Professional Documents
Culture Documents
Kap
Uploaded by
Yet Barreda BasbasCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Kap
Uploaded by
Yet Barreda BasbasCopyright:
Available Formats
i
REPORT
Prepared by : Gfk MODE Pvt. Ltd. 60/2, Ist Floor, BL House, Yusuf Sarai, New Delhi-110016
CONTRIBUTORS
Gfk MODE:
Dr. R.B.Gupta Dr. Piyusha Majumdar Raghu Maharishi Ridhima Bahl
UNION:
Dr Nevin Wilson Dr Sarabjit S Chadha Dr A Sreenivas Dr Srinath Satyanarayana Mr Subrat Mohanty Dr Subhash Yadav Dr Geetanjali Sharma
iii
ACKNOWLEDGEMENT
This study was successfully completed due to the efforts and involvement of numerous individuals at different stages of the survey. We would like to thank everyone who was involved in the entire research work. We are extremely thankful to Dr. Nevin Wilson, Regional Director of The Union, South-East Asia Regional Office for giving us an opportunity to conduct this study. We gratefully acknowledge the immense help received from Dr Sarabjit Chadha (Project Director) and all the members of the Programme Management Unit of The Unions Global Fund Round 9 India TB Project (Project Axshya) during various phases of study. They also provided us guidance regarding preparation of tools tabulation plan and report for the study. We would like to thank Deputy Director General (TB), Central TB Division, Ministry of Health and Family Welfare, Government of India for giving their permission and the authority letters to conduct study in 15 states of India. Thanks are also due to, all the General Population, People Infected with TB, Health service providers, NGOs and opinion leaders who spent their valuable time and responded to the interview schedule. We also appreciate the efforts taken by the GfK MODEs Research and Field Teams for completing the study successfully in a stipulated time period. We hope this report will be proved helpful in the decision making process at various levels.
Study Team GfK MODE Social Research Unit
iv
ABBREVIATION
ASHAs : Accredited Social Health Activists ACSM : Advocacy communication and social mobilization ANM : Auxiliary Nurse Midwife AWW : Anganwadi Worker CBO: Community Based organization DOT : Directly observed Therapy Shortcourse DMC : Designated Microscopy Centre HIV: Human Immunodeficiency virus IPC: Interpersonal Communication KABP : knowledge, Attitude, Behaviour & Practice LT : Lab Technician MDR - TB : Multidrug Resistant Tuberculosis NGO: Non Governmental Organization NFHS : National family Health Survey PLHWA : People living with HIV and AIDS PPM : public Private Mix PSU : Primary Sampling unit PR : Principle Recipient RNTCP: Revised National Tuberculosis Control Program SPSS: Statistical Package for Social Science SC: Sputum Collection centre UNION : International Union Against Tuberculosis and Lung Disease WVI : World Vision India
Content Page No.
Executive Summary .............................................................................................................................................I-VI CHAPTER 1: BACKGROUND, STUDY OBJECTIVES AND METHODOLOGY ............................................................... 1 1.1 BURDEN OF DISEASE ........................................................................................................................................ 2 1.2 THE TB CONTROL STRATEGY ............................................................................................................................ 2 1.3 TUBERCULOSIS SITUATION IN INDIA................................................................................................................ 3 1.4 GLOBAL FUND ROUND 9 INDIA TB PROJECT .................................................................................................. 5 1.5 SPECIFIC OBJECTIVE OF THE STUDY: ................................................................................................................ 5 1.6 SURVEY INSTRUMENTS .................................................................................................................................. 10 1.7 SAMPLE IMPLEMENTATION AND DATA COLLECTION.................................................................................... 11 1.8 RECRUITMENT, TRAINING AND FIELDWORK ................................................................................................. 12 1.9 ETHICS ............................................................................................................................................................ 14 1.10 DATA PROCESSING........................................................................................................................................ 14 CHAPTER 2: GENERAL POPULATION .................................................................................................................. 16 2.1 DEMOGRAPHIC CHARACTERSTICS OF THE RESPONDENTS ........................................................................... 16 2.2 HOUSEHOLD CHARACTERISTICS AND ASSETS ............................................................................................... 18 2.3 KNOWLEDGE, ATTITUDE AND PRACTICES..................................................................................................... 22 CHAPTER 3: TB DISEASED PERSONS ................................................................................................................... 33 3.1 DEMOGRAPHIC CHARACTERISTICS OF TB DISEASED PERSONS .................................................................... 34 3.2 HOUSING CHARACTERISTICS AND ASSETS .................................................................................................... 35 3.3 KNOWLEDGE, ATTITUDE & PRACTICES ......................................................................................................... 39 CHAPTER 4: HEALTH SERVICE PROVIDERS ......................................................................................................... 49 4.1 KAP ON TUBERCULOSIS................................................................................................................................. 50 4.2 TREATMENT APPROACH OF HEALTH SERVICE PROVIDERS ........................................................................... 51 4.3 PRECAUTION AND RECOMMENDATION ....................................................................................................... 53 4.4 PERCEPTION OF HEALTH SERVICE PROVIDERS ON DOTS/ RNTCP ................................................................ 54 CHAPTER 5: OPINION LEADERS .......................................................................................................................... 58 5.1 PROFILE .......................................................................................................................................................... 58 5.2 KNOWLEDGE ON TREATMENT OF TB ............................................................................................................ 61 5.3 KNOWLEDGE AND PRACTICES- ROLES PLAYED BY OPINION LEADERS .......................................................... 62 CHAPTER 6: NON-GOVERNMENTAL ORGANIZATION/COMMUNITY BASED ORGANIZATION ........................... 65 6.1 GENERAL PROFILE OF NGO/CBO FUNCTIONARIES ....................................................................................... 65 6.2 NGO/CBOS KNOWLEDGE, ATTITUDE & PRACTICES ON TUBERCULOSIS ....................................................... 66 6.3 ROLE OF THE NGOS ....................................................................................................................................... 69 6.4 COMMUNITY PARTICIPATION- NGO/CBOs ................................................................................................... 71 CHAPTER-7: STIGMA AND DISCRIMINATION ....................................................................................................... 73 7.1 CONCEPTUAL FRAMEWORK .......................................................................................................................... 73 7.2 ASSESSING STIGMA AND DISCRIMINATION AMONG GENERAL POPULATION .............................................. 74 7.3 VALUES - SHAME, BLAME AND JUDGMENT .................................................................................................. 75 ANNEXURE ............................................................................................................................................................ 84
List of Table
Table No. Table 1.1 Table 1.2 Table 1.3 Table 2.1 Table 2.2 Table 2.3 Table 2.4 Table 2.5 Table 2.6 Table 2.7 Table 2.8 Table 2.9 Table 2.10 Table 2.11 Table 2.12 Table 2.13 Table 2.14 Table 2.15 Table 2.16 Table 2.17 Table 2.18 Table 2.19 Table 3.1 Table 3.2 Table 3.3 Table 3.4 Table 3.5 Table 3.6 Table 3.7 Table 3.8 Table 3.9 Table 3.10 Table 3.11 Table 3.12 Table Name Number of household interviews, number of interviews with General Population and TB diseased persons by urban-rural residence Number of Respondents interviewed (General Population, TB Diseased, Health Service Providers and Opinion Leaders) stratified by zones Number of Respondents (GP, TB Diseased, Service Providers, Opinion Leaders & NGOs) interviewed stratified by state Socio demographic characteristics of respondents from the General Population Household Characteristics of Respondents from the General Population Household assets owned by respondents of the general population Characteristics of respondents who had heard of TB Awareness of the symptoms of TB among the respondents who had heard of TB disaggregated by zones (N=3823) Awareness of the mode TB transmission among the respondents who had heard of TB disaggregated by zones (N=3823) Respondents opinion on the people who are more prone for TB in the community disaggregated by zones (N=3823)* Respondents awareness of the mode of diagnosis for tuberculosis stratified by Zone Opinion of the respondents on the seriousness of the TB disease and about curability Best treatment for TB (among those who considered TB as a curable disease completely or partially) and the duration of treatment Proportion of respondents who had heard of the term DOTS Proportion of respondents who had heard of DOTS knew that TB treatment is available free of cost under DOTS Self-perception of the susceptibility to develop TB disease among the respondents Major Reasons why respondents felt that they cannot develop TB Cough among respondents and their care seeking behaviour Source of TB related information of the respondents Respondents reply to Visit by any individual to provide information on Tuberculosis Respondents response to the query on visit by people to provide TB related information Summary of key Indicators* on TB Related Awareness at the project level stratified by Zone Distribution of the patients identified during the course of the survey disaggregated state wise Characteristics of TB Diseased Persons Household Characteristics of TB Diseased Persons Assets/Possession of Households of TB patients identified during the survey TB patients awareness on what causes Tuberculosis Symptoms experienced by TB diseased Persons prior to the diagnosis of the present episode of TB Duration between onset of symptoms to diagnosis of tuberculosis Health seeking behaviour of TB diseased Persons prior to diagnosis Diagnosis of tuberculosis among Diseased Persons Treatment for TB among TB diseased persons Health Seeking Behaviour of households of TB diseased Persons Source of Information for TB Diseased Persons Page No. 11 12 12 17 19 20 22 23 24 25 26 26 27 28 28 29 29 30 30 31 31 31 33 34 36 37 39 40 41 41 42 45 46 47
ii
Table No. Table 4.1 Table 4.2 Table 4.3 Table 4.4 Table 4.5 Table 4.6 Table 5.1 Table 5.2 Table: 5.3 Table 5.4 Table 5.5 Table 6.1 Table 6.2 Table 6.3 Table 6.4 Table 6.5 Table 6.6
Table Name General Characteristics of Service Providers Knowledge on Tuberculosis (Multiple response*) Tuberculosis Diagnosis and treatment approach of Health Service Providers Challenges, precautions and advises given by Health Service Providers in dealing with Tuberculosis Patients Perception of Health Service Providers on DOTS/ RNTCP Summary of Key KAP survey Indicators of Health Care Providers General Profile of Opinion Leaders interviewed during the survey Knowledge of Opinion Leaders on TB, Symptoms, mode of transmission and diagnosis of Tuberculosis Opinion leaders Knowledge on treatment of tuberculosis Awareness of the opinion leaders on the availability of diagnostic and treatment facilities and the role played by them in their community to address TB Summary of Key KAP survey Indicators of Opinion Leaders General Profile of NGO/CBO representatives identified for the KAP Survey Knowledge about Tuberculosis among NGO functionaries NGO/CBO Representatives Knowledge on TB Symptoms, Mode of transmission and Diagnosis of Tuberculosis NGO/CBO Representatives Knowledge on TB treatment, duration and DOTS Activities done by NGO/ CBO representatives on the addressing TB in their localities Community Participation NGO/CBOs (Multiple Response*)
Page No. 49 51 52 54 55 56 58 60 62 63 64 65 67 67 68 70 71
iii
List of Figure
Figure No. Figure 2.1 Figure 3.1 Figure 5.1 Figure 7.1 Figure 7.2 Figure 7.3 Figure 7.4 Figure 7.5 Figure 7.6 Figure 7.7 Figure 7.8 Figure 7.9 Figure 7.10 Figure 7.11 Figure 7.12 Figure 7.13
Figure Name Proportion of Respondent Households Considered to be of Low SLI stratified by State Proportion of TB patients living in the Lowest Standard of Living Index disaggregated by State Profile of Opinion Leaders included in the survey Fear of casual Transmission and refusal to contact with TB persons among General Population Value, Shame, Blame and Judgment Enacted Stigma (Discrimination) Fear of casual Transmission and refusal to contact with TB diseased persons Enacted Stigma (Discrimination) Abuse and Rejection Disclosure Opinion Leaders Perspective on Stigma and Discrimination Fear of Causal Transmission Value, Shame, Blame and Judgement Enacted Stigma Opinion of NGO Representatives on Stigma and Discrimination Value, Shame, Blame and Judgement Enacted Stigma
Page No. 21 38 59 76 76 77 78 79 79 79 80 80 81 82 82 83
Project Axshya Baseline Knowledge, Attitude and Practices on tuberculosis Survey Executive Summary Background India is the highest TB burden country accounting for nearly one fourth of the global incidence. Tuberculosis (TB) is an infectious bacterial disease that spreads through the air and most commonly affects the lungs (pulmonary TB). Once infected, a person has about a 10% lifetime risk of developing the disease. The most common symptom of a person with pulmonary TB is cough of two weeks or more. Patients are usually diagnosed by sputum smear examination and once detected; TB is curable with 6-8 months of treatment. The diagnosis (sputum smear examination) and treatment of TB is made available free of cost by Government of Indias Revised National Tuberculosis Control Programme (RNTCP). All TB patients registered in the RNTCP are treated under directly observed therapy (DOT). RNTCP uses the WHO recommended Stop TB Strategy for the control of TB in India. Axshya is a Global Funded Round 9 India TB project launched in 2010, that will reach 374 districts across 23 states in the country in a phased manner and expand the reach and visibility of the RNTCP through increased civil society engagement at the community and the individual levels. Marginalized and vulnerable populations, women and children living in these districts will be prioritized. Axshya will be implemented through two civil society Principal Recipients (PRs) International Union Against Tuberculosis and Lung Disease (The Union) and World Vision India. Project activities will focus on advocacy, communications and social mobilization at all levels from the village to the national level. In this regard, in order to provide evidence based guidance to the civil society Principal Recipients in implementing the ACSM activities, a baseline Knowledge, Attitude and Practices survey was conducted. The information generated through this survey is expected to be representative of the various demographic and social characteristics of population living in these districts, keeping in view the relationship between these characteristics to tuberculosis control, and the activities visualised under global fund Rd 9 India TB project and also act as a baseline to later measure the impact of the project activities. Objectives of the survey Through this survey an attempt has been made to Gather baseline information on TB related knowledge, attitude and practices among five representative segments of the community namely general population, TB Diseased persons, opinion leaders, non-governmental organisations and health services providers.
ii
Explore attitudes and experiences of stigma and discrimination related to TB within these segments. Understand the attitude of the segments towards TB patient with particular reference to gender. Identify individual, social and environmental barriers including provider and patient delay that contribute to low TB case detection and poor completion of TB treatment. Identify sources of information on TB and level of exposure to mass media channels.
Methodology A cross sectional community-based survey was conducted. Thirty districts out of the 374 global fund project districts were selected by a stratified cluster sampling technique. Districts were initially stratified into the 4 RNTCP zones (north, south, east and west) of the country. The number of districts in each zone was selected in proportion to the distribution of the 374 districts in the respective zones of the country and the required number of districts in each zone was selected by population proportionate to size sampling. From each of these districts, the population was divided into urban and rural primary sampling units of approximately 250 households (the average approximate population in each household is 4 and the approximate size of the primary sampling unit is 1000 population), based on the data available from the countrys 2001 census. Ten primary sampling units were selected randomly in each district from the urban and rural primary sampling units in proportion to the districts estimated urban and rural population. The study was implemented by The Union, South-East Asia Regional Office with assistance from field investigators of the social research organization GfK MODE. The trained field investigators visited the preselected primary sampling units during the months of January to March, 2011 and conducted a household line listing. After this line listing process, the respondents from the General Population, TB patients (identified by interviewing heads of the households or other available household members to know whether any current household member was known to be suffering from TB (or an equivalent local term referring to TB), the locally available health service providers, opinion leaders and representatives of Non-Governmental Organizations were identified and interviewed by a semi-structured questionnaire designed to provide information on knowledge, attitude and practices of these respondents with respect to tuberculosis.
iii
Results General Population A sample of 4562 respondents was selected from the General population which included 1067 respondents from the north zone states, 1234 respondents from the east zone states, 1202 respondents from the west zone states and 1059 respondents from the South Zone states. The proportion of males to females was also equal (51% and 49% respectively). About 84% of the total respondents had heard of TB, 69% were having knowledge that a cough of two weeks or more could be TB; half of them (50%) knew that TB is caused by bacteria/germs and is transmitted through air. More than half (55%) knew that TB can by diagnosed by sputum examination. Although 80% believed that TB is curable, only about 37% knew that 6-8 month of treatment is needed. Only 23% had heard of the term DOTS, and less than a fifth (19%) knew that free treatment for tuberculosis is available under DOTS. Approximately 10% of the respondents were having cough of more than 2 weeks in the last two months prior to the survey. Out of those with cough of more than 2 weeks, only about one third (37%) visited a health facility for seeking care or sputum examination. TB Diseased People A total of 752 TB patients were identified of which 609 (81%) were interviewed. This included 145 patients from the north zone, 235 patients from the east zone, 124 patients from the west zone and 105 patients from the south zone. Nearly two thirds of the respondents (64%) were males, 43% were illiterate and 35% of them belonged to households with a current monthly income of less than two thousand Indian Rupees. One third (33%) of them were aware that TB is caused by microorganisms, 70% of them had heard of free diagnosis and treatment of TB, 68% had visited less than 3 health care providers prior to the diagnosis of tuberculosis and nearly 60% of them had undergone diagnosis in a government health facility. Nearly three fourths (74%) were diagnosed as having tuberculosis within 1 month of the onset of symptoms and 69% were initiated on treatment within 7 days of diagnosis. Overall 54% were determined to be receiving treatment free of cost under DOTS. Although 80% were aware that treatment has to be taken regularly, only 55% knew that the duration of TB treatment is for 6-8 months. Health Service providers
iv
A total of 614 health service providers (HSPs) were identified to be providing medical services in the primary sampling units and all of them were interviewed during the survey. More than half of them (55%) were qualified practitioners of allopathic medicine, 26% were qualified practitioners of Ayurveda medicine, 12% were qualified practitioners of homeopathic medicine and 5% were practitioners of Unani system of medicine and the remaining were not qualified in any of the systems of medicine mentioned above. Almost 94% of the HSPs considered A cough of two weeks as a predominant symptom of TB and 79% had said that sputum smear examination is the preferred mode of diagnosis of tuberculosis and that that the diagnostic and treatment services are available free of cost at the Government hospitals. 71% of the health service providers had informed the patients to go to the nearest government hospital for the treatment of tuberculosis when they diagnosed TB among them or if the patients sought their advice for the treatment of tuberculosis, and almost all of them had said that they have treated TB in the past and 88% had prescribed/dispensed allopathic drugs for the treatment of TB. 79% of the health service providers had information that the duration of TB treatment is for 6-8 months. Only two thirds of the HSPs had heard of multi-drug resistant TB and 54% knew that MDR has to be diagnosed by Culture and Drug Susceptibility testing. The predominant source of TB related information to the HSPs was medical text books or journals. Opinion Leaders Opinion leaders are influential leaders in the society to whom people look upon for advice, opinion and views thus significantly affecting the course of action taken by the people within a community. These opinion leaders are primarily functionaries at grass root working in different capacities and mainly comprise of elected representatives of Panchayati Raj Institutions like Village Pradhan, Sarpanch/Panch/Ward members, religious leaders, teachers or health functionaries like ANM (Auxiliary Nursing Midwife) AWW (Anganwadi Worker). A total of 511 such opinion leaders were interviewed. All of them had heard of TB and 88% knew that cough of two weeks or more is the predominant symptom of TB, 78% knew that TB is transmitted from person to person through air when the diseased person coughs or sneezes and almost 80% knew that sputum has to be tested for the diagnosis of tuberculosis. Only 22% of the opinion leaders were able to include TB in the top 5 health priorities of their community.
