You might also like
- Oral Surgery FlapsDocument13 pagesOral Surgery Flapshaneefmdf100% (1)
- FCMFOS (SA) Regulations 18 12 2022Document17 pagesFCMFOS (SA) Regulations 18 12 2022haneefmdfNo ratings yet
- UK Job Scope For MRGCP INTDocument1 pageUK Job Scope For MRGCP INThaneefmdfNo ratings yet
- Middle Third Fracture MCQDocument6 pagesMiddle Third Fracture MCQhaneefmdf83% (6)
- Tracheal Deviation - Causes and TreatmentDocument5 pagesTracheal Deviation - Causes and TreatmenthaneefmdfNo ratings yet
- 9 Kyorin UniversityDocument2 pages9 Kyorin UniversityhaneefmdfNo ratings yet
- National Board of Dental Examination (Nbde) Tips: Boardvitals BlogDocument5 pagesNational Board of Dental Examination (Nbde) Tips: Boardvitals BloghaneefmdfNo ratings yet
- Primary CareDocument184 pagesPrimary Carehaneefmdf100% (1)
- Mandibular Fracture MCQDocument6 pagesMandibular Fracture MCQhaneefmdf67% (9)
- Inverted L OsteotomyDocument9 pagesInverted L OsteotomyhaneefmdfNo ratings yet
- PGDIM2015Document12 pagesPGDIM2015haneefmdfNo ratings yet
- Cases of MaxillofacialDocument5 pagesCases of MaxillofacialhaneefmdfNo ratings yet
- Age-Dependant Cephalometric Standards As Determined by Multilevel Modeling ABOUT SNADocument2 pagesAge-Dependant Cephalometric Standards As Determined by Multilevel Modeling ABOUT SNAhaneefmdfNo ratings yet
- Socket Shield Technique 11Document11 pagesSocket Shield Technique 11haneefmdfNo ratings yet
- 270 Accel Tapered WebDocument4 pages270 Accel Tapered WebhaneefmdfNo ratings yet
- A Countdown To Orthognathic SurgeryDocument5 pagesA Countdown To Orthognathic SurgeryhaneefmdfNo ratings yet
- Ena 1Document4 pagesEna 1haneefmdfNo ratings yet
- Quick Start - Prosthetics: ImpladentDocument3 pagesQuick Start - Prosthetics: ImpladenthaneefmdfNo ratings yet
- Handleman - Point The Case For Nonsurgical ExpansionDocument11 pagesHandleman - Point The Case For Nonsurgical ExpansionhaneefmdfNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Depression, Anxiety and Stress During COVID-19: Associations With Changes in Physical Activity, Sleep, Tobacco and Alcohol Use in Australian AdultsDocument13 pagesDepression, Anxiety and Stress During COVID-19: Associations With Changes in Physical Activity, Sleep, Tobacco and Alcohol Use in Australian AdultsKeysha VinoraNo ratings yet
- The Latest:: Veg. Vs Non-VegDocument44 pagesThe Latest:: Veg. Vs Non-VegedwincliffordNo ratings yet
- Mass Gatherings Evidence ReviewDocument72 pagesMass Gatherings Evidence ReviewRogueNo ratings yet
- Catmon National High School: Summative Test in MAPEH 10 - Health 3 QuarterDocument2 pagesCatmon National High School: Summative Test in MAPEH 10 - Health 3 QuarterJoselito EubraNo ratings yet
- Endogenous Fungal Endophthalmitis Following Intensive Corticosteroid Therapy in Severe COVID-19 Disease Expedited Publication, Original ArticleDocument6 pagesEndogenous Fungal Endophthalmitis Following Intensive Corticosteroid Therapy in Severe COVID-19 Disease Expedited Publication, Original ArticleNurul FebrianiNo ratings yet
- Sprouts of Iman Parent HandbookDocument17 pagesSprouts of Iman Parent HandbookSamara DugalNo ratings yet
