You might also like
- Crohns Disease PDFDocument3 pagesCrohns Disease PDFjetri0905No ratings yet
- Double-Glove 2Document4 pagesDouble-Glove 2jetri0905No ratings yet
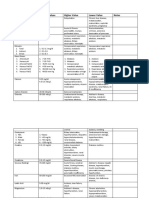
- Test Normal Values Higher Value Lower Value NotesDocument6 pagesTest Normal Values Higher Value Lower Value Notesjetri0905No ratings yet
- Running Head: Relationship Between Nursing 1Document3 pagesRunning Head: Relationship Between Nursing 1jetri0905100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Root Canals: What To Expect During A ROOT CANALDocument3 pagesRoot Canals: What To Expect During A ROOT CANALKuntum Khaira UmmahNo ratings yet
- VITAMIN K Drug StudyDocument2 pagesVITAMIN K Drug StudyMarl DumiligNo ratings yet
- Ssri Presentation - 674 - Final2Document52 pagesSsri Presentation - 674 - Final2api-289842236100% (1)
- IVTDocument6 pagesIVTpatzieNo ratings yet
- Buteyko OutputDocument6 pagesButeyko OutputFatimatus Zahroh IchsanNo ratings yet
- National Mediclaim Policy PDFDocument19 pagesNational Mediclaim Policy PDFTanmoy Pal ChowdhuryNo ratings yet
- Hygiene 1Document36 pagesHygiene 1Mayom MabuongNo ratings yet
- MDR in DetailsDocument370 pagesMDR in Detailssachin100% (2)
- "Mdicleaim": Mamta Ashok GuptaDocument50 pages"Mdicleaim": Mamta Ashok GuptaKarishma Dharmesh SoohindaNo ratings yet
- VOLUX 尖沙咀 chung parr hall 鍾伯豪醫生 PDFDocument8 pagesVOLUX 尖沙咀 chung parr hall 鍾伯豪醫生 PDFAnonymous YT4f4ejNtH100% (1)
- Antimicrobial Disk Diffusion Zone Interpretation Guide: Working PaperDocument3 pagesAntimicrobial Disk Diffusion Zone Interpretation Guide: Working Papermajdi bilbisiNo ratings yet
- Age NCPDocument2 pagesAge NCPCharmaine Dela CruzNo ratings yet
- Dr. Andy Tampubolon, SPS - Management of Diabetic NeuropathyDocument26 pagesDr. Andy Tampubolon, SPS - Management of Diabetic NeuropathyAthalia TalawayNo ratings yet
- Functional Medicine Coaching PDFDocument142 pagesFunctional Medicine Coaching PDFAnabell Garcia100% (13)
- MetaanalysisDocument12 pagesMetaanalysisAhmed BadrNo ratings yet
- Presbyopia: Care of The Patient WithDocument34 pagesPresbyopia: Care of The Patient Withbebek sakitNo ratings yet
- Circadian Rhythm Sleep Disorders CRSDDocument11 pagesCircadian Rhythm Sleep Disorders CRSDjaime manciaNo ratings yet
- 5 IV CannulationDocument61 pages5 IV CannulationNursing Superintendent (SH)No ratings yet
- GECKO-CRF v1.1Document2 pagesGECKO-CRF v1.1David Rendra MahardikaNo ratings yet
- Terminal Illness and DeathDocument37 pagesTerminal Illness and DeathJAYSON KING100% (2)
- Book Review of Peter Bartlett, Oliver Lewis and Oliver Thorold, Mental Disability and The European Convention On Human RightsDocument6 pagesBook Review of Peter Bartlett, Oliver Lewis and Oliver Thorold, Mental Disability and The European Convention On Human RightsJohn RussellNo ratings yet
- Protocol For Malaysian HospitalsDocument434 pagesProtocol For Malaysian HospitalsSidney Lee100% (1)
- Acute PyelonephritisDocument27 pagesAcute PyelonephritisLucia CaseNo ratings yet
- Vapormate MSDS 2016Document7 pagesVapormate MSDS 2016parejayaNo ratings yet
- Practice Questions 1Document51 pagesPractice Questions 1Lucille Isidro CruzNo ratings yet
- Ii. Draping:: A. AnesthesiaDocument4 pagesIi. Draping:: A. AnesthesiaJo Hn VengzNo ratings yet
- Solomon Ankle Injury PDFDocument9 pagesSolomon Ankle Injury PDFHikmah Wahid AkbarNo ratings yet
- Tugas Ringkasan UU PrekursorDocument37 pagesTugas Ringkasan UU PrekursorshanhikariNo ratings yet
- Psychoanalytic TherapyDocument28 pagesPsychoanalytic Therapyapi-3704513100% (3)
- Plab Mock TestsDocument17 pagesPlab Mock TestsMisbah ShahzadiNo ratings yet