More than 90% of the opinion leaders knew that TB is curable, that allopathic medicines are the predominant mode of treatment of tuberculosis and 62 % knew that the duration of TB treatment is for 6-8 months. Nearly 90% of the opinion leaders informed that the Government hospitals are the places for TB diagnosis and treatment. Less than two thirds (59%) of the opinion leaders had heard of the term DOTS and were able to associate this term with tuberculosis. Less than one fourth of the respondents (22%) had taken any initiative to address TB control in their localities and the most common form of initiative was by being a DOT Provider to the TB patients. Non-Governmental Organizations/Community Based Organizations For this a total 51 NGOs/CBO were identified (by information given by the opinion leaders or members of the general community who were interviewed) to be working in the 300 primary sampling units of the 30 districts. Their head of the organisations were interviewed. Nearly half (51%) of them informed that they were doing activities that were related to tuberculosis control in their localities. More than three fourths (78%) of the respondents informed that TB is a major public health problem in our country and 100% of them believed that TB disease is completely curable. More than 90% of them had heard of DOTS and knew that diagnosis and TB treatment is provided free of cost at all government health facilities. More than 90% of them were able to identify cough of more than 2 weeks as tuberculosis, and that it spreads through air when a TB diseased person coughs or sneezes, nearly all persons mentioned that allopathic system of treatment is the best method to treat tuberculosis and that the treatment has to be taken for 6-8 months duration. 41% of them were involved in the RNTCP schemes and the most common scheme that they were involved is the ACSM scheme. Almost 84% had expressed their interest to collaborate with the RNTCP in one or the other schemes to address tuberculosis control in their localities. Limitations of the Survey While we believe that the findings are valid, there are some limitations to the study First, these data are not nationally representative but representative of the 374 Global Fund Round 9 ACSM intervention districts.
vi
These district were selected for the project interventions by RNTCP based on their relatively poor programme performance. Second, the study identified respondents based on a door to door household survey and some of the respondents were identified based on Self-reported (eg TB patients, opinion leaders, heads of the NGO representatives). Third, only 10% of respondents of all stakeholder categories were re-visited to cross check the accuracy of the information gathered by the field investigators and was found to be accurate in more than 95% of the cases. Fourth, we were not able to interview nearly 20% of the TB patients identified in this survey due to certain operational and ethical reasons (non-availability of TB patients or the heads of their households at the time of interview). The only two variables by which we could assess whether the patients interviewed were similar to the patients not interviewed were the zone and the urban / rural status of the patients. Conclusions This community based survey provides valuable information on the current levels of knowledge, attitudes and practices of the various stakeholders of the population with respect to TB. This report provides data that shows the gaps and opportunities for enhancing the reach, visibility and access of the Government of Indias Revised National TB Control Programme within the framework of the ACSM component of Global Fund Round 9 India TB project. Further detailed analysis of the individual components of the survey can provide valuable information that will be helpful in finding appropriate strategies, interventions to address the TB control challenges in the country.
CHAPTER 1 BACKGROUND, STUDY OBJECTIVES AND METHODOLOGY
Tuberculosis (TB) is one of the oldest diseases known to affect mankind as shown by the findings of tuberculous spinal disease in Egyptian mummies. The Greeks called the disease phthisis (consumption), emphasizing the dramatic aspect of general wasting associated with chronic untreated disease. It has also been referred to in the Vedas and Ayurvedic Samhitas as the Kshaya Rog. The infectious etiology was debated until It was first isolated in 1882 by a German physician named Robert Koch who received the Nobel Prize for this discovery. It is very well now known that TB is an infectious disease caused by bacteria whose scientific name is Mycobacterium Tuberculosis. Effective anti-tuberculosis drugs were available in the middle of last century, but in Europe and the United States, mortality rates began to decrease decades before the introduction of antimycobacterial drugs due to improvement in socio-economic conditions thereby establishing the fact that TB and poverty are closely related. A person can become infected with tuberculosis bacteria when he or she inhales minute particles of infected sputum from the air. The bacteria get into the air when someone who has tuberculosis coughs.1 Tuberculosis is spread (transmitted) primarily from person to person by breathing air which contains bacilli. This usually happens during close contact. When the inhaled tuberculosis bacteria enter the lungs, they can multiply and cause a local lung infection. The local lymph nodes associated with the lungs may also become involved with the infection and usually become enlarged. The hilar lymph nodes (the lymph nodes adjacent to the heart in the central part of the chest) are often involved. Only small bacilli are needed to cause infection. Failure of the immune system to control infection with TB bacilli leads to active disease, when TB bacilli multiply and cause damage in the body. Only a small fraction (10%) of the people infected with the tuberculosis bacteria develop the disease during their lifetime. Left untreated, each person with infectious TB will spread the germs to about 10 - 15 people every year.
Tuberculosis definition, symptoms and cause in Wikipedia
1.1
BURDEN OF DISEASE Mycobacterium tuberculosis remains the single most serious pathogen worldwide and a major global public health problem in much of the developing world. Globally it is estimated that more than 9 million people develop active tuberculosis (TB) disease every year of which nearly 4 million cases are sputum smear-positive, the majority of whom are in the developing countries[1]. This is due to the failure to cure a high proportion of sputum smear-positive cases, population growth, HIV-epidemic and other socio-economic and demographic factors (poverty, migration, etc). Globally the HIV epidemic worsened the TB situation, increasing the number of tuberculosis cases and accelerating the spread of the disease. TB kills more adults than all other infectious diseases combined. More children are orphaned because of TB than because of any other infectious disease. TB was declared a global emergency by WHO in 1993, and countries round the world have intensified their measures towards TB control programs. In fact, the threat of HIV/ AIDS alerted them to potential danger of TB resurgence.
1.2
THE TB CONTROL STRATEGY World Health Organization and its partners across the world are implementing a six point Stop TB Strategy which builds on the successes of DOTS while also explicitly addressing the key challenges facing TB. Its goal is to reduce the global burden of tuberculosis by 2015 by ensuring all TB patients, including for example, those coinfected with HIV and those with drug-resistant TB, benefit from universal access to high quality diagnosis and patient-centered treatment. The strategy also supports the development of new and effective tools to prevent, detect and treat TB. The Stop TB Strategy underpins the Stop TB Partnership's Global Plan to Stop TB 2006-2015.2 This stop TB strategy contains 6 key components: Pursue high-quality DOTS expansion and enhancement Address TB/HIV, MDR-TB and other challenges Contribute to health system strengthening Engage all care providers Empower people with TB, and communities Enable and promote research
Stop TB Partnership and World Health Organization, Geneva (2006) Global Plan to Stop TB 20062015
All high TB burden countries across the world recognize and have endorsed the importance of completely implementing all components of the strategy for reducing the burden of TB control. 1.3 TUBERCULOSIS SITUATION IN INDIA India is highest TB burden country in the world, accounting for nearly one-fifth of the global incidence. In 2010, out of the estimated global annual incidence of 9.4 million TB cases, 2 million were estimated to have occurred in India, of whom 0.9 million were infectious cases.3
Global TB Report WHO 2009
SOME MAJOR FACTS ABOUT TUBERCULOSIS IN INDIA
Estimated Mortality o o 330,000 deaths due to TB each year Over 900 deaths a day 2 deaths every 3
Previous estimated Incidence of new smear positive T.B in India - 75 (PTB in 1 lakh Population) North - 95 East - 75** West - 80 South - 75**
minutes
TB-HIV o 2.31 million people living with HIV (PLWHA) 10-15% annual risk (60% lifetime risk) of developing active TB disease in PLWHA Estimated ~ 5% of TB patients are HIV infected Estimated Incidence of TB in India Annually - 2 million new cases Annually - 0.9 million new smear positive cases
The Revised National TB Control Programme (RNTCP), based on the internationally recommended Directly Observed Treatment Short-course (DOTS) strategy, was launched in 1997, expanded across the country in a phased manner. Full nationwide coverage was achieved in March 2006 covering over a billion populations (1114 million) in 632 districts / reporting units. In terms of treatment of patients, RNTCP has been recognized as the largest and the fastest expanding TB control programme in the world. The goal of TB control Programme is to decrease mortality and morbidity due to TB and cut transmission of infection until TB ceases to be a major public health problem in India. The current focus of the programme is on ensuring universal access to quality TB diagnosis and treatment services to all TB patients in the community.
1.4
GLOBAL FUND ROUND 9 INDIA TB PROJECT Recognizing the vital need for Advocacy, Communication and Social Mobilisation activities and in order to sustain the gains achieved by RNTCP and to realise its new objective of ensuring universal access, The Global Fund Round 9 India TB proposal is built on the Global Fund principle of Dual Track Financing envisages bridging one of the most challenging gaps in Tuberculosis control. Diagnosis and treatment of DR-TB through programmatic activities and seeks to strengthen quality of basic DOTS services through civil society participation in a country that bears 20% of global burden of TB. The project activities related to diagnosis and treatment of MDR-TB under Programme will be undertaken by the Central TB Division (PR1) as one of the Principal Recipient (PR). The civil society component through 2 civil society PRs- the International Union against Tuberculosis and Lung Diseases (The Union) and World Vision India (WVI) endeavours to address challenges in programme implementation and access to quality TB care. The project specifically addresses these issues through the project activities on Advocacy, Communication and Social Mobilization (ACSM) in identified 374 districts of the country. The ACSM activities include high-level advocacy for political and administrative support, implementation of the RNTCP ACSM strategy at the state and district levels, and social mobilization to garner community demand for TB services. Civil society involvement aims at strengthening engagement of providers and communities, complement programme efforts in human resource development, supervision and monitoring, and access to diagnostics, increased commitment to DRTB and TB-HIV from all levels, enhancing engagement of community-based ASHAs (Accredited Social Health Activists), engage more providers in RNTCPs revised schemes, and some exemplary awareness raising efforts. The project will broaden the scope of civil society involvement in TB services through an enduring National Partnership to link RNTCP to other stakeholders through National and State coordination committees. In order to provide the evidence to guide the civil society PRs in implementing the ACSM activities in its full sense and to act as a baseline for measuring the impact of the project activities, a baseline study was conducted on the knowledge, attitude & practice of tuberculosis in a representative sample of 30 project districts in 15 states of India.
1.5
SPECIFIC OBJECTIVE OF THE STUDY: The specific objective of the study were the following
Gather baseline information on TB related knowledge, attitude and practices among general population, TB diseased persons, opinion leaders and health services providers. Explore attitudes and experiences of stigma and discrimination related to TB among general public and persons/relations affected by the disease. Understand the attitude of the segments towards TB patient with particular reference to gender. Identify individual, social and environmental barriers including provider and patient delay that contribute to low TB case detection and poor completion of TB treatment. Find out the health seeking behaviour of women and men, especially the vulnerable groups such as people living in hard to reach areas, backward communities etc., with reference to TB related symptoms. Study the role of key community influencers and NGOs in RNTCP. Map the media habits/preferences of the beneficiaries. Identify sources of information on TB and exposure to mass media channels
Sample Size: Sample sizes required for each population (for each district) were calculated on the basis of the following factors typically used in surveys with probability samples and provided by The Union to GfK-Mode: The minimum sample size required for the measurement of changes on given indicator is a function of four factors: The initial or base level of the key variable/proportion of the eligible population The magnitude of change that needs to be detected reliably The level of significance The power of testing
The two set of indicators used for calculating sample size individually for General population & those diseased with TB are as follows A. Proportion of General Population in the district with correct knowledge on TB B. Proportion of TB diseased Persons in the district with correct knowledge on TB
The sample size for each district have been calculated using the formula
2 1 [ Z 1 2 P (1 P) + Z 1 P1 (1 P1 ) + P2 (1 P2 ) ] n= * *D R ( P2 P1 ) 2
Where n = required sample size D = Design effect P1 = Proportion estimated P2 = Expected value of the indicator P = (P1 + P2)/ 2 Z1- = z score corresponding to desired level of significance Z1- = z score corresponding to desired level of power To estimate within 95% CI, with a absolute precision of + 10% the proportion of general population in the district with correct knowledge of TB (mode of transmission, symptoms, treatment and curability). Assuming a cluster sampling methodology with a design effect of 1.5, a sample size of 131 individuals was required. Assuming 20% non-response rate a sample of 150 individuals were interviewed in each district. For TB patients on treatment, assuming that 50% of them have correct knowledge of TB, for estimating sample size, with a precision of + 10% at the district level, a sample size of 24 patients was required. Assuming cluster sampling method and a 10% nonresponse rate a sample size of 52 TB patients were need to be contacted per district. A three stage stratified random sampling method was used to select target respondents for the study. Stage 1: Selection of Districts Stage 2: Selection of PSUs Stage 3: Selection of Households Stage 1: Selection of Districts It was decided to select a minimum of at least 30 districts out of the 374 districts. These 30 districts would have representation from the districts covered by The Union and World Vision. Since Union will be implementing the project in 300 districts and World Vision in 74 districts, 24 out of 30 districts were from the districts covered by the Union PR and 6 from the world vision PR.
Thirty districts out of the 374 global fund project districts were selected by a stratified cluster sampling technique. Districts were initially stratified into the 4 RNTCP zones (north, south, east and west) of the country. The number of districts in each zone was selected in proportion to the distribution of the 374 districts in the respective zones of the country and the required number of districts in each zone was selected by population proportionate to size sampling (Table 1).The following table provides the list of districts in each of the zone PR wise and also some other characteristics of the districts.
Zones Union-PR WV PR Grand Total No. of districts to be selected No. of union PR districts selected No. of World Vision PR districts selected 0 1 3 2 6
North Zone South Zone East Zone West Zone Grand Total
89 53 74 85 301
0 7 46 21 74
89 60 120 106 375
7 6 9 8 30
7 6 5 6 24
The List of 30 districts selected for the survey was as follows:
Zone North North North North North North North South South South South South South East East East Principal recipient The Union The Union The Union The Union The Union The Union The Union World Vision The Union The Union The Union The Union The Union The Union The Union The Union State Uttar Pradesh Uttar Pradesh Uttar Pradesh Uttar Pradesh Punjab Haryana Haryana Andhra Pradesh Karnataka Tamil Nadu Tami Nadu Kerala Kerala Mizoram Bihar Bihar Agra Banda ** Faizabad Maharajganj** Hoshiarpur Panipat Sirsa Medak Bijapur Erode Vellore Thiruvananthapuram Kollam Aizwal Lakhisarai ** Nalanda ** District Population 42 18 20 33 16 11 13 29 20 28 38 35 28 4 9 27
Zone East East East East East East West West West West West West West West
Principal recipient The Union World vision The Union The Union World vision World vision The Union The Union World vision The Union World vision World vision The Union The Union Bihar Bihar
State
District Purnia ** Saran ** Uttar Dinajpur Gharwa Bhubaneshwar Corp Koraput Bhopal Hoshangabad ** Sehore ** Sagar ** Barwani Kanker * Mumbai Jhunjhunun
Population 29 37 27 16 7 13 21 13 13 24 13 8 133 22
West Bengal Jharkhand Orissa Orissa Madhya Pradesh Madhya Pradesh Madhya Pradesh Madhya Pradesh Madhya Pradesh Chhatisgarh Maharashtra Rajasthan
* tribal districts ** Poor and backward districts both poor and backward districts
Stage 2: Selection of Primary Sampling Units (PSUs) In each district, 10 primary sampling units which were villages for rural areas and wards for urban areas were selected by Population Proportional to size sampling procedure (PPS). The urban: rural ratio of the primary sampling units in each district was maintained in proportion to the districts actual urban rural population ratio. For selection of PSU, census 2001 list served as a sampling frame. The list of villages and wards were separately drawn from each district. The villages and wards were arranged in the ascending order based on their population size. The required number of PSUs from each district was selected using circular systematic sampling procedure. Stage 3: Selection of Households and Respondents In every primary sampling unit, a house listing operation was carried out. The listing provided the necessary sampling frame for identification of respondents from the general population and for selecting self-reported TB diseased persons from each primary sampling unit. The house listing process involved assigning numbers to each residential structure, recording address and location of these structures, and listing the name of all the persons in the households, identification of head of the household and screening the household members for the presence of self-reported TB diseased persons. In order to obtain the awareness on the tuberculosis among general population, 15 persons aged 18 years and above interviewed from each PSU.
