708784100% (1)
- Module 1. General and Special Questions of Clinical Laboratory Diagnostics Text Test QuestionDocument229 pagesModule 1. General and Special Questions of Clinical Laboratory Diagnostics Text Test QuestionA.h.MuradNo ratings yet
- Hubtex Forklift DQ 45 G 3050 El T Operating Instructions and Spare Parts List deDocument23 pagesHubtex Forklift DQ 45 G 3050 El T Operating Instructions and Spare Parts List dewilliamalexandermd041189tkz100% (71)
- Test Bank TNCC Full Solution Pack All TNCC Exams and Study Questions Are Here All Answered CorrecDocument109 pagesTest Bank TNCC Full Solution Pack All TNCC Exams and Study Questions Are Here All Answered Correcmary011danielNo ratings yet
- From: Rapid Interpretation of EKG'sDocument14 pagesFrom: Rapid Interpretation of EKG'sLucija Kljaić100% (1)