You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Sample Appellant BriefDocument6 pagesSample Appellant BriefKaye Pascual89% (9)
- FBC MNCS Service-, Error-, Infocodes ENDocument23 pagesFBC MNCS Service-, Error-, Infocodes ENDragos Stoian100% (1)
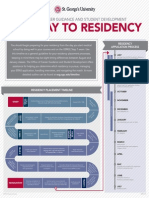
- ST Georges University Pathway To ResidencyDocument1 pageST Georges University Pathway To ResidencyMark HilmyNo ratings yet
- FALL 2012: Parasitology Final ExamDocument14 pagesFALL 2012: Parasitology Final ExamMark HilmyNo ratings yet
- PerspectiveDocument2 pagesPerspectiveJahangeer KhanNo ratings yet
- PerspectiveDocument2 pagesPerspectiveJahangeer KhanNo ratings yet
- c270 KW NTA855G2 60 HZDocument31 pagesc270 KW NTA855G2 60 HZAhmad El KhatibNo ratings yet
- Surface Finish Measurement NotesDocument32 pagesSurface Finish Measurement NotesAneez ShresthaNo ratings yet
- Metaphysics of LucretiusDocument6 pagesMetaphysics of LucretiusChristopher BennettNo ratings yet
- Cold Regions Science and TechnologyDocument8 pagesCold Regions Science and TechnologyAbraham SilesNo ratings yet
- Metal Workers BizHouse - UkDocument3 pagesMetal Workers BizHouse - UkAlex BekeNo ratings yet
- Airport Security Post 9-11Document7 pagesAirport Security Post 9-11lewisNo ratings yet
- 1 Circuit TheoryDocument34 pages1 Circuit TheoryLove StrikeNo ratings yet
- Aquaculture Scoop May IssueDocument20 pagesAquaculture Scoop May IssueAquaculture ScoopNo ratings yet
- Adaptive Reuse Architecture Documentation and Analysis 2168 9717 1000172Document9 pagesAdaptive Reuse Architecture Documentation and Analysis 2168 9717 1000172Komal HundiaNo ratings yet
- Hashimoto's Thyroiditis: Veena RedkarDocument10 pagesHashimoto's Thyroiditis: Veena RedkarSan RedkarNo ratings yet
- Azure Machine Learning StudioDocument17 pagesAzure Machine Learning StudioNurain IsmailNo ratings yet
- W0L0XCF0866101640 (2006 Opel Corsa) PDFDocument7 pagesW0L0XCF0866101640 (2006 Opel Corsa) PDFgianyNo ratings yet
- 1n5711 RF Detector Diode 70v PIV DatasheetDocument3 pages1n5711 RF Detector Diode 70v PIV DatasheetgordslaterNo ratings yet
- The Manufacture and Uses of Expanded Clay Aggregate: Thursday 15 November 2012 SCI HQ, LondonDocument36 pagesThe Manufacture and Uses of Expanded Clay Aggregate: Thursday 15 November 2012 SCI HQ, LondonVibhuti JainNo ratings yet
- Principles Involved in Baking 1Document97 pagesPrinciples Involved in Baking 1Milky BoyNo ratings yet
- Vanish Magic Magazine VANISH MAGIC MAGAZINE 58 May 2019Document118 pagesVanish Magic Magazine VANISH MAGIC MAGAZINE 58 May 2019mick byrnes100% (1)
- Water Filling MachineDocument15 pagesWater Filling Machinepallab D RozarioNo ratings yet
- Ujian 1 THN 4Document13 pagesUjian 1 THN 4Che Shuk ShukaNo ratings yet
- Ruhangawebare Kalemera Godfrey Thesis PDFDocument116 pagesRuhangawebare Kalemera Godfrey Thesis PDFYoobsan Tamiru TTolaaNo ratings yet
- Flow Zone Indicator Guided Workflows For PetrelDocument11 pagesFlow Zone Indicator Guided Workflows For PetrelAiwarikiaar100% (1)
- Exercise On Word Formation 2 (Unit 2 - Advanced) : Tran Dai Nghia High School For The GiftedDocument3 pagesExercise On Word Formation 2 (Unit 2 - Advanced) : Tran Dai Nghia High School For The GiftedEveryonehateshiuzo 2.0No ratings yet
- 2nd APJ Abdul Kalam Essay Writing CompetitionDocument2 pages2nd APJ Abdul Kalam Essay Writing CompetitionANURAG SINGHNo ratings yet
- Model Detailed Project Report: Animal Feed Making UnitDocument19 pagesModel Detailed Project Report: Animal Feed Making UnitShashi ShekharNo ratings yet
- Orbitol Motor TMTHWDocument20 pagesOrbitol Motor TMTHWRodolfo ErenoNo ratings yet
- Compiled LecsDocument24 pagesCompiled LecsNur SetsuNo ratings yet
- VavDocument8 pagesVavkprasad_56900No ratings yet
- Terminals of Ecm: E3 E4 E5 E6Document2 pagesTerminals of Ecm: E3 E4 E5 E6jeremih alhegn100% (1)
- SR No Service CodeDocument30 pagesSR No Service CodeShiva KrishnaNo ratings yet