10
These 15 persons such persons were selected by systematic sampling method from the list of persons identified in the house listing process; the male is to female ratio selected for the interview was 1:1. All self-reported TB Patients identified in each primary sampling unit were included in the study. In order to have a better understanding of the RNTCP programme, health service providers role, barrier in treating TB patients, stigma and discrimination associated with the disease, certain qualitative interviews were also carried out with different stakeholders from the identified PSU and district level. All Health service providers, opinion leaders and NGOs working in the primary sampling units were line listed and interviewed. While interviewing the respondents of the general population and the TB patients, they were asked to identify the health service providers that they usually visit and opinion leaders that they usually seek advice for health/medical care related matters. All such medical providers and opinion leaders, if located within the primary sampling units were line listed and interviewed. The non-governmental organisations working in the area of the primary sampling units were identified based on interviews of the village/ward representatives, and then the local heads of these identified organisations were interviewed. 1.6 SURVEY INSTRUMENTS The main instrument used for collection of data in this survey was a set of separate semi-structured questionnaires for General Population, TB diseased, Health Service Providers, Opinion Leaders and NGOs.. The questionnaire was developed in English and then translated in 10 local regional languages (Hindi, Bengali, Marathi, Telagu, Kannada, Tamil, Malayalam, Oriya, and Assamese). The final translated questionnaire was pilot tested with the target groups, mainly for language checks and partly to ascertain that most issues are covered. The English version of the questionnaires are enclosed in annexures. General Population Questionnaire: - The respondents were persons identified from the general Population who is the usual member of the household. Information on the age, sex, marital and education status were collected. Efforts were made to get Information on the Standard of Living Index. Information was collected on Knowledge, awareness and practice on TB, Stigma and discrimination associated with TB, Health seeking behaviour, media habits and source of Information. TB Diseased People Questionnaire - The respondents for this questionnaire was TB patients identified from the household listing (both undergoing treatment and who have taken treatment in last 1 year).
11
Information was also collected on knowledge, awareness and practice on TB, stigma and discrimination associated with TB, Health seeking behaviour, media habits and sources of information. The demographic and socio-economic statuses of these people were also obtained. Health Service Providers Questionnaire: - This questionnaire was designed for health service provider working in the health facility of the primary sampling for the past 5 years. The questionnaire was intended to collect information on the knowledge and treatment on TB, Barrier in TB detection and treatment of TB cases, involvement in RNTCP Programme. Opinion Leader Questionnaire: - The respondents for this questionnaire were opinion leader/Religious leader & ward member/Panchayat member of community. Information collected included knowledge on TB and, TB control services, stigma and discrimination, role of opinion leader in referral of TB patients, Initiatives taken by Opinion Leaders to address TB in their locality. NGO Questionnaire: NGO Questionnaire was for NGO representatives working in Health and non health sector. Information was collected on knowledge, attitude and practice on TB, stigma and discrimination, role of NGOs in referral of TB patients, Initiatives taken by NGO.
1.7
SAMPLE IMPLEMENTATION AND DATA COLLECTION The fieldwork was carried out in all the fifteen states simultaneously. The fieldwork started in 15 states on 5th January, 2011 and completed on 24th February, 2011. The fieldwork was carried out in 30 representative districts from the states of Uttar Pradesh, Punjab, Haryana, Rajasthan, West Bengal, Orissa, Bihar, Mizoram, Karnataka, Tamil Nadu, Kerala, Andhra Pradesh, Maharashtra, Chhattisgarh and Madhya Pradesh. The total numbers of respondents in each stakeholder group their stratified zone wise and state wise is given in Tables 1.1, 1.2 and 1.3. Table 1.1: Number of household interviews, number of interviews with General Population and TB diseased persons by urban-rural residence.
Sample Coverage Number of General Population Interviewed Number of TB Diseased Persons Interviewed Rural 3388 468 Urban 1174 141 Total 4562 609
12
The total number of respondents covered during the survey was 6347. Zone wise number of respondents interviewed from each category was provided in the table below. Table 1.2: Number of Respondents interviewed (General Population, TB Diseased, Health Service Providers and Opinion Leaders) stratified by zones
Sample coverage General Population TB Diseased Person Health Service Providers Opinion Leader NGOs North 1067 145 150 131 8 East 1234 235 164 143 18 West 1202 124 164 138 12 South 1059 105 136 99 13 Total 4562 609 614 511 51
Table 1.3: Number of Respondents (GP, TB Diseased, Service Providers, Opinion Leaders & NGOs) interviewed stratified by state
State Uttar Pradesh Punjab Haryana Rajasthan West Bengal Orissa Bihar Mizoram Karnataka Tamil Nadu Kerala A.P Maharashtra Chhattisgarh Madhya Pradesh Total GP 617 150 300 150 317 617 150 155 451 298 155 150 150 150 752 4562 TB Diseased 99 2 44 27 30 26 168 11 30 45 24 6 1 5 91 609 Service Providers 82 21 47 27 20 42 81 21 22 59 35 20 20 19 98 614 Opinion Leaders 70 19 42 19 18 39 69 17 20 54 6 19 20 20 79 511 NGOs 6 2 2 1 7 8 2 3 6 2 2 1 9 51
1.8
RECRUITMENT, TRAINING AND FIELDWORK GfK-MODE, conducted TOT (Training of Trainers) workshop in two phases; one in North zone and other in south zone. The purpose of this workshop was to ensure uniformity in data collection procedure in different states. Unions technical team also attended the workshop to give its technical inputs to the trainers.
13
Field Executives received training in the workshop subsequently trained the field staff (Investigators and supervisors) in each state according to the standard procedures discussed in the Training of Trainers (TOT) workshop. Training consisted of classroom training, demonstration and practice interviews, as well as field practice. Field staff in each state was trained over a period of three days.
Ist TOT: 27th 30th December Venue: Conference Hall, Gfk MODE Pvt. Ltd. Delhi
IInd TOT: 3rd 5th January, 2011 Venue: Conference Hall, Gfk MODE Pvt. Ltd, Chennai
The fieldwork in each state was carried out by a number of interviewing teams, each team consisting of four investigators and one supervisor. One such team was deployed in each state. Prior to the main field work at each primary sampling unit, house listing exercise was carried out by a team of two listers in order to list all persons and TB diseased persons in each PSU. Experienced and qualified interviewers were hired from our panel of investigators, taking into consideration their education background and experience in health-related surveys. The field supervisor was responsible for the overall management of the field team. In addition, the field supervisor conducted spot-checks to verify the accuracy of key information, particularly with respect to the eligibility of respondents. In each state monitoring and supervision was performed by the field executive of Gfk MODE & Unions staff. From time to time, Unions professional staff and GfK-MODE professional staff based in New Delhi visited the field sites to monitor the data collection operation.
14
1.9
ETHICS The study was reviewed and approved by the Ethics Advisory Group of the International Union Against Tuberculosis and Lung Disease. Permission to conduct the study was also obtained from the Central TB Division, Ministry of Health and Family Welfare, Government of India. At the Primary Sampling Units, information about the survey was provided to the heads of the primary sampling units. Written informed consent was obtained from the heads of the households and the individuals being interviewed.
1.10
DATA PROCESSING Data Processing of KAP study involved office editing, double data entry by using FoxPro software, and verification of data entry, by the Gfk MODE. All completed questionnaires were sent to the Analysis office of the Gfk MODE for editing and data processing (including office editing, coding, data entry, and machine editing). Although field supervisor examined every completed questionnaire in the field, the questionnaires were re-edited by office editors. The office editors checked all skip sequences, response codes that were circled, and information recorded in filter questions. The data were entered directly from the pre coded questionnaires, usually starting within one week of the receipt of the first set of completed questionnaires. Data entry and editing operations were usually completed a few days after the end of fieldwork in each state. Computer based checks were used to clean the data, and inconsistencies were resolved on the basis of information recorded in the questionnaires. The tables were generated by SPSS/MERLYN Software. Data Analysis Since one of the key objectives of the study was to assess the knowledge level among the community partners and stakeholders a two way approach was adopted. Firstly respondents were judged on the basis of answers given by them on various issues separately. Later on questions related to the knowledge part were assimilated to understand the holistic/complete knowledge about TB. These questions were binary coded as 1 and 0 (i.e. Knowledge and Ignorant) on the basis of responses made by the general population. This was followed by constructing a summary score (Knowledge Score) by clubbing all these questions together.
15
Experience and challenges Presence of The Unions and GfK-MODE research teams during the training and field work helped in rectifying issues in the questionnaire and in clarifying issues with certain questions to the investigators, supervisors & FEs, thus improving the quality of data collection. The processes of translations, back translations, cross verification, pilot testing and finalization of local language versions took more time than estimated. Due to less number of TB diseased persons in each PSU, it was difficult for field teams to select required number of target respondents especially from the urban areas. Problem in collection of Census Enumerated Blocks (CEB) maps from census office. Officials informed that current CEB maps were not in use now because they were in a process of launching new digital CEB maps Not able to find two Health service Providers in a PSU as most of the people approached District Hospital for any type of problem.
16
CHAPTER 2 GENERAL POPULATION This section of the chapter presents the demographic and socio-economic characteristics of the respondents and their households, interviewed during the survey in selected 15 states of India. The socio-demographic profile presented in this report is based on the de-jure population, who is the usual resident of the household. Only individuals who were above the age of 18 years were included in the survey. 2.1 DEMOGRAPHIC CHARACTERSTICS OF THE RESPONDENTS Age and sex are the basic demographic characteristics which have an important role in study of family health, individual health and disease prevalence. Table 2.1 shows the zone wise distribution of the respondents from the General Population by sex, age, education status, marital status and occupation. A total of 4562 persons representing the general population were interviewed during the survey in which 2320 were males and 2242 were females. Efforts were made to interview almost equal number of male and females from each PSU. There was equal coverage of male and females in all four zones. There were no significant variations in the age group of respondents from each zone. The mean age of the respondents was between 34-36 years in all four zones. Education is an important socio economic indicator in analysis for its nature of association with any disease and other behavioural aspects. The survey collected information on the educational status of the respondents during the survey. Around 30% per cent of the respondents were found to be illiterate, with lower levels in the southern zone (19 %). Most of the respondents who were literate reported having studied to primary and secondary levels. Very few respondents (5%) reported having studied up to graduation. Marriage, in the Indian context, has a bearing on several social, demographic and health outcomes. Around 85% of the respondents were married and 12% were unmarried. Very few of the respondents were widowed and separated. The marital status of respondents was similar across all the four zones. With respect to occupation, majority of the respondents were either wage labourers (26%) or were involved in agriculture (15%) or were housewives (30.8). There were some minor variations in the profile of the occupation of the respondents across all zones.
17
Table 2.1: Socio demographic characteristics of respondents from the General Population
Characteristics Sex Male Female Age 18-25yrs 26-35yrs 36-45yrs 46+ Mean Age (in yrs) Education Illiterate Literate but no formal education Less than primary Primary Secondary Senior Secondary Graduation and above Marital Status Married Unmarried Divorced Widowed Separated Occupation Wage laborer Skilled worker Self employed Service (Govt. & Private) Business Agriculture/cultivator Unemployed House wife Students Petty Traders Total Sample 208 52 44 47 15 193 24 417 59 8 1067 20 5 4 4 1 18 2 39 6 1 267 40 62 78 54 208 40 417 63 5 1234 22 3 5 6 4 17 3 34 5 0 345 81 74 81 30 211 29 292 45 14 1202 29 7 6 7 3 18 2 24 4 1 341 139 49 44 43 66 61 278 31 7 1059 32 13 5 4 4 6 6 26 3 1 1161 312 229 250 142 678 154 1404 198 34 4562 26 7 5 6 3 15 3 31 4 1 892 144 1 29 1 84 14 0 3 0 1033 161 1 39 0 84 13 0 3 0 1031 132 2 37 0 86 11 0 3 0 901 110 4 44 0 85 10 0 4 0 3857 547 8 149 1 85 12 0 3 0 355 86 58 167 208 126 67 33 8 5 16 20 12 6 494 134 82 155 174 122 73 40 11 7 13 14 10 6 344 121 110 216 243 119 49 29 10 9 18 20 10 4 201 87 182 312 168 57 52 19 8 17 30 16 5 5 1394 428 432 850 793 424 241 31 9 9 19 17 9 5 259 285 358 165 34 24 27 34 16 250 372 373 239 35 20 30 30 19 217 405 358 222 35 18 34 30 19 173 284 296 306 36 16 27 28 29 899 1346 1385 932 35 20 30 30 20 North N 531 536 (%) 50 50 N 617 617 East (%) 50 50 N 635 567 West (%) 53 47 South N 537 522 (%) 51 49 N 2320 2242 Total (%) 51 49
18
The profile of the respondents indicates that they are likely to be representative of the General Population whose characteristics is described in the various other sources (Census, NHFS-III). 2.2 HOUSEHOLD CHARACTERISTICS AND ASSETS Housing Amenities such as Access to safe drinking water, fuel used for cooking, type of house, ownership status and household assets also have significant bearing particularly, on knowledge, attitude, practices and the vulnerability to any disease, mortality and physical and mental health of an individual. Table 2.2 shows the zone wise distribution of type of house, drinking water and fuel used for cooking by the households of the respondents. For the purpose of categorization of quality of housing into Kachha, Pucca and Semi pucca, the type of roof [made of concrete, metal sheet or straw/bamboo], type of wall [concrete, wooden, bamboo/mud] and type of floor [ concrete, wooden, clay] are considered. Pucca [roof, wall and floor made up of concrete], semi-pucca[either the roof, wall or the floor is made up of non-concrete substance] and kachha[the roof, wall and floor is made up of non-concrete] is the highest to lowest quality of housing. Around 60% of respondents were staying in either Semi Pucca or Kachha houses whereas nearly 40 % of them were staying in Pucca house. The proportion of the respondents living in these three types of houses varied across the zones with the respondents in the southern zone less likely to be staying in a kuccha house. The percentage of Pucca House varies from 54 percent in north to only 35 percent in Eastern and western region. More rural housing structures were Kuchha while more urban were pucca (not shown in table). The vast majority of the respondents (81%) owned a house and this proportion is highest in northern region (90%) and lowest in western region (61%) On asking respondents for their main source of drinking water for their households, majority of the people (84%) had access to improved source of drinking water (Private & Public tap and hand pump).The most common source of drinking water for people in southern zone was Public tap whereas in northern and eastern zone, people used private hand pump for collection of drinking water. Usage of solid cooking fuel causes indoor air pollution by emanating Smoke and is a serious health hazard. Solid cooking fuels include coal/lignite, charcoal, wood, straw, shrubs, grass, agricultural crop waste and dung cakes. Around 58 percent of the households of the respondents used fire wood for cooking food. Overall, at national level, 25% of households used LPG/Natural Gas for cooking.
19
However, its proportion was highest in the southern zone where 34% of General Population reported to have used LPG gas for cooking purpose, while the proportion was found to be lowest in Northern region (12%). Table 2.2: Household Characteristics of Respondents from the General Population
Characteristics Type of House Pucca Semi Pucca Kutcha Ownership of House (Yes, Own) Source of Drinking Water Private Tap Private Hand Pump Public Tap Public Hand Pump Tube well Supply tanker Well/River/Pond Type of Fuel Wood Dung Cakes LPG(Gas)/Natural Gas Straw/Shrubs/Grass Agriculture Crop Waste Electricity Coal/Lignite Kerosene Charcoal Bio-gas Others Total (respondents) 680 210 131 30 29 3 2 2 5 2 6 1067 64 20 12 3 3 0 0 0 1 0 1 435 266 298 142 72 2 2 12 7 6 2 1234 35 22 24 12 6 0 0 1 1 1 0 820 38 358 2 1 9 13 93 4 15 1 1202 68 3 30 0 0 1 1 8 0 1 0 725 0 355 7 5 8 4 18 0 13 0 1059 69 0 34 1 1 1 0 2 0 1 0 2660 514 1142 181 107 22 21 125 16 36 9 4562 58 11 25 4 2 0 0 3 0 1 0 308 355 211 173 2 2 16 29 33 20 16 0 0 2 197 410 102 305 169 7 43 16 33 8 25 14 1 4 300 101 371 285 124 12 0 25 8 31 24 10 1 0 202 47 405 110 264 29 0 19 4 38 10 25 3 0 1007 913 1089 873 559 50 59 22 20 24 19 12 1 1 North N 582 245 240 957 % 55 23 23 90 N 443 391 400 1097 East % 36 32 32 89 West N 413 309 480 732 % 34 26 40 61 South N 471 492 96 917 % 45 47 9 87 N 1909 1437 1216 3703 Total % 42 32 27 81
The socio-economic status of households of respondents can be indirectly assessed in terms of possession of consumer durables. Around two third of households of respondents owned mobile phones, electric fan followed by bicycle and colour television. Car/Motorcycle and scooter were owned by 25% of the households of the respondents. The proportion of consumer durable items was found to be higher in southern region as compared to the other three regions.