- Primary Immunodeficiency DiseasesDocument24 pagesPrimary Immunodeficiency DiseasesClaire Henderson100% (1)
- SINGAPORE Occupational Health and Safety Guidelines For Laboratories and Production Facilities in The Biomedical Sciences.259190104 PDFDocument85 pagesSINGAPORE Occupational Health and Safety Guidelines For Laboratories and Production Facilities in The Biomedical Sciences.259190104 PDFStansilous Tatenda NyagomoNo ratings yet
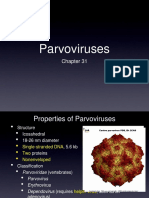
- ParvovirusDocument8 pagesParvovirusAldila safitriNo ratings yet
- Become Healthy or Extinct by Darryl D'Souza-1Document288 pagesBecome Healthy or Extinct by Darryl D'Souza-1Asha ShivaramNo ratings yet
- Clinical Microbiology-I SEMESTER-IDocument26 pagesClinical Microbiology-I SEMESTER-IAreeba NazNo ratings yet
- Sharma - 2023 - Emerging Evidence On Monkeypox - Resurgence, Global Burden, Molecular Insights, Genomics and Possible ManagementDocument21 pagesSharma - 2023 - Emerging Evidence On Monkeypox - Resurgence, Global Burden, Molecular Insights, Genomics and Possible ManagementIsabella FernandesNo ratings yet
- Laboratory Associated Infections: Tania Chintya IKD BiomedikDocument16 pagesLaboratory Associated Infections: Tania Chintya IKD BiomedikTania Chintya Dewi KarimaNo ratings yet
- Spss Assignment 1 KhadirDocument7 pagesSpss Assignment 1 KhadirMohammad KhadeerNo ratings yet
- Nicolle2008 PDFDocument12 pagesNicolle2008 PDFRizki Noor AmeliaNo ratings yet
- Physiology in Health and Disease (2018)Document391 pagesPhysiology in Health and Disease (2018)crackintheshat100% (1)
- CCDM Manual PDFDocument715 pagesCCDM Manual PDFrehanaNo ratings yet
- 4th ThesisDocument26 pages4th ThesisArjay Ladiana50% (8)
- Animal Health Care and Management NC III (Autosaved)Document98 pagesAnimal Health Care and Management NC III (Autosaved)Mark Warren Atienza Revellame100% (2)
- Quotes On Vaccines by Health Care ExpertsDocument29 pagesQuotes On Vaccines by Health Care ExpertsM. R. WildeNo ratings yet
- TrismusDocument4 pagesTrismusEkaNo ratings yet
- Cedar Crest College Clinical and Concept Map Worksheet For Nursing 330 PediatricsDocument13 pagesCedar Crest College Clinical and Concept Map Worksheet For Nursing 330 Pediatricsapi-405374041No ratings yet
- English: Quarter 3 - LESSON 1Document11 pagesEnglish: Quarter 3 - LESSON 1Nina Romina NavaltaNo ratings yet
- Introductory MicroBiology With PracticalsDocument118 pagesIntroductory MicroBiology With Practicalsmatrixxxx420100% (1)
- NCMH - Burden of Disease - (29 Sep 2005)Document388 pagesNCMH - Burden of Disease - (29 Sep 2005)jyoti dua100% (1)
- TARUN SETHI 28Y - M-CDocument1 pageTARUN SETHI 28Y - M-CArun SethiNo ratings yet
- Hope Segment 2 Final Exam ReviewDocument5 pagesHope Segment 2 Final Exam ReviewschneidercornNo ratings yet
- Nclex TipsDocument93 pagesNclex TipsAmiel Francisco Reyes86% (7)
- Onchocerciasis in Mozambique - An Unknown Condition For Health Professionals PDFDocument13 pagesOnchocerciasis in Mozambique - An Unknown Condition For Health Professionals PDFStélioNo ratings yet
- TB Test AlternativeDocument7 pagesTB Test Alternativejohn_crassNo ratings yet