20
Regarding the monthly income of the households of the respondents; nearly two thirds of the respondents reported that their monthly household income was less than Rs 4000. A higher proportion of respondents from the southern zone informed of having a household monthly income of Rs 4000 or more when compared to other zones. Only about 5% of the respondents reported to have their household income of more than 10,000 per month. A standard of living index was created by the NFHS as a summary household measure (IIPS, 2000). It is composed of 27 items, including consumer durables, agricultural machinery, housing conditions and access to basic services (water, light, fuel, etc). These durables were given weights. The details of weights given to each component are provided in the annexure. The index is calculated by summing the weights which have been developed by the International Institute of Population Sciences NFHS research team in India. These weights are based upon their considerable knowledge of the relative significance of ownership of these items, rather than on a more formal analysis. Overall, equal number of respondents (around 33-36%) belonged to Low SLI (0-14), and medium SLI (14-25). Around thirty percent of the respondents belongs to High SLI (25 and above). In Eastern region, around half of the respondents belonged to Low SLI where as its proportion is quite less in southern region (Less than 20%). Table 2.3: Household assets owned by respondents of the general population
Characteristics Household Assets(% owned) Electricity Mattress Pressure cooker Chair cot or Bed Table Electric Fan Radio Or Transistor Black & white Television Colour Television Sewing Machine Mobile Telephone Any other Type of Phone Computer Refrigerator Watch or Clock Bicycle Motorcycle or Scooter Animal drawn cart Car North N % 732 69 784 74 439 41 634 59 1048 98 481 45 620 58 196 18 108 10 434 41 389 37 751 70 190 18 34 3 251 24 881 83 801 75 318 30 146 14 47 4 East N % 740 60 534 43 455 37 788 64 1033 84 537 44 441 36 280 23 94 8 399 32 205 17 652 53 166 14 95 8 227 18 832 67 626 51 213 17 12 1 38 3 West N % 1078 90 680 57 512 43 861 72 946 79 448 37 803 67 193 16 97 8 642 53 225 19 641 53 221 18 47 4 175 15 986 82 606 50 286 24 114 10 28 2 South N % 1036 98 586 55 390 37 815 77 689 65 541 51 918 87 171 16 44 4 860 81 132 13 736 70 192 18 29 3 193 18 872 82 579 55 353 33 57 5 16 2 Total N % 3586 79 2584 57 1796 39 3098 68 3716 82 2007 44 2782 61 840 18 343 8 2335 51 951 21 2780 61 769 17 205 5 846 19 3571 78 2612 57 1170 26 329 7 129 3
21
Characteristics Water Pump (For agricultural Use) Thresher (For agricultural Use) Tractor(For agricultural Use) Standard of Living Index Low SLI Medium SLI High SLI Household Income Less than Rs. 2000 Rs. 2000 - Rs. 4000 Rs. 4001 - Rs. 8000 Rs. 8001 - Rs. 10,000 Rs. 10,001 and above Don't know Total
North 217 68 88 346 326 395 20 6 8 32 31 37
East 65 21 8 632 299 303 5 2 1 51 24 25
West 136 31 35 460 411 331 11 3 3 38 34 28
South 225 5 35 198 510 351 21 1 3 19 48 33
Total 643 125 166 1636 1546 1380 14 3 4 36 34 30
292 33 419 39 194 17 83 3 74 3 5 4 1067
364 27 473 39 174 18 114 8 90 7 19 1 1234
334 30 376 38 282 14 92 9 57 7 61 2 1202
249 28 368 31 232 24 153 8 35 5 22 5 1059
1239 27 1636 36 882 19 442 10 256 6 107 2 4562
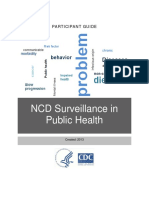
Figure 2.1: Proportion of Respondent Households Considered to be of Low SLI stratified by State
The figure shows that as high as 60% of Households of the respondents belonged to low SLI in Chhattisgarh and Bihar, while only 1-5 % households in Mizoram and Punjab belonged to Low SLI. This coincides with the occupational categories, the sample population belonged to.
22
2.3
KNOWLEDGE, ATTITUDE AND PRACTICES This section presents the existing knowledge, attitude and practices of the respondents during the survey. The survey collected information on the awareness on cause and treatment of TB, diagnosis, symptoms in TB patients, and source of treatment. Heard of TB When respondents were asked about whether they heard about TB, 84% of them responded in the affirmative. The proportion of respondents who had heard of TB was higher among respondents from urban areas when compared to rural areas and among males when compared to females. It was less among respondents who were illiterate, those aged more than 55 years, those from the east zone and south zones (Table 2.4). Table 2.4: Characteristics of respondents who had heard of TB
No N Heard of TB? Setting Rural Urban Sex Female Male Age group 18 to24 years >25 to <35 years >35 to <45 Years >45 to <55 Years >55 years Literacy Status Illiterate Less than Primary Literate but no formal education Primary but less than Secondary Secondary but less than Senior Secondary Senior Secondary but not 404 77 82 118 39 10 29 18 19 14 5 2 990 355 346 732 754 414 71 82 81 86 95 98 1394 432 428 850 793 424 100 100 100 100 100 100 83 209 217 170 60 12 17 15 18 27 609 1057 1210 787 160 88 84 85 82 73 692 1266 1427 957 220 100 100 100 100 100 436 303 19 13 1806 2017 81 87 2242 2320 100 100 629 110 19 9 2759 1064 81 91 3388 1174 100 100 739 % 16 N 3823 Yes % 84 N 4562 Total % 100
23
No N Heard of TB? Graduate Graduation and above Zone East North South West 184 46 286 223 15 4 27 19 1050 1021 773 979 739 9 % 16 4 N 3823 232
Yes % 84 96 85 96 73 81 N 4562 241 1234 1067 1059 1202
Total % 100 100 100 100 100 100
Knowledge about the symptoms of TB Tuberculosis is an infectious disease which predominantly affects the lungs although any other part of the body can also get affected. The most common symptoms are cough with or without expectoration for more than 2 weeks, chest pain, weight loss, and fever and weight loss. On asking the respondents who had heard about TB (n=3823) on their awareness on the symptoms of tuberculosis, the responses provided by them is as given below. Table 2.5: Awareness of the symptoms of TB among the respondents who had heard of TB disaggregated by zones (N=3823)
Zone TOTAL Total A cough of 2 weeks Coughing up blood Fever Pain in the chest Weight loss Night sweat Loss of appetite Cough with cold Dont know 3823 % 74 45 33 30 17 2 9 4 11 NORTH 1021 % 68 39 20 19 9 0 8 5 15 EAST 1050 % 73 57 42 46 9 2 6 2 12 WEST 979 % 74 41 34 28 26 3 14 8 9 SOUTH 773 % 84 42 40 24 28 6 9 1 4
* Percentages can add up to more than 100% as more than one response possible Nearly three fourth of the respondents who had heard of TB knew that the major symptom of TB is cough of two weeks or more. The proportion was highest (84%) in south zone and least (68%) in the north zone. The other major symptoms identified included coughing up blood (45%), fever (33%) and chest pain (30%). Overall at the National Level 11% of the respondents did not know of any symptom at all.
24
The proportion of respondents without any knowledge of any of the symptoms of TB was highest in the north zone (15%) and least in the south zone (4%). Knowledge of the mode of transmission The respondents who had heard of TB were asked about the mode of spread of TB from person to person. The responses are shown in Table 2.6. Nearly 60% of the respondents knew that it spreads through air when the infected person coughs or sneezes. There were wide variations in the proportion of respondents who knew that TB spreads through air among the respondents from different zones. Nearly 80% of the respondents in the southern zone informed that it spreads through air whereas only about half of the respondents in the north and east zones informed that it spreads through air. Many other incorrect modes of transmission such as spread through sharing of food (31%), through sharing of bed/clothes (14%) and through handshake were also identified (18%). These misconceptions about the spread of TB in the community may aid in stigma and discrimination if un-corrected. Nearly 20% of the respondents did not know any mode by which TB spreads from person to person. The proportion of respondents who did not know of any mode of TB transmission was highest in the east zone (25%) when compared to other zones and it was least in south zone of the country (9%). Table 2.6: Awareness of the mode TB transmission among the respondents who had heard of TB disaggregated by zones (N=3823)
Zone TOTAL Number of respondents Through the air when the infected person cough or sneeze Through sharing food with a person with TB By sharing bed/clothes with a person with TB Through handshake with a person with TB Dont Know / Not aware 3823 % 60 31 14 18 20 NORTH 1021 % 52 31 12 16 22 EAST 1050 % 52 35 10 20 25 WEST 979 % 61 25 12 16 20 SOUTH 773 % 78 32 22 17 9
* Percentages can add up to more than 100% as more than one response possible
25
Knowledge on who are more prone for TB Disease The respondents who had heard of TB were asked about who are more prone for the development of TB Disease in the community and the responses given are shown in Table 2.7. Table 2.7: Respondents opinion on the people who are more prone for TB in the community disaggregated by zones (N=3823)*
Total Number of Respondents People who are more prone for TB Smokers Those living in unhygienic condition Alcoholics Family members of TB persons Exposed to cough and cold for long time Poor people Malnourished Children Women HIV positive persons Dont Know 3823 % 43 41 28 20 18 16 15 4 3 4 14 NORTH ZONE 1021 % 34 42 11 16 16 16 7 2 3 1 16 EAST ZONE 1050 % 52 41 44 12 12 15 20 3 2 4 17 WEST ZONE 979 % 46 43 30 17 22 12 5 3 2 3 16 SOUTH ZONE 773 % 38 39 26 42 22 21 28 12 3 10 3
* Percentages can add up to more than 100% as more than one response possible Majority of the respondents (more than 40%) identified smokers and those living in un-hygienic conditions are more prone for TB Disease. The other persons identified to be more prone for TB disease are alcoholics, family members of TB persons. Surprisingly only 4% of the respondents identified HIV positive persons as more prone for TB disease. This could be because the respondents would have seen more persons with the other conditions getting the TB disease than HIV positive persons due to relative low prevalence of HIV in the community. Knowledge on the mode of diagnosis of TB The respondents were asked whether they were aware of any methods for the diagnosis of Tuberculosis (investigations) and the responses given by them are shown in Table 2.8.
26
Table 2.8: Respondents awareness of the mode of diagnosis for tuberculosis stratified by Zone
TOTAL Number of respondents Investigations Sputum Smear Test X-Ray Any Other (blood, urine, ultrasound etc.,) Dont know 3823 % 66 61 10 15 NORTH ZONE 1021 % 62 57 6 18 EAST ZONE 1050 % 67 64 24 15 WEST ZONE 979 % 71 59 8 15 SOUTH ZONE 773 % 62 66 4 13
Nearly two thirds of the respondents mentioned that TB can be diagnosed by sputum examination. The proportion of respondents who identified the investigation as sputum examination remained more or less the same across the different zones. Nearly 60% of the respondents also identified X-Ray as the mode of diagnosis for TB. Overall 15% of the respondents did not know of any investigations for tuberculosis. The proportion of respondents without any knowledge of the methods for diagnosis of TB remained more or less the same across various zones. Knowledge about the curability of the TB disease In order to elicit the information on the curability of TB disease, the respondents were asked whether they consider TB as a serious life threatening disease, whether they consider TB a curable disease, the best form of treatment and the duration of treatment. The responses are given in tables 2.9 and 2.10. Table 2.9: Opinion of the respondents on the seriousness of the TB disease and about curability
TOTAL Number of respondents Yes, Serious life threatening disease Consider TB as a curable disease Yes, completely Yes, Partially No Dont Know 88 8 1 3 87 9 2 2 88 9 1 2 88 7 2 3 87 7 2 4 3823 % 77 NORTH ZONE 1021 % 91 EAST ZONE 1050 % 75 WEST ZONE 979 % 75 SOUTH ZONE 773 % 63
27
Three fourths of the respondents considered TB as a serious life threatening disease. The proportion of respondents of respondents who considered TB as a life threatening disease was highest in north zone (91%) and a relatively lesser proportion of the respondents from the south Zone (63%). Nearly all respondents (96%) considered TB as a curable disease. The proportion of respondents who considered that TB is not curable or who did not know that TB is curable was only 4%. Table 2.10: Best treatment for TB (among those who considered TB as a curable disease completely or partially) and the duration of treatment
TOTAL Number of respondents Allopathic medicines DOTS (if specific response given) Herbal Remedies Home Remedies Ayurvedic Homeopathy Other Dont Know Duration of TB treatment 4 weeks or less 1-5 months 6-8 months More than 8 months Dont Know 3 16 46 8 26 2 12 49 11 25 4 10 45 9 32 4 19 54 7 16 2 27 35 4 31 3654 % 55 16 2 2 2 3 4 16 NORTH ZONE 980 % 59 12 0 1 1 3 4 20 WEST EAST ZONE ZONE 1020 % 61 12 0 4 0 1 1 18 927 % 35 30 2 1 6 4 10 11 SOUTH ZONE 727 % 64 10 9 2 0 3 1 10
Nearly 70% of the respondents mentioned that allopathic medicine or DOTS as the best treatment for tuberculosis and this proportion remained same more or less across all zones. Nearly 12 % of the respondents considered non-allopathic form of medicines as the best form of treatment for tuberculosis.16% of the respondents did not know of the best treatment for TB and this proportion was highest in the north zone (20%) and least in the south zone (10%). With respect to duration of TB treatment nearly half of the respondents (46%) knew that the duration of treatment is for 6-8 months. It was highest among the respondents of the west zone (54%) when compared to south zone (35%). One fourth of the respondents did not know of the duration of TB treatment. This was least in the West Zone (16%) and highest in the east zone (32%).
28
Knowledge on DOTS The respondents who have heard of TB were asked whether they heard of the term DOTS. The response to this question is given in Table 2.11. Table 2.11: Proportion of respondents who had heard of the term DOTS
TOTAL Total number of respondents Heard of Dots Yes No 3823 % 28 72 NORTH ZONE 1021 % 24 76 EAST ZONE 1050 % 29 71 WEST ZONE 979 % 40 60 SOUTH ZONE 773 % 16 84
Only 28% of the respondents who had heard of TB had heard of the term DOTS. The proportion of respondents who had heard of DOTS was highest in the west zone (40%) and least in the south zone (16%). Of the respondents who had heard of the term DOTS (n=1060), 80% knew that TB Treatment is available free of cost under DOTS (Table 2.12). Table 2.12: Proportion of respondents who had heard of DOTS knew that TB treatment is available free of cost under DOTS
TOTAL Total number of respondents Heard of free TB treatment Yes No Dont know 1060 % 80 12 8 NORTH ZONE EAST ZONE WEST ZONE SOUTH ZONE 240 % 80 9 11 304 % 86 9 5 392 % 77 16 7 124 % 75 15 10
Self-perception about susceptibility to TB Disease (a measure of the attitude) The respondents when asked whether they perceive themselves to be susceptible to TB disease, overall 35% felt that they are susceptibility to TB Disease. Only 1% of the respondents of the south zone felt that they are susceptible to TB Disease and 89% felt that they are not, whereas in other zones the proportion was relatively higher.
29
Table 2.13: Self-perception of the susceptibility to develop TB disease among the respondents
TOTAL Number of respondents Can you have TB? Yes No Dont know/Cant Say 3823 % 35 54 11 NORTH ZONE 1021 % 56 32 12 EAST ZONE WEST ZONE SOUTH ZONE 1050 % 41 42 17 979 % 32 62 5 773 % 1 89 9
Among respondent who informed that they are not susceptible to TB disease, the reasons for their lack of susceptibility to develop TB disease is given in Table 2.14. Table 2.14: Major Reasons why respondents felt that they cannot develop TB
TOTAL Total No. of respondents Reasons I am healthy and strong I do not fall sick easily No one in my family has suffered from TB I have not come in contact with a patient I stay away from poor/sick people 2063 % 76 36 37 10 2 NORTH ZONE 326 % 60 20 45 6 2 EAST ZONE 436 % 88 36 36 5 0 WEST ZONE 610 % 82 37 23 8 1 SOUTH ZONE 691 % 71 42 46 16 2
Cough among respondents (a measure of practices) Nearly 10% of the overall respondents were having cough or have had cough for more than 2 weeks in the past 2 months (Table 2.15). This varied between 12% in the east Zone to 8% in the west and south zones. Out of those with cough of more than 2 weeks, only about 30% had visited any health care provider for seeking medical care or sputum examination. The proportion was highest in the south Zone (55%) and least in the east zone (17%). Overall nearly 70% of the respondents with cough of more than 2 weeks had not sought care from any source.
30
Table 2.15: Cough among respondents and their care seeking behaviour
Total 4562 N (%) Respondents having/having had cough of 2 weeks or more in the past 2 months Out of those with cough of more than 2 weeks, number who visited a health facility for seeking care or sputum examination North zone 1067 N (%) East zone West zone South zone 1234 1202 1059 N (%) N (%) N (%
Number of respondents
437 (10)
114 (11)
149 (12)
92 (8)
82 (8)
137 (31)
29 (25)
25 (17)
38 (41)
45 (55)
Sources of TB related information The survey further probed on the sources of information for their TB related knowledge, most preferred source of information and about any health personnel visiting them to provide information on TB (interpersonal communication). The respondents revealed that their main source for TB related information like cause, symptoms & prevention of Tuberculosis; were Television (37%) and Doctors (36%). Newspaper and magazines and Hoardings were mentioned by about one fourth of respondents as the next major sources of information. More than a quarter of respondents also mentioned interpersonal communication as their source of information on different TB related issues (Table 2.16). Table 2.16: Source of TB related information of the respondents
Characteristics Existing Source of TB related info* Television Hospital /Doctors Interpersonal Communication Newspaper/Magazine/Hoardings/ Radio Preferred Source of TB related info Hospital /Doctors Television Newspaper/Magazine/Hoardings/ Local Health Workers ( ASHA, ANM etc) Interpersonal Communication North N % 158 15 545 51 244 23 252 24 107 10 426 328 275 245 259 40 31 26 23 24 East N % 465 38 518 42 592 48 428 35 164 13 771 458 404 525 570 62 37 33 43 46 West N % 665 55 340 28 220 18 421 35 144 12 545 734 451 206 112 45 61 36 17 9 South N % 387 37 262 25 177 17 315 30 79 7 443 487 327 330 68 42 46 31 31 6 Total N % 1675 37 1665 37 1233 27 1416 31 494 11 2185 2007 1457 1306 1009 48 44 31 29 22
* Percentages may add up to more than 100% as multiple responses possible When asked about the preference of the source of TB related information, the most preferred source of information was mentioned as Hospitals/Doctors (48%) and Television (44%).
31
Around 43 49 % of respondents felt that information on TB provided by Hospitals and Doctors were more reliable than any other sources. Less than 1/3rd of the respondents preferred local health workers or interpersonal communication as the source of TB related information. When asked about whether anybody visited their locality or their home to give health related message in the past 2 years, only 4 % of the respondents mentioned in the affirmative (Table 2.17). The proportion was more or less similar. Nearly 96% of the respondents in the north zone confirmed that nobody has visited their homes or locality to provide TB related information, however this proportion was less in the east, west and south zones of the country. Table 2.17: Respondents reply to Visit by any individual to provide information on Tuberculosis
TOTAL Number of respondents 4562 Anybody visited their locality to discuss TB related information Yes No Dont know % 4 87 9 1067 % 3 96 2 1234 % 5 81 14 1202 % 4 88 8 1059 % 3 84 13 NORTH ZONE EAST ZONE WEST ZONE SOUTH ZONE
Among the respondents who confirmed anybody visiting their locality in the last two years, when asked who it was and what information was provided, the responses are given in the following table 2.18. Table 2.18: Respondents response to the query on visit by people to provide TB related information
Characteristics Total number of respondents Visit of people to provide TB related Information (% responded yes) Who visited? (Only those visited): AWW/ASHA/HW/ANM Government Doctor Private Doctor Type of Information provided* Symptoms of Tuberculosis 16 59 22 36 18 38 31 84 87 50 20 10 4 74 37 15 57 11 3 92 18 5 43 11 2 90 23 4 35 14 2 100 38 5 159 46 11 91 26 6 North 1067 N 27 % 3 East 1234 N 62 % 5 West 1202 N 48 % 4 N 37 South 1059 % 3 Total 4562 N 174 % 4
32
Characteristics Prevention from Tuberculosis Cure for Tuberculosis DOTS Place of Treatment Information on prevailing myths about TB patients
North 12 9 6 7 0 44 33 22 26 0
East 32 26 2 12 0 52 42 3 19 0
West 22 9 4 12 4 46 19 8 25 8
South 27 18 7 10 4 73 49 19 27 10
Total 93 62 19 41 8 54 36 11 24 5
Table 2.19: Summary of key Indicators* on TB Related Awareness at the project level stratified by Zone
Zone TOTAL Number of respondents Key indicators Heard of TB Having knowledge that cough of > 2 weeks is TB Having knowledge that TB is caused by bacteria/germs and is transmitted through air Having knowledge that TB can be diagnosed by sputum examination Having knowledge that TB is curable Having knowledge that the duration of TB treatment is 6-8 months Have heard of DOTS Know that TB treatment is free under DOTS Respondents having/having had cough of 2 weeks or more in the past 2 months Out of those with cough of more than 2 weeks, number who visited a health facility for seeking care or sputum examination 4562 N (%) 3823 (84) North 1067 N (%) 1021 (96) East 1234 N (%) West 1202 N (%) N South 1059 (%)
1050 (85)
979 (81)
773 (73)
2829 (69)
694 (65)
767(62)
724 (60)
649 (61)
2282 (50) 2253 (55) 3670 (80) 1681 (37) 1070 (23)
533 (50) 633 (59) 980 (92) 480 (45) 245 (23)
550 (45) 704 (57) 1019 (83) 459 (37) 305 (25)
595 (50) 695 (58) 930 (77) 501 (42) 392 (33)
604 (57) 479 (45) 727 (69) 254 (24) 124 (12)
848 (19)
192 (18)
261 (21)
302 (25)
93 (9)
437 (10)
114 (11)
149 (12)
92 (8)
82 (8)
137 (31)
29 (25)
25 (17)
38 (41)
45 (55)
* The denominators for all indicators is the total number of persons interviewed
33
CHAPTER 3 TB DISEASED PERSONS This section presents the demographic and socio-economic characteristics of households of self-reported TB Diseased Population, interviewed during the survey in selected 30 districts from 15 states of India. The survey collected information on agesex composition, marital status, education status, and household characteristic and housing assets. The socio-demographic profile presented in this report is based on the de-jure population, who is the usual resident of the household. The respondents were self-reported TB diseased persons known to be on Anti-TB Drug at present or known to have taken anti-TB drugs for any duration in the past 12 months. The data was collected from the TB diseased persons identified from the line listing process. A total of 752 TB diseased persons were identified and the field teams collected data from a total of 609 (81%) TB diseased persons, selected from the PSUs by house listing procedure. The distribution of the selected patients is given in Table 3.1. Table 3.1: Distribution of the patients identified during the course of the survey disaggregated state wise
State Name Andhra Pradesh Bihar Chhattisgarh Haryana Karnataka Kerala Maharashtra Mizoram Madhya Pradesh Orissa Punjab Rajasthan Tamil Nadu Uttar Pradesh West Bengal Total Rural 5 155 0 44 0 16 42 0 5 0 2 21 4 75 25 394 Tribal 0 2 4 0 30 6 28 0 0 18 0 0 0 0 0 88 Urban 0 1 0 0 0 0 7 0 0 0 0 0 0 3 1 12 Unknown 1 10 1 0 0 2 14 1 6 8 0 6 41 21 4 115 Total 6 168 5 44 30 24 91 1 11 26 2 27 45 99 30 609
Nearly two thirds (65%) of the patients were from rural areas, 14% were from tribal areas, 19% from urban areas and in 2% cases, the locality could not be ascertained.
34
3.1
DEMOGRAPHIC CHARACTERISTICS OF TB DISEASED PERSONS Table 3.2 shows demographic characteristics of the TB diseased persons disaggregated by Zones. Out of the 609 TB diseased persons interviewed, 389 (64%) were males and 220 (36%) were females. The proportion of males varied across the zones ranging from 72% in the south zone to 59% in the east Zone. On the whole less than 10% of the surveyed TB diseased persons aged less than 18 years and 13-20 % were found in the age group of 19-25, 26-35 and 35-45 years. Majority (38%) of the TB patients were aged more than 45 years. The situation was similar in all the four zones except western zone, where large number of TB diseased persons were also found in age bracket of 26-35 years. Level of education considered as an important social indicator and plays significant role in interpreting the behaviour aspects of the respondents, it also has strong association with level of knowledge. The survey collected information on the educational status of the TB diseased persons. another 10% were literate but received no formal education. More proportion of TB patients in the southern zone was literate when compared to other zones. Around 77 % of the TB diseased persons were married and 19% were unmarried. Very few of the interviewed TB patients were widowed. The situation is somewhat similar in all the four zones. In terms of occupation, more than half of them were either daily wage labourers or worked in the agriculture and more than half of the women were housewives. Table 3.2: Characteristics of TB Diseased Persons
Characteristics Sex Male Female Age < 18 yrs 19-25yrs 26-35yrs 36-45yrs 46+ Education Illiterate Literate but no formal education Less than primary Primary Secondary Senior Secondary Graduation and above North N % 96 66 49 34 4 20 36 33 52 79 8 10 18 22 4 4 3 14 25 23 36 55 6 7 12 15 3 3 East N % 139 59 96 41 30 34 45 44 82 106 26 30 32 29 9 3 13 15 19 19 35 45 11 13 14 12 4 1 West N 78 46 7 17 36 28 36 50 16 17 26 11 3 1 % 63 37 6 14 29 23 29 40 13 14 21 9 2 1 South N % 76 72 29 28 5 11 14 16 59 29 14 25 25 9 3 0 5 11 13 15 56 28 13 24 24 9 3 0 Total N % 389 64 220 36 46 82 131 121 229 264 64 82 101 71 19 8 8 13 22 20 38 43 11 14 17 12 3 1
35
Characteristics Marital Status Married Unmarried Divorced Widowed Separated Occupation Wage labourer Skilled worker Self employed Service (Govt. & Private) Business Agriculture/cultivator Unemployed House wife Student / Handicapped Total
North 121 15 0 9 0 46 8 5 1 1 24 12 40 8 145 84 10 0 6 0 32 6 4 1 1 17 8 28 6
East 169 47 1 18 0 57 10 7 5 9 43 20 54 30 235 72 20 0 8 0 24 4 3 2 4 18 9 23 13
West 102 19 0 3 0 56 8 2 2 1 26 5 15 9 124 82 15 0 2 0 45 7 2 2 1 21 4 12 7
South 81 16 0 7 1 39 11 2 1 5 8 16 18 5 105 77 15 0 7 1 37 11 2 1 5 8 15 17 5
Total 473 97 1 37 1 198 37 16 9 16 101 53 127 52 609 78 16 0 6 0 33 6 3 2 3 17 9 21 9
3.2
HOUSING CHARACTERISTICS AND ASSETS Housing Amenities such as access to safe drinking water, fuel used for cooking, type of house, ownership status and household assets also have significant bearing particularly, on incidence of any disease, mortality and physical and mental health of an individual. Table 3.3 shows the zone wise distribution of type of house, drinking water and fuel used for cooking by TB diseased persons. The housing of TB patients can be described based on the quality into Kachha, Pucca and Semi pucca houses [described in detail in Chapter 2]. There were distinct zone wise variation observed in the housing structure of TB diseased persons. The percentage of TB patients living in Pucca souse varies from 47% in south zone to only 19% in Eastern region. More housing of respondents from rural areas were Kuchha while those from the urban were pucca. The vast majority of the respondents (83.2%) owned a house and this proportion is highest in southern region (92%). On asking TB diseased persons for their main source of drinking water, majority of the people (90%) had access to improved source of drinking water (Private & Public tap and hand pump).The most common source of drinking water for people in southern zone was Public tap whereas in western zone, people used private hand pump for collection of drinking water.
36
Smoke from solid cooking fuels is a serious health hazard and indoor air pollution is a definite risk factor for TB. Solid cooking fuels include coal/lignite, charcoal, wood, straw, shrubs, grass, agricultural crop waste and dung cakes. As many as 56% of the households of TB diseased persons used fire wood for cooking while 21 % cooked their food with dung cakes (mainly from rural areas). Overall, on National level, only 12% of households used LPG/Natural Gas for cooking. However, its proportion was highest in the southern zone where 40% of TB diseased person reported to have used LPG gas for cooking purpose in their households. Table 3.3: Household Characteristics of TB Diseased Persons
Characteristics Type of House Pucca Semi Pucca Kachha Ownership of House (% Own) Source of Drinking Water Private Tap Private Hand Pump Public Tap Public Hand Pump Tube well Supply tanker Well/River/Pond Type of Fuel Electricity Wood Coal/Lignite Kerosene LPG(Gas)/Natural Gas Bio-gas Dung Cakes Agriculture Crop Waste Straw/Shrubs/Grass Total North N % 39 27 50 35 56 39 126 32 34 45 33 1 0 0 87 22 24 31 23 1 0 0 East N 67 84 84 192 18 108 9 63 26 0 11 0 79 1 2 17 3 93 16 28 235 % 29 36 36 82 8 46 4 27 11 0 5 0 34 0 1 7 1 40 7 12 West N % 24 19 36 29 64 52 93 22 13 29 36 3 5 16 75 18 11 23 29 2 4 13 South N % 50 48 45 43 10 10 97 16 3 54 5 12 0 15 1 63 0 1 42 4 0 0 0 105 92 15 3 51 5 11 0 14 1 60 0 1 40 4 0 0 0 Total N % 180 30 215 35 214 35 508 88 158 137 137 42 5 42 1 341 3 12 76 7 131 27 37 609 83 14 26 23 23 7 1 7 0 56 1 2 13 1 22 4 6
0 0 85 59 2 1 0 0 7 5 0 0 35 24 11 8 9 6 145
0 0 114 92 0 0 9 7 10 8 0 0 3 2 0 0 0 0 124
Household Assets (Table 3.4) The socio-economic status of households can be indirectly assessed in terms of possession of consumer durables. More than 50% of households of TB diseased persons owned a bicycle and mobile phones, followed by electric fan and colour television in 30-40% of households. Car/Motorcycle and scooter were owned by 12% of the household.
37
The proportion of consumer durable items was found to be higher in southern region as compared to the other three regions. Regarding the monthly income of the households of TB diseased persons; more than 40% of them reported a monthly income in the range of Rs. 2000-4000 and a slightly lower proportion in the range of less than Rs. 2000 per month. Only 2% of the respondents reported to have a monthly household income of more than 10,000 per month. There were no distinct Zone-wise variations in the monthly income of the households of TB diseased persons. A standard of living index was created by the NFHS as a summary household asset (IIPS, 2000). It is composed of 27 items, including consumer durables, agricultural machinery, housing conditions and access to basic services (water, light, fuel, etc). These durables were given some weights. The details of weights given to each component are provided in the annexure. The index is calculated by summing the weights which have been developed by the International Institute of Population Sciences NFHS research team in India. These weights are based upon their considerable knowledge of the relative significance of ownership of these items, rather than on a more formal analysis. Majority of the TB patients (around 55%) belonged to the Low SLI (0-14), however their proportion was high in eastern region (69%) while it was low in southern region (26%). The proportion of the respondents belongs to High SLI (More than 25) varies from as low as 9- 10% in northern, eastern and western zone to as high as 30% in southern region. Table 3.4: Assets/Possession of Households of TB patients identified during the survey
Characteristics Household Assets (% Ownership) Electricity Mattress Pressure cooker Chair cot or Bed Table Electric Fan Radio Or Transistor Black & white Television Color Television Sewing Machine Mobile Telephone North N 73 79 36 65 138 38 54 20 15 23 26 76 % 50 55 25 45 95 26 37 14 10 16 18 52 East N 127 76 51 143 186 86 54 39 16 33 21 115 % 54 32 22 61 79 37 23 17 7 14 9 49 West N 103 53 44 86 91 44 61 16 16 45 14 53 % 83 43 36 69 73 36 49 13 13 36 11 43 South N 102 75 36 85 78 56 83 10 3 76 11 75 % 97 71 34 81 74 53 79 10 3 72 11 71 Total N 405 283 167 379 493 224 252 85 50 177 72 319 % 67 47 27 62 81 37 41 14 8 29 12 52
38
Characteristics Any other Type of Phone Computer Refrigerator Watch or Clock Bicycle Motorcycle or Scooter Animal drawn cart Car Water Pump (For agricultural Use) Thresher (For agricultural Use) Tractor(For agricultural Use) Standard of Living Index Low SLI Medium SLI High SLI Household Income Less than Rs. 2000 Rs. 2000 - Rs. 4000 Rs. 4001 - Rs. 8000 Rs. 8001 - Rs. 10,000 Rs. 10,001 and above Dont know Total
North 4 3 0 0 10 7 92 64 93 64 9 6 6 4 1 1 17 12 1 1 3 2 84 46 15 63 61 10 7 3 1 145 58 32 10 44 42 7 5 2 1
East 5 2 4 2 15 6 147 63 102 43 14 6 0 0 2 1 5 2 2 1 0 0 161 51 23 69 22 10
West 7 6 1 1 6 5 96 77 78 63 15 12 4 3 1 1 18 15 0 0 1 1 62 49 13 41 48 16 4 3 12 124 50 40 11 33 39 13 3 2 10
South 11 11 2 2 15 14 81 77 45 43 33 31 2 2 5 5 10 10 0 0 1 1 27 46 32 26 44 31
Total 27 4 7 1 46 8 416 68 318 52 71 12 12 2 9 2 50 8 3 1 5 1 334 192 83 55 32 14
75 32 125 53 22 9 3 1 4 2 6 3 235
33 31 36 34 16 15 8 8 1 1 11 11 105
212 35 270 44 64 11 22 4 11 2 30 5 609
Figure 3.1: Proportion of TB patients living in the Lowest Standard of Living Index disaggregated by State
The states with less than 7 % of households in low SLI is not shown in the figure. The figure shows that the households of 85 % of TB diseased persons in Orissa belong to Low SLI while only less than 10 % of TB diseased persons in Mizoram and Tamil Nadu belongs to Low SLI.
39
3.3
KNOWLEDGE, ATTITUDE & PRACTICES This section presents the existing experiences, knowledge, attitude and Practice of TB diseased persons interviewed during the survey. Knowledge that TB is caused by micro-organisms Tuberculosis is caused by Micro-organisms (a bacterium called Mycobacterium Tuberculosis). The proportion of patients who knew that TB is caused by microorganisms is given in table 3.5. Table 3.5: TB patients awareness on what causes Tuberculosis
Variables Total sex Female Male Age group <25 Years >=25<55 Years >=55 Years Literacy status Illiterate Literate Household income <4000 =>4000 Don't Know Setting Rural Tribal Urban Unknown Zone East North South West Don't Know N % 298 49 125 173 65 161 72 151 147 251 27 20 215 32 43 8 155 74 21 48 57 45 58 47 47 57 43 52 28 67 55 36 37 67 66 51 20 39 Microorganisms/germs N % 201 33 59 142 36 109 56 72 129 148 46 7 109 35 55 2 44 52 68 37 27 37 32 32 36 27 37 31 47 23 28 40 48 17 19 36 65 30 Other causes N % 110 18 36 74 11 72 27 41 69 83 24 3 70 21 17 2 36 19 16 39 16 19 10 21 17 16 20 17 25 10 18 24 15 17 15 13 15 32 Total 609 220 389 112 342 155 264 345 482 97 30 394 88 115 12 235 145 105 124 %
100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100 100
Overall, 49% of the TB patients did not know what causes tuberculosis, 33% knew that it is caused by germs/micro-organisms and the remaining 18% knew that TB is caused by other causes. The proportion of TB patients who correctly knew that TB was caused by micro-organisms/germs was relatively higher among males, literates, those living in urban areas, those who were previously treated for TB.
40
Among the four zones, the proportion who correctly knew that TB is caused by germs/micro-organisms was higher among TB patients from the south-zone when compared to all other zones. Out of the 609 TB patients, 573 (94.1%) were having pulmonary TB, 28 (4.6%) were having extra-pulmonary TB and TB site could not be ascertained in 8 (1.3%) of the TB cases. Personal experience of the symptoms of TB in pulmonary TB For nearly three fourth of the patients, this was the first time that they were diagnosed with TB (new cases) whereas the remaining patients were previously treated (treated for TB in the past for more than a month prior to the current treatment episode). Nearly two thirds (66%) had cough as the presenting symptom, almost half (47%) had fever, one third (33%) had chest pain (Table 3.6) Table 3.6: Symptoms experienced by TB diseased Persons prior to the diagnosis of the present episode of TB
Characteristics Diagnosis of TB First time diagnosed with TB Major Symptoms of TB * Cough Fever Chest Pain Blood in Sputum Weight Loss Total (N) 72 51 26 30 8 145 50 35 18 21 6 186 131 113 58 24 235 79 56 48 25 10 72 58 36 17 11 124 58 47 29 14 9 70 45 23 3 14 105 67 43 22 3 13 400 285 198 108 57 609 66 47 33 18 9 North N 115 % 79 East N 186 % 79 West N 107 % 86 South N 62 % 59 Total N 470 % 77
* those symptoms experienced by less than 9% of the patients are not shown in the table
The duration between onsets of symptoms to diagnosis of TB is given in Table 3.7. Overall, 34% of the TB patients did not have cough. Of those who had cough (n=400), Majority (N=352, 88%) were diagnosed within the period of 10 weeks (2.5 months) after the onset of cough. However, the proportion of TB patients with cough diagnosed within 3 weeks of the onset of symptoms were 50% of the TB patients
41
Table 3.7: Duration between onset of symptoms to diagnosis of tuberculosis
Duration N 1 Week 2 Weeks 3 Weeks > 3 weeks-6 Weeks > 6 weeks-10 Weeks 11-20 Weeks >5 months Absence of corresponding symptom Total 22 116 66 126 32 26 12 209 609 Cough % 4 19 11 21 5 4 2 34 100 N 37 102 34 68 26 16 2 324 609 Fever % 6 17 6 11 4 3 0 53 100
Nearly half of the patients did not have fever. Those with fever (n=285), 80% were diagnosed within 6 weeks of the onset of symptoms. Health Seeking Behaviour of TB patients after the onset of Symptoms (Table 3.8) Majority (~70%) of the patients had consulted within a month of onset of symptoms either their family members or any health service providers about their symptoms. The survey asked the respondents about their first source of consultation after the onset of symptom. Close to 50% of the respondents mentioned consulting their family members /spouse/relative either simultaneously or before going to any health service provider. Around 40 % reported that they visited qualified private health care providers of their area. Government dispensary/health centre were found to be source of consultation for only quarter of the TB diseased persons. Table 3.8: Health seeking behaviour of TB diseased Persons prior to diagnosis
Characteristics North N First Visit to HSP after onset of symptom less than a week In 15 days After 15 days to 1 month After 1 month to less than 2 months 2 months to 3 months More than three months Not visited /Dont Remember Source of Consultation before diagnosis* 24 44 24 26 14 13 0 17 30 17 18 10 9 0 24 53 97 36 7 16 2 10 23 41 15 3 7 1 12 36 35 31 4 4 2 10 29 28 25 3 3 2 12 36 23 24 7 0 3 11 34 22 23 7 0 3 72 169 179 117 32 33 7 12 28 29 19 5 5 1 % East N % West N % South N % Total N %
42
Characteristics Qualified private doctor/clinic Family Members /Spouse/Relative Govt. dispensary /health centre Unqualified Healer in locality (quack) Local Health Care Provider
North 55 43 41 37 17 38 30 28 26 12
East 119 141 45 34 22 235 51 60 19 15 9
West 43 48 37 15 14 35 39 30 12 11
South 36 67 29 5 7 105 34 64 28 5 7
Total 253 299 152 91 60 609 42 49 25 15 10
Total (N) 145 *Multiple answers, so % may add to more than 100.
124
Diagnosis of Tuberculosis (Table 3.9) For TB control, Government is providing diagnosis and treatment of TB under DOTS free of cost to all the people. This section addressed the awareness on treatment, source of medicines, awareness on duration of treatment and other social and economic barrier in continuing the treatment of Tuberculosis. Nearly 70% of the respondents had heard of free diagnosis and treatment of TB and the proportion was more or less similar in all three zones except eastern region. A point for concern was that 30% of TB diseases persons (under treatment) were not aware of the free DOTS treatment provided by the government. Table 3.9: Diagnosis of tuberculosis among Diseased Persons
Characteristics Diagnosis of TB Heard of Free Diagnosis & treatment Source of TB Diagnosis Government health facility Non-Government health facility others/unknown Investigations Underwent Sputum examination Underwent X-Ray examination Under went Blood Tests Made Payment for investigations No. of providers visited prior to diagnosis 1 provider North N 111 % 77 N 142 East % 60 N 96 West % 77 South N 77 % 73 N 426 Total % 70
98 46 1
68 32 0
89 141 5
38 60 2
96 27 1
77 22 1
83 22 0
79 21 0
366 236 7
60 39 1
133 135 135 102
92 93 93 70
187 221 217 170
80 94 92 72
120 117 107 55
97 94 86 44
103 102 103 44
98 97 98 42
543 575 562 371
89 94 92 61
29
20
73
31
39
32
47
45
188
31
43
Characteristics 2 providers 3 providers 4 providers 5 providers > 5 providers Can't say Duration between onset of symptoms to diagnosis <=1 month > 1 month Can't Say Site of Tuberculosis Extra-pulmonary Pulmonary Unknown Type of Tuberculosis New previously treated Total
North 57 31 13 4 11 0 39 21 9 3 8 0 97 28 20 5 10 2
East 41 12 9 2 4 1
West 37 19 12 7 7 3 30 15 10 6 6 2 8 5 1 4 8
South 32 31 8 5 1 4 8 86 50 17 32 13
Total 223 37 14 8 3 5 2
107 36 2 3 142 0 115 30 145
74 25 1 2 98 0 79 21
169 58 8 17 213 5 186 49 235
72 25 3 7 91 2 79 21
92 32 0 2 122 0 107 17 124
74 26 0 2 98 0 86 14
80 20 5 6 96 3 62 43 105
76 19 5 6 91 3 59 41
448 146 15 28 573 8 470 139 609
74 24 3 5 94 1 77 23
In 60% of the TB cases, the diagnosis of TB was made in a Government Health Facility and in the remaining cases; it was done in a non-government health facility (predominantly private health care providers). The proportion of TB cases diagnosed in a government health facility was highest in the south zone (79%) and lowest in the east Zone (38%). Almost 90% of the patients had undergone sputum smear examination, and more than 90% of the patients had undergone X-Ray examination and blood tests for the diagnosis of TB. Nearly three out of five (61%) patients informed that they had made payments for the TB investigations. The proportion of patients who had undergone sputum examination was lower in East Zone (80%) and the proportion of patients who reported having had to pay for TB medicines was highest in the east Zone (72%) and lower among TB patients from the southern zone (42%). Nearly 72% of the patients were diagnosed of tuberculosis after having to visit one, two or three providers. However, more than 15% of the TB patients had visited more than three providers prior to the diagnosis of tuberculosis. There were minimal zone wise variations on this aspect.
44
Nearly three fourth (74%) of the TB patients were diagnosed within 1 month of the onset of the symptoms. The proportion of patients who were diagnosed within 1 month remained more or less the same across all the zones. The site of TB disease for more than 90% of the TB patients was pulmonary. This was also observed across all zones. Nearly three fourth of the TB patients this was the first episode of TB treatment also called as new TB cases. 23% of the remaining TB patients were previously treated (i.e., taken TB treatment for more than a month in the past prior to the present episode of TB) Treatment of Tuberculosis (Table 3.10) Nearly 70% of the patients were initiated on TB treatment within 7 days of diagnosis, 8% could not recollect exactly how many days after the diagnosis they were initiated on treatment (table 3.10). The duration was more than 7 days in 22% of the cases, with 13% of the patients initiated on treatment more than 2 weeks after the diagnosis of TB was made. On asking the respondents of their source of medicines (Table 3.10), nearly 54% of them were taking their medicines from the government centres (absolutely free of cost) while the remaining were not taking medicines from the government centres free of cost. Very few of them (6%) also mentioned even government centres were not providing medicines free of cost. There is distinct zone wise variation existed in the source of medicines. Government centres acted as a free source of medicines for more than three fourth of the TB diseased persons from southern region while nearly half of the TB diseased persons from eastern region were taking medicines from non-government centres by paying money for it. Lack of information on various aspect accounts for low cure rate of the TB diseased persons. Only 80% of the patients were aware that TB treatment has to be taken regularly. The proportion of TB diseased people who knew about the need for taking medicines regularly was higher in the south zone (88%) when compared to northzone where it was only 75%. Regarding awareness on the duration of treatment of tuberculosis, only 55% of TB diseased persons were aware that medicines should be taken for 6-8 months for its complete cure.
45
Table 3.10: Treatment for TB among TB diseased persons
Characteristics Duration between diagnosis and initiation of TB treatment 1-3 days 4 days-1 week >1-2 weeks >2-3 weeks >3 weeks Can't say Source of TB Medicine Government health centres, free of cost under DOTS Government health centres, with payment for medicines Non-government health centres, with payment for medicines Non-government health centres, free of cost Unknown Aware that treatment has to be taken regularly Awareness on Duration of Treatment Less than 2 weeks 2-4 weeks 1-3 months 4-5 months 6-8 Months More than 8 months Dont know/Not aware Total 3 2 4 5 91 33 7 145 1 2 8 4 59 19 8 1 4 24 8 129 52 17 235 2 1 3 4 63 23 5 1 0 8 6 78 23 8 124 0 2 10 3 55 22 7 3 6 11 5 58 8 14 105 1 0 7 5 63 19 6 8 12 47 24 356 116 46 609 3 6 11 5 55 8 13 North N % N East % N West % N South % N Total %
73 33 15 11 8 5
50 23 10 8 6 3
107 52 16 13 9 38
46 22 7 6 4 16
69 26 11 9 3 6
56 21 9 7 2 5
38 20 18 17 9 3
36 19 17 16 9 3
287 131 60 50 29 52
47 22 10 8 5 9
62
43
85
36
85
69
78
74
310
51
15
10
11
36
58
40
116
49
26
21
18
17
218
36
4 6 109
3 4 75
9 14 188
4 6 80
2 2 98
2 2 79
6 2 93
6 2 89
21 24 488
3 4 80
General Health Seeking Behaviour of the families of TB patients (Table 3.11) Families of TB Diseased persons are usually at higher risk of developing tuberculosis. If they seek care at facilities from where the TB diagnosis and treatment can be availed, early detection of tuberculosis and prompt treatment will be possible.
46
During the survey the respondents were asked to identify the place where they/their family members generally/usually go when they get sick. Nearly two third of the respondents (60%) usually seek health care from the Government hospitals which includes PHC, CHC and District hospital while 33% of the respondents mentioned visiting Private Clinic or Hospital to seek health care for any illness. Very few of the respondents also mentioned visiting non-qualified practitioners or Traditional healers doctors for any kind of illness. Government health care remained a primary source of health care for majority of the respondents for both rural (70%) and urban area (81%). The proportion of respondents mentioned visiting non-qualified practitioners /traditional healers were reported majorly from rural area. Overall, 40% of the respondents were not visiting Government health facilities for any kind of illness and seeking healthcare. The two main reasons for not visiting Government health facilities mainly because the patients felt that there were lack of diagnostic facilities (42%) in these hospitals and unfriendly behaviour of service providers (34%). Table 3.11: Health Seeking Behaviour of households of TB diseased Persons
Characteristics Health Seeking Behaviour Government Hospital (Including PHC,CHC) Private Clinic /Private Hospital Traditional healer/ Quacks Ayurveda health service providers Sub Center/ANM Homeopathic health service providers Reason for not visiting Government Lack of Diagnostic facility Unfriendly behaviour Hospital is far from home Long Waiting Hours Unavailability of doctors Private Clinic is nearby Total 22 25 12 13 6 9 145 37 42 20 22 10 15 73 53 51 37 25 18 235 53 38 37 27 18 13 7 2 11 10 6 2 124 32 9 50 46 27 9 1 4 8 13 8 2 105 4 16 32 52 32 8 103 84 82 73 45 31 609 42 34 34 30 18 13 North N 86 46 12 1 0 0 % 59 32 8 1 0 0 N 96 111 23 4 0 1 East % 41 48 10 2 0 0 West N 102 19 0 1 2 0 % 82 15 0 1 2 0 South N 80 25 0 0 0 0 % 76 24 0 0 0 0 Total N 364 201 35 6 2 1 % 60 33 6 1 0 0
47
Sources of TB related Information (Table 3.12) The survey probed on the source of information for their TB related knowledge, most preferred source of information and if anybody visited them to provide information on TB. Nearly 50% of the TB diseased person reported Interpersonal communication from either paramedical workers or persons in the general community or medical doctors were the sources of information for their current TB related knowledge. Electronic and Print media acted as the source of information for only 21 % of the people diseased with TB. Television or radio, newspapers or hoardings were sources of information in less than a quarter of the TB patients. TB patients preferred to receive information on TB from radio, cinema, newspapers, magazines, television and from the hospitals. Table 3.12: Source of Information for TB Diseased Persons
Characteristics Existing Source of TB related info* Television Hospital /Doctors Interpersonal Communication Newspaper/Magazine/Hoardi ngs/ Radio Preferred Source of TB related info* Radio Cinema Newspaper/Magazine/Hoardi ngs/ Television Hospital/Doctors Total 9 9 10 6 8 145 60 60 67 40 53 16 15 14 14 19 235 55 52 48 48 66 5 5 3 2 7 124 63 63 38 25 88 22 23 24 28 6 105 76 79 83 97 21 52 52 51 50 40 609 64 64 63 62 49 North N 21 78 91 52 9 % 14 54 63 36 6 N 43 114 144 34 21 East % 18 49 61 14 9 N 38 37 49 27 6 West % 31 30 40 22 5 South N 27 41 12 15 3 % 26 39 11 14 3 N 129 270 296 128 39 Total % 21 44 49 21 6
*multiple responses possible
48
In summary Based on the information provided by 609 TB patients out of the 752 TB patients identified in the community, the key indicators are as follows:
North 145 N % 96 66 79 55 63 52 111 98 86 44 36 77 68 59 East 235 N 139 106 75 44 142 89 170 % 59 45 32 19 60 38 72 West 124 N % 78 63 50 40 41 30 96 96 76 33 39 77 77 62 South 105 N % 76 72 29 28 33 65 77 83 79 31 16 73 79 76 Total 609 N % 389 64 264 43 212 201 426 366 411 35 33 70 60 68
Characteristics Total number of TB patients TB Patients who were Male TB patients who were Illiterate TB patients with Household monthly income Less than Rs. 2000 Aware that TB is caused by microorganisms Heard of free diagnosis and treatment of Tuberculosis Underwent diagnosis in a government Health facility No. of patients who visited two providers or Less for the diagnosis of TB Patients diagnosed within 1 month of the Onset of symptoms Proportion of TB patients initiated on Treatment within 7 days of diagnosis Receiving treatment free of cost under DOTS Aware that treatment has to be taken regularly Aware that the duration of treatment is For 6-8 months
107 106 66 109 91
74 73 46 75 59
169 159 94 188 129
72 68 40 80 63
92 95 87 98 78
74 77 70 79 55
80 58 84 93 58
76 55 80 89 63
448 418 331 488 356
74 69 54 80 55
49
CHAPTER 4 HEALTH SERVICE PROVIDERS The service providers were one of the key components of the study and comprised of health personnel of different systems like MBBS (Qualified in Allopathic systems), BAMS (Qualified in Ayurvedic systems), BHMS (Qualified in Homeopathic systems), and BUMS (Qualified in Unani Systems). The questionnaire was designed in a way to get insight from service providers on knowledge and treatment of TB, barriers in TB detection and their involvement in RNTCP programme. These service providers were present in the primary sampling units that were chosen to do the general population survey. A total of 614 health care providers were practicing in the localities of the Primary Sampling units. On the basis of their educational qualification, more than half of them (55%) were MBBS, while the remaining were BAMS (26%), BHMS (12%), BUMS (5%) and the remaining were not qualified in any of the systems of medicine mentioned above. Table 4.1 elaborately deals with the general characteristics of the service providers at regional and national level showing that almost 90% of the service providers were males in comparison to female service providers (who were just 10 %). More than half of the health service providers were qualified allopathic medicine practitioners (55%). The proportions of allopathic practitioners were higher in the eastern and southern zones when compared to the northern (45%) and West Zones (39%). The different regions are hardly in difference with each other since in all the regions private practitioner are higher in numbers and in total there are 62.7% private practitioner while a little more than one fourth (32%) are government practitioners. Table 4.1: General Characteristics of Service Providers
Characteristics Gender Male Female Age 18-25 years 26-35 years 36-45 years 46 + years Category Private Government Education Qualification North N % 142 95 8 5 3 44 49 54 109 32 2 29 33 36 73 21 East N 150 14 2 38 49 75 86 68 % 93 7 1 23 30 46 52 42 West N 152 12 1 45 60 58 105 55 % 77 24 1 27 37 35 64 34 South N 104 32 4 35 37 60 85 42 % 89 11 3 26 27 44 63 31 Total N 548 66 10 162 195 247 385 197 % 89 11 2 26 32 40 63 32
50
Characteristics MBBS BAMS BHMS BUMS Others (BDS, BSc, traditional) Nature of Practice Dispensing GP Prescribing GP Consultant Specialist Total
North 67 45 43 29 19 13 22 15 0 98 46 6 150 0 65 31 4
East 119 73 24 15 16 10 4 2 6 55 93 16 164 4 34 57 10
West 64 39 59 36 32 20 9 5 10 113 19 32 164 6 69 12 20
South 87 64 26 19 7 5 0 0 20 49 28 59 136 15 36 21 43
Total 337 53 152 24 74 12 35 5 36 315 186 113 614 6 51 30 18
4.1
KAP ON TUBERCULOSIS This chapter depicts the knowledge level and treatment related attitude and practices of service providers. Uniformly (94%) all the HSP identified A cough of two weeks as the major symptom for Tuberculosis. Also few other symptoms of TB mentioned were Fever 64.5 %, Coughing of Blood 59% and Pain in the chest 52% at the national level and the same trend also holds true at the regional level. Almost half of the Health Service Providers were dispensing while rest of the practitioners were either prescribing or consultant specialist. Table 4.2 reveals about 96.7 % of the health service providers had come across TB patients that were suffering from Pulmonary TB. The other types of the TB patients that the practitioners usually come across were Lymph TB 36%, Abdominal TB 14%, Spinal TB 11% and the other types 14 % respectively. Thus this is a clear indication that the major type of TB diagnosed by the practitioners cutting across the geographical & regional boundaries was Pulmonary TB. Despite the fact that the respondents were medical practitioners awareness about MDR TB (Multi Drug Resistant TB) was not so high. Nationally 64% were aware about MDR TB while regionally the awareness ranges between 59% to 71% with eastern region having the highest level of awareness and Western region was at the lowest. On the various techniques related to diagnosis of MDR TB 55% believed in conducting the Sputum culture/sensitivity test, while 20% of them stated that they practice Clinical Examination for confirmation of MDR TB. Some other ways of diagnosing the MDR TB suggested by Health Service Providers were X-Ray, Blood test, P.C.R, etc, clearly indicating the need for better training for these medical practitioners on MDR-TB.
51
Table 4.2: Knowledge on Tuberculosis (Multiple response*)
Characteristics Symptoms of TB A cough of 2 weeks Pain in the chest Coughing up blood Fever Weight less Any Other Types of TB patients diagnosed by HSP Pulmonary TB Lymph TB Spinal TB Abdominal TB Any Other Heard of MDR TB Diagnosis of MDR TB Based on sputum culture/sensitivity Clinical Examination Other tests Total North N % 141 60 76 111 15 5 94 40 51 74 10 3 East N 151 100 102 110 7 1 % 92 61 62 67 4 1 West N % 157 90 112 96 11 2 96 55 68 59 7 1 South N % 127 68 72 79 18 2 93 50 53 58 13 1 Total N % 576 318 362 396 51 10 94 52 59 65 8 2
148 43 11 33 84 90
99 29 7 22 9 60
160 90 19 23 14 116
98 55 12 14 24 71
161 43 16 18 39 97
98 26 10 11 7 59
125 45 25 15 11 87
92 33 18 11 15 64
594 221 71 89 20 390
97 36 12 15 14 64
88 26 25 150
59 17 17
92 40 13 164
56 24 8
83 31 23 164
51 19 14
71 30 21 136
52 22 15
334 127 82 614
54 21 13
4.2
TREATMENT APPROACH OF HEALTH SERVICE PROVIDERS In the follow-up questions HSPs were asked about where they send the TB suspects for Sputum examination for confirmation of Pulmonary TB (Table 4.3). It has been observed that more than three fourth of these practitioners (79%) recommended to Government Hospitals with Designated Microscopy Centre (DMC), at the same time as many as 16% mentioned that they send it to the Private Hospitals with DMC, though a very few 4% were also send to the Private Hospitals without DMC facility. On the issue related to the problems of getting the Sputum smear examination at these done at these facilities 13% HSPs acknowledged that they faced problems in getting these examinations done. These problems range from Non-availability of sputum smear examination facility in 51% to Non-availability of staff 17%. One of the major constraints in these examinations is inability of patients to incur the costs for these tests which is as high as 44%.
52
In Eastern & Southern regions this inability on monetary part is almost affecting half of the diseased population to get these tests done at these facilities. On the questions of post diagnosis steps taken by the service providers a little below three fourth (71%) recommend their patients to visit the Government Hospital/or DOTS centre to have complete course for their proper treatment. At the same time just above one fourth i.e. 29% HSPs start treatment of these patients on their own. Only a hand-full of the service providers refer them to the private facility or to some NGOs which is only about 5.1 & 9% respectively. The Health Service providers were questioned about the medicinal system followed by them for treatment of the Pulmonary TB where it has been found that mostly they follow the allopathic treatment for their patients (87.7%). This medicinal system is also in majority because of the very reason that most of these service providers are from Allopathic background. To certain extent Homeopathic treatment is also practiced in Western region where 12.8 percent HSP follow this medicinal approach. When inquired for duration of treatment for the TB, most of the service providers (79%) acknowledged that it requires 6-8 months, while 12 % said that it takes more than 8 months or more for complete therapy. Less than one tenth of the providers believed TB patients could be treated in between 1-5 months. Table 4.3: Tuberculosis Diagnosis and treatment approach of Health Service Providers
Characteristics Place for sending Sputum smear Examination Govt. Hospital with DMC Private Hospital with DMC Private Hospital without DMC Any other Lab Face any kind of Problem for Sputum smear examination of TB Type of Problem Non-Availability of Facility Non-Availability of Staff Patient is unable to incur expenses Poor Quality Results Post Diagnosis Activity Advise to go to Government /TB Hospital 75 58 91 63 127 88 87 75 380 71 North N % N East % West N % South N % Total N %
88 40 17 5 20
59 27 11 3 13
127 28 6 3 20
77 17 4 2 12
154 9 1 0 20
94 6 1 0 12
116 20 0 0 20
85 15 0 0 15
485 97 24 8 80
79 16 4 1 13
9 2 9 3
45 10 45 15
7 4 10 1
35 20 50 5
15 4 6 3
75 20 30 15
10 4 10 0
50 20 50 0
41 14 35 7
51 18 44 9
53
Characteristics Treat on their own Refer to private facility Refer to DOTS centre (if specifically mentioned) Refer to NGO System of Medicine Followed for TB treatment Allopathic Homeopathy Ayurvedic Traditional Duration of TB Treatment 1-2 weeks 2-4 weeks 1-5 months 6-8 months More than 8 months Total
North N 50 6 16 1 % 39 5 12 1 N
East % 32 6 8 0 46 8 11 0
West N 25 2 9 0 % 17 1 6 0
South N 34 11 12 0 % 29 10 10 0
Total N 155 27 48 1 % 29 5 9 0
141 9 0 0
94 6 0 0
147 15 2 0
90 9 1 0
135 21 5 3
82 13 3 2
116 14 4 2
85 10 3 1
539 59 11 5
87 10 2 1
0 0 5 116
0 0 3 77
1 4 8 130 21 164
1 2 5 79 13
1 0 10 140 13 164
1 0 6 85 8
1 4 17 102 12 136
1 3 13 75 9
3 8 40 488
0 1 7 79
29 19 150
75 12 614
4.3
PRECAUTION AND RECOMMENDATION The Health service providers were asked about the problems faced by them while treating the TB patients. As illustrated in table 4.4 multiple responses were given by the HSPs on this. One of the foremost problems faced by HSPs is that half of the patients (50.9%) are hesitant in coming for the treatment due to the stigma and discrimination associated with this disease. Similarly because of the same reasons 33% patients dont reveal their previous history of TB. Few other impediments in treating TB patients were Non-availability of anti TB drugs in 11% cases and inaccessibility of pathology or X-ray lab in the nearby vicinity of the patients in 10% cases. Almost 37 % of these service providers were apprehensive about their own health and health of other patients while dealing and treating tuberculosis patients. The HSPs were asked questions about precautionary measures adopted by them to ensure their own safety in response of which they said that in more than 62 % cases they wear masks and gloves while they treat any patients suffering from TB, in addition to this in 51% cases they wash their hands with soap after the treatment. HSPs also ensures that while making any contact/treatment with TB patients a proper distance is be maintained as responded by 47% cases.
54
On the other hand while giving the precautionary advice/recommendations to the TB patients, service providers said that as many as 92% time they suggest patients to cover their face while coughing, or in 72% cases they suggest them not to spit anywhere. Similarly they were advised to use separate utensils (44%) and separate towels/clothes in 38% cases. Table 4.4: Challenges, precautions and advises given by Health Service Providers in dealing with Tuberculosis Patients
Characteristics Difficulties while treating TB patients People hesitate to come for treatment Non availability of anti TB drugs No pathology or X ray Lab available in the vicinity People do not reveal previous history of TB easily Don't completed the course None Precaution to Protect yourself from TB Maintain distance Wear masks & gloves Wash hands with soap None Advice given to TB patients Cover your face while coughing Use separate utensils Not to spit anywhere Use separate towels/clothes Isolate the patient Avoid Tobacco/smoking North N 88 14 14 58 5 32 % 59 9 9 39 3 21 61 N 63 11 14 51 1 62 53 East % 38 7 9 31 1 38 32 West N 102 24 24 50 6 16 58 % 62 15 15 30 4 10 35 South N 60 19 12 45 2 55 22 % 44 14 9 33 1 40 16 Total N 313 68 64 204 14 165 225 % 51 11 10 33 2 27 37
TB constitute risk to other Patients 92
99 73 45 8 144 79 100 61 11 4 150
66 49 30 5 96 53 67 41 7 3
80 76 95 19 150 49 118 32 30 4 164
49 46 58 12 91 30 72 20 18 2
52 123 92 6 144 95 128 83 21 0 164
32 75 56 4 88 58 78 51 13 0
61 111 84 8 130 48 104 59 15 0 136
45 82 62 6 96 35 76 43 11 0
292 383 316 41 568 271 450 235 77 8 614
48 62 51 7 93 44 73 38 13 1
4.4
PERCEPTION OF HEALTH SERVICE PROVIDERS ON DOTS/ RNTCP The understanding acquired by the health service providers in course of their medical practice and contacts made with TB diseased persons reflects their perceived experience on DOTS programme, involvement in various scheme and how other patients reciprocates to these HSPs who are engaged in treating TB patients.
55
Since these service providers were involved in treating TB patients when asked for DOTS, a little above half (52.6%) of the services providers considered DOTS excellent while almost 36% stated this therapy good which clearly shows the faith deposited in the DOTS. In-spite of the fact that DOTS is concerned one of the best measure for treating TB, the knowledge among the HSPs about any scheme to involve private practitioners in DOTS programme is only around 52 % showing that they were not aware of these schemes. The same holds true for Government Doctors as well when inquired for their involvement in DOTS programme only 49 % confirmed their participation in some way or other, clearly demanding a wider participation both among public and private practitioners. Table 4.5: Perception of Health Service Providers on DOTS/ RNTCP
Characteristics For Treating TB: Do you feel; DOTS is Excellent Good Average Bad Aware about Schemes to involve Private Practitioners in DOTS programme Yes NO Participate in DOTS programme (Govt. Doctors) Yes NO Perception that other patients may not come to them if they treat TB patients Yes NO DK/CS North N 64 63 23 0 % 43 42 15 0 N 77 72 15 0 East % 47 44 9 0 N 98 48 18 0 West % 60 29 11 0 N 84 39 5 8 South % 62 29 4 6 N 323 222 61 8 Total % 53 36 10 1
83 67 32 11 21
55 45
92 72 68
56 44
65 99 55
40 60
79 57 42
58 42
319 295 197
52 48
34 66
39 29
57 43
22 33
40 60
27 15
64 36
99 98
50 50
12 130 8 150
8 87 5
12 151 1 164
7 92 1
18 146 0 164
11 89 0
8 127 1 136
6 93 1
50 554 10 614
8 90 2
56
One other issue that needs to be answered is how masses react towards both TB diseased patients and medical practitioners because of the stigma and discrimination associated with TB if it exists in any form. The fact that though small but still 8 % perceived that patients of other diseases are reluctant to visit them because of their treating TB patients shows stigma attached with Tuberculosis. Predominant Source of TB Related Information The respondents were asked about their predominant source of information of TB. Nearly three fourths of the respondents had mentioned that their predominant source of information was by reading Medical Journals or Text Books. Nearly one third of the respondents had mentioned that their sources of TB related information were their colleagues or by attending CME/ Training. Medical Representatives formed another major source of information to one-fourth of the respondents. Professional bodies acted as a source of information to less than 10% of the respondents.
Characteristics Medical journals/ Text Book Colleague CME/trainings / Conferences/TV Professional bodies Medical representatives North 114 76 42 28 45 30 9 6 47 31 150 East 125 76 43 26 81 49 8 5 32 20 164 West 131 80 56 34 46 28 11 7 48 29 164 South 101 74 45 33 42 31 21 15 28 21 136 Total 471 77 186 30 214 35 49 8 155 25 614
Table 4.6: Summary of Key KAP survey Indicators of Health Care Providers:
Characteristics Major Symptoms of TB A cough of 2 weeks Place for sending patients for sputum smear Examination Govt. Hospital with DMC System of Medicine Followed for TB treatment Allopathic For Treatment of TB Advise to go to Government /TB Hospital for treatment under DOTS Heard of MDR TB Aware that MDR-TB is diagnosed based on sputum culture/sensitivity Duration of TB Treatment 6-8 months Aware about Schemes to involve Private North N 141 % 94 N 151 East % 92 West N 157 % 96 South N 127 % 93 Total N 576 % 94
88
59
127
77
154
94
116
85
485
79
141 75 90 88
94 58 60 59
147 91 116 92
90 63 71 56
135 127 97 83
82 88 59 51
116 87 87 71
85 75 64 52
539 380 390 334
88 71 64 54
116
77
130
79
140
85
102
75
488
79
57
Characteristics Major Symptoms of TB Practitioners in DOTS programme Predominant Source of TB Related Information Medical journals/ Text Book
North N 11 % 34 N
East % 57 39
West N 22 % 40
South N 27 % 64
Total N 99 % 50
114 150
76
125 164
76
131 80 164
101 74 136
471 77 614
58
CHAPTER 5 OPINION LEADERS A questionnaire was designed for Opinion leaders also to understand their role in improving Tuberculosis care and control for the communities and how they can contribute towards this cause on the basis of their knowledge, attitude and practices on this particular issue. Opinion leaders are influential leaders in the society to whom people look upon for advices, opinion and views thus significantly affecting the course of action taken by the persons in the community. These opinion leaders are primarily functionaries at grass root working in different capacities and mainly comprise of elected representatives of Panchayati Raj Institutions like Village Pradhan, Sarpanch/Panch/Ward members, religious leaders, teachers or health functionaries like ANM (Auxiliary Nursing Midwife) AWW (Anganwadi Worker). Care was taken to ensure that at each district at least one to two available and contactable (on the days of the survey) opinion leaders were selected and interviewed from each of the primary sampling units. If more than 2 opinion leaders were identified in any primary sampling unit then priority was given to elected representatives, teachers, religious leaders and then to health workers (in that order) for inclusion in the study. 5.1 PROFILE Table 5.1 and Fig 5.1 depicts the brief profile of these Opinion leaders who were selected for interview during the course of the survey. 61% of the opinion leaders selected for interview were male while females constituted 39%. A total 511 respondents were interviewed which included 131 from Northern, 143 from Eastern, 138 from Western and 99 from Southern region respectively. A reasonable number of respondents were below 35 years (30 % of them were in the age group of 26-35 years while 36% of the respondents were in the age group of 35-46). As much as 46 percent of these opinion leaders selected for interview were elected representatives as they are Pradhans, Sarpanch, Panch and Ward members representing different constituencies. Anganwadi workers constituted 16% of the opinion leaders group interviewed followed by teachers with 13% representation. Table 5.1: General Profile of Opinion Leaders interviewed during the survey
Characteristics Gender Male Female North N % 87 66 44 34 East N 73 70 % 51 49 West N % 88 64 50 36 South N 63 36 % 64 36 Total N % 311 61 200 39
59
Characteristics Age 18-25 years 26-35 years 36-45 years More than 46 yrs Respondents Category Village Pradhan Panchayat Member Ward Member Religious Leader ANM AWW Teacher Not Specified Total
North 8 39 49 35 37 22 17 16 4 18 10 7 131 6 30 37 27 28 17 13 12 3 14 8 5 11 45 43 44 8 14 32 14 6 35 22 12
East 8 32 30 31 6 10 22 10 4 25 15 8 143
West 2 52 57 27 12 10 27 17 7 21 21 23 138 2 38 41 20 9 7 20 12 5 15 15 17 5 19 36 39 16 12 25 10 7 9 14 6
South 5 19 36 39 16 12 25 10 7 9 14 6 99
Total 26 155 185 145 73 58 101 57 24 83 67 48 511 5 30 36 28 14 11 20 11 5 16 13 9
Figure 5.1: Profile of Opinion Leaders included in the survey
Table 5.2 portrays the responses made by the opinion leaders about knowledge and awareness about Tuberculosis and its treatment. When the opinion leaders were asked about the common diseases in their community, the spontaneous recall of TB was only 22 % but when they were probed further about whether they had heard of TB, the answer was in affirmation and the response was 100% that they have heard about Tuberculosis. This was followed by asking them about their knowledge on few symptoms of TB where multiple responses were given by them and a majority of them (88%) believed that A cough of two weeks is a most important symptom of TB.
60
Other than this 47.5% thought that coughing up of blood and 45% said Fever is major symptoms of TB. In addition to these other symptom mentioned by respondents were weight loss (34%), Pain in the chest (26%), loss of appetite (15%) and night sweat 4% respectively. A heartening fact was that the opinion leaders were well aware about the transmission mode of spreading of TB since 78% knew that it spreads through the air when the infected person cough or sneezes. In addition, 35% assumed that it could also spread by sharing food with infected person and 23% believed by sharing bed/clothes with infected persons, as low and 13% said that it could also spread by shaking hands with infected persons. The responses clearly shows that a sizeable number were still unaware about transmission mode of Tuberculosis, a matter of concern because the opinion leaders are the very people who were supposed to educate masses and work on grass root level to mitigate dreaded diseases like TB. Almost 80% of the respondents said that the best way to diagnose TB is to conduct a Sputum smear test, while 67% said that X-ray could also be one way to diagnose the TB. Table 5.2: Knowledge of Opinion Leaders on TB, Symptoms, mode of transmission and diagnosis of Tuberculosis
Characteristics Heard of TB Spontaneous Recall (TB Included in the top health priorities of their community) On Probing Symptoms of Tuberculosis A cough of 2 weeks Coughing up blood Fever Weight loss Pain in the chest Loss of appetite Night sweat Mode of Transmission Through the air when the infected person cough or sneeze Through sharing food with infected person By sharing bed/clothes with infected person 110 84 106 74 98 71 86 87 400 78 N North % 14 100 87 38 37 29 17 7 3 East N 37 106 82 69 55 24 41 13 4 % 26 100 82 69 55 24 41 13 4 N West % 19 100 91 54 44 40 20 20 3 South N % 32 67 58 11 27 29 15 13 4 32 100 95 18 44 48 25 21 7 Total N % 113 398 319 172 163 122 93 53 14 22 100 88 48 45 34 26 15 4
18 113 90 39 38 30 17 7 3
26 112 89 53 43 39 20 20 3
39 23
30 18
54 26
38 18
44 50
32 36
44 20
44 20
181 119
35 23
61
Characteristics Through handshake with infected person Don't Know Diagnosis of TB Sputum smear Test X - Ray Monteux Skin Test DK/CS Total
North 10 8 8 6 10 13
East 7 9
West 21 15 15 11
South 25 7 25 7
Total 66 43 13 8
111 78 5 4 131
85 60 4 3
106 102 6 8 143
74 71 4 6
120 85 6 9 138
87 62 4 7
70 76 7 3 99
71 77 7 3
407 341 24 24 511
80 67 5 5
5.2
KNOWLEDGE ON TREATMENT OF TB In view of the fact that Opinion Leaders play a vital role in making people understand about issues which affects them in some way or other and sensitizes the community at large it is decisive to know their awareness on treatment for TB patients when required. Table 5.3 shows how the Opinion Leaders envisage when a person get diseased by Tuberculosis. The leaders opined on various approaches of medicinal practices to cure a TB patients. A little above two third (67%) showed their faith in Allopathic medicines to treat someone diseased with TB. While almost 34 % precisely mentioned DOTS therapy for treatment, besides this some of the opinion leaders believed that a TB patient can also be cured by Herbal Remedies (7.2%), Ayurvedic Treatment (6.5%) and Homeopathy (4.3%). Further they were asked about the duration of the treatment and 62% said that it takes around 6-8 months to cure TB, while there are 11 % of them felt that it takes more than 8 months for the treatment. 13 % of these leaders felt that TB is curable within the time period of 1-5 months and almost 10% of the people were ignorant about the time required for a TB person to cure. Though these opinion leaders are pivotal in disseminating any pertinent information among communities it is a matter of grave concern that only 59 % of them have heard about the DOTS which is a key feature of RNTC Programme. Though when the same respondents who answered in affirmation about knowledge of DOTS were again asked about the places where this treatment is available 84 % of them were well aware that this treatment is available in government hospital and 26 % said that there are DOTS Centre/Providers for specifically providing DOTS to the TB patients.
62
Table: 5.3: Opinion leaders Knowledge on treatment of tuberculosis
Characteristics Consider TB as a fully curable disease Heard of DOTS Treatment of Tuberculosis* Allopathic medicines DOTS (specifically mentioned) Herbal Remedies Ayurvedic Homeopathy DK/CS Duration of Treatment Less than 2 weeks 2-4 weeks 1-5 months 6 -8 months More than 8 months and others DK/CS Place of TB diagnosis and treatment Government Hospital DOTS provider/Centre Private Hospital NGO DK/CS Total North N 123 69 103 32 5 3 2 5 0 1 12 74 30 14 % 94 53 79 24 4 2 2 4 0 1 9 57 23 11 East N 136 86 103 46 13 4 6 2 1 4 21 89 14 14 % 95 60 72 32 9 3 4 1 1 3 15 62 10 10 West N 129 110 61 79 9 15 7 1 0 3 21 102 8 4 % 93 80 44 57 7 11 5 1 0 2 15 74 6 3 South N 80 35 75 14 10 11 7 2 7 1 14 54 5 18 % 81 35 76 14 10 11 7 2 7 1 14 55 5 18 Total N 468 300 342 171 37 33 22 10 8 9 68 319 57 50 % 92 59 67 34 7 7 4 2 2 2 13 62 11 10
55 7 3 2 1 131
80 10 4 3 2
78 35 2 1 3 143
91 41 2 1 4
95 20 1 2 6 138
86 18 1 2 6
24 16 1 1 5 99
69 46 3 3 14
252 78 7 6 15 511
84 26 2 2 5
*Multiple Answers 5.3 KNOWLEDGE AND PRACTICES- ROLES PLAYED BY OPINION LEADERS All across 91% of the community leaders were aware that a person having symptoms of TB can go to government hospital to diagnose for TB and 5 percent each voiced for DOTS/TB centre and Private Hospital for detecting TB. The following table deals with how opinion leaders counselled on issues when they were asked to opine in a situation where a person was suffering from TB or shown symptoms of the diseases. For this Leaders were asked about the recommendations made for TB patients and 87% advised them to visit a government hospital having DMC facility and 15% specifically asked them to visit a DOTS/TB centre.
63
But when asked about being aware of anyone in family or neighbourhood suffering from TB in the last two years just above one third of the respondents (37%) answered positively though, the response varied from 47% in Northern region to only 22% in Western region. The Opinion leaders in the community are expected to build a conducive environment for issues which affect the population at large so they were asked that weather they have taken any initiative towards generating awareness about TB and DOTS within the society for which only 22% affirmed that in some way they have played some role which drops down to around 10% in the southern region and highest is in Northern region with 24%. The same respondents were then asked about what kind of role they played, 38% said they have worked as DOTS provider, 21% had suggested free treatment with ASHA/ANM, 17 % organized lectures/seminars/workshops to enlighten people about TB and the same percentage of people organized awareness camps (table 5.4). Table 5.4: Awareness of the opinion leaders on the availability of diagnostic and treatment facilities and the role played by them in their community to address TB
Characteristics Place for TB Diagnosis Government Hospital (DMC) Private Hospital DOTS/TB centre Place for TB Treatment Government Hospital (DMC) Private Hospital DOTS/TB centre Knows anyone suffer from TB Advice Given to visit Government Hospital Private Hospital Role in creating awareness for DOTS Activities undertaken Worked as DOT provider Suggestions for free treatment, visit ASHA,ANM Organized lectures /Seminars/ Workshops Organized camps Organized rallies Total 55 6 32 90 10 24 53 11 39 83 17 27 30 0 32 100 0 23 31 2 10 97 3 10 169 18 113 90 10 22 115 9 9 61 88 7 7 47 126 8 17 64 88 6 12 45 115 3 41 30 83 2 30 22 88 8 11 32 89 8 11 32 444 28 78 187 87 6 15 37 North N 120 7 4 % 92 5 3 N 126 9 8 East % 88 6 6 N 130 0 8 West % 94 0 6 South N 88 7 4 % 89 7 4 Total N 464 23 24 % 91 5 5
10 12 1 6 3 131
31 38 3 19 9
12 6 13 7 1 143
31 15 33 18 3
17 5 4 5 1 138
53 16 13 16 3
4 1 2 2 1 99
40 10 20 20 10
43 24 20 20 6 511
38 21 18 18 5
64
Table 5.5:Summary of Key KAP survey Indicators of Opinion Leaders
Characteristics Spontaneous Recall (TB Included in the top health priorities of their community) Heard of TB Mode of Transmission: Through the air when the infected person cough or sneeze Know that the major Symptom of TB is Cough of 2 weeks or more Know that Sputum smear Test is necessary for the diagnosis of tuberculosis Consider TB as a fully curable Disease Heard of DOTS Know that TB the treatment of TB is through Allopathic medicines Know that the duration of TB Treatment is 6-8 months Know that treatment of TB is available at Government Hospital Have played a Role in creating awareness for DOTS Total North N 18 131 110 % 14 100 84 N 37 141 106 East % 26 100 74 West N 26 138 98 % 19 100 71 South N 32 99 86 % 32 100 87 N 113 511 400 Total % 22 100 78
90
87
82
82
89
91
58
95
319
88
111 123 69 103 74 55 32 131
85 94 53 79 57 80 24
106 136 86 103 89 78 39 143
74 95 60 72 62 91 27
120 129 110 61 102 95 32 138
87 93 80 44 74 86 23
70 80 35 75 54 24 10 99
71 81 35 76 55 69 10
407 468 300 342 319 252 113 511
80 92 59 67 62 84 22
65
CHAPTER 6 NON-GOVERNMENTAL ORGANIZATION/COMMUNITY BASED ORGANIZATION
6.1
GENERAL PROFILE OF NGO/CBO FUNCTIONARIES This chapter elaborates the role played by Non-Governmental Organizations/Community Based Organizations (NGO/CBO) by collecting information on Knowledge, Attitude and Practices on TB, stigma and discrimination and the role in referring TB patients or initiatives taken by them for the suffering group or in creating awareness in the society. These NGO/CBOs were selected on the basis of their presence and work in the 30 districts. They were identified based on the information given by the opinion leaders and other community members. For this a total 51 NGOs/CBO were identified to be working in the 300 primary sampling units of the 30 districts. Their head of the organisations were interviewed. Out of the representatives interviewed 40 were males and 11 were females. Most of the representatives interviewed (49%) were in the age group of 35-46, whereas 28% of them were more than 46 years and only 2 were in the age group of 18-25 years. Interestingly as high as 41% of these representatives s were having experience of 1-5 years and only 16% were employees having experience of 16 years or more. NGOs approached for this study were from all across the country, 20% of the organizations were working for last 1-5 years, while 26% were operational for last 610 years and more than 50% of the organizations were in field for last 11 years or more. NGO/CBOs were also asked about the thematic areas of working and most of them were working on multiple areas and themes. When asked in detail 51% said that they are working on TB specific/DOTS programme. Education (55%), Health and diseases related issues (45%) are other themes that these organisations were working for. Besides these, few other prominent thematic areas where the organizations were working were Rural Development (33%), Sanitation (43%), Domestic violence/Gender issues (35%) and Environment (4%) etc. Table 6.1: General Profile of NGO/CBO representatives identified for the KAP Survey
Characteristics Gender Male Female Age 18-25 years 26-35 years 36-45 years More than 46 yrs 0 2 3 3 0 25 38 38 1 2 11 4 6 11 61 22 0 4 5 3 0 33 42 25 0 3 6 4 0 23 46 31 1 11 25 14 2 22 49 28 North N 6 2 % 75 25 N 18 0 East % 100 0 West N 10 2 % 83 17 South N 6 7 % 46 54 N 40 11 Total % 78 22
66
Characteristics Years of Experience of NGOs 1-5yrs 6-10yrs 11-15yrs 16-20yrs More than 21 yrs Year of Experience of NGO Representatives 1-5 yrs 6-10 yrs 11-15 yrs 16-20yrs Area of working of their NGOs* TB specific/ DOTS program Rural Development Sanitation Education Other Health & Disease Related issues Domestic violence/Gender Employment Environment Total
North 0 3 1 3 1 0 38 13 38 13 4 4 1 6 3
East 22 22 6 33 17
West 1 3 5 3 0 8 25 42 25 0
South 5 3 2 0 3 39 23 15 0 23 10 13 9 12 7
Total 20 26 18 24 14
2 3 1 2
25 38 13 25
5 6 1 6
28 33 6 33
5 7 0 0
42 58 0 0
9 3 1 0
69 23 8 0
21 19 3 8
41 37 6 16
4 0 4 8 6 2 1 2 8
50 0 50 100 75 25 13 25
12 6 5 6 5 4 4 0 18
67 33 28 33 28 22 22 0
1 8 7 9 7 8 0 0 12
8 67 58 75 58 67 0 0
9 3 6 5 5 4 2 0 13
69 23 46 39 39 31 15 0
26 17 22 28 23 18 7 2 51
51 33 43 55 45 35 14 4
* Multiple answers possible 6.2 NGO/CBOS KNOWLEDGE, ATTITUDE & PRACTICES ON TUBERCULOSIS The Non-Governmental Organizations working on various themes including tuberculosis were enquired on TB related knowledge. It is perceived by more than three fourth of the NGO functionaries (78%) that Tuberculosis is indeed a serious diseases for a country like India and a dreaded threat to the health of the people. When asked about their opinion on whether TB diseased person can be treated completely or any specific treatment available for TB 100 % of the respondents answered in affirmation. More than 90 % had heard about DOTS and the awareness about government providing DOTS free of cost is also known to more than 90 % people. In view of the fact that these organization are working in the field of Tuberculosis their valued knowledge level is an asset for the society.
67
Table 6.2: Knowledge about Tuberculosis among NGO functionaries
Is TB serious Diseases in India N % YES NO DK/CS 40 11 -78 22 -TB diseased person can be treated N % 51 00 -100 00 -Is any specific treatment available for TB N % 51 00 -100 00 -Heard of DOTS N 46 5 -% 90 10 -Aware that Govt. is providing DOTS free of Cost N % 46 4 1 90 8 2
The respondents were questioned on their Knowledge, Attitude and Practices on Tuberculosis and their response on various activities undertaken by their NGOs. All the respondents answered positively that they have heard about TB and when asked to mention few symptoms of the disease, 94% stated that A cough of two weeks is a major symptom, other prominent symptom singled-out were Coughing up of blood (61%), Fever (55%), Weight loss (43%), Pain in the chest (35%) and Loss of Appetite (20%). On the issue related to mode of transmission 92% said that it could be transmitted through the air when the infected person cough or sneeze. 37% also believed that it could also spread through sharing of food with infected person and 28% believed this by sharing bed/clothes of TB patients. Though regionally, level of awareness differed; in Northern region it was only 13 % and as high as 58 % in Eastern region believed that sharing bed/clothes with infected person could infect others also. Some of them even thought that it can also spread through handshake (6%). When the respondents were asked for the various means to diagnose TB, 92% said that Sputum Smear Test could be used to detect the disease, and 80% of them also said that X-Ray could be another way of identify a TB diseased person. 11% also suggested Blood test as a method to diagnose TB. Table 6.3: NGO/CBO Representatives Knowledge on TB Symptoms, Mode of transmission and Diagnosis of Tuberculosis
Characteristics N Symptoms of Tuberculosis* A cough of 2 weeks Coughing up blood Fever Weight loss Pain in the chest 6 5 7 2 3 75 63 88 25 38 17 12 6 8 8 94 67 33 44 44 12 6 9 5 5 100 50 75 42 42 13 8 6 7 2 100 62 46 54 15 48 31 28 22 18 94 61 55 43 35 North % N East % N West % N South % N Total %
68
Characteristics Loss of appetite Night Sweat Mode of Transmission* Through the air Through sharing food with infected person By sharing bed/clothes with infected person Through handshake with infected person Diagnosis of TB* Sputum smear Test X - Ray Mantoux Skin Test Blood test Total 7 3 1 0 2 0
North 25 0 88 38 13 0 1 1
East 6 6 89 44 0 6 5 0
West 42 0 92 25 58 0 2 1
South 15 8 100 39 46 15 2
Total 10 20 4 92 37 28 6
16 8 0 1
11 3 7 0
13 5 6 2
47 19 14 3
8 7 1 1 8
100 88 13 13
16 14 1 3 18
89 78 6 17
12 9 3 1 12
100 75 25 8
11 11 3 1 13
85 85 23 8
47 41 8 6 51
92 80 16 12
*Multiple Answers The respondents were also asked about different types of the treatment they think could be possible to cure TB and the duration required for this and where one should go for DOTS. A little below two third (65%) of the respondents precisely advised for DOTS and almost half of the respondents said that Allopathic medicines could be a way to treat a TB patients, while 6% suggested for Ayurveda and Homeopathic treatment for Tuberculosis. More than 80% said that it requires 6-8 months to treat TB patients. At the same time when inquired for the different places of DOTS treatment almost 86% suggested for government hospital while around 6-8 % recommended for CHC/PHC. Table 6.4: NGO/CBO Representatives Knowledge on TB treatment, duration and DOTS
Characteristics Know that TB is fully curable Treatment of Tuberculosis DOTS (if specifically mentioned) Allopathic medicines Ayurvedic Homeopathy Duration of Treatment North N 8 % 100 N 18 East % 100 N 12 West % 100 N 13 South % 100 N 51 Total % 100
5 3 0 0
63 38 0 0
10 9 1 1
56 50 6 6
10 6 0 1
83 50 0 8
8 8 2 1
62 62 15 8
33 26 3 3
65 51 6 6
69
Characteristics
North N % 0 75 25 0 N 2
East % 11 78 11 0 N 0 11 0 1
West % 0 92 0 8 N 0
South % 0 77 8 15 N 2 41 5 3
Total % 4 80 10 6
1-5 months 6-8 months More than 8 months DK/CS Place of TB treatment Any Government Hospital CHC/PHC DOTS centers Total
0 6 2 0
14 2 0
10 1 2
8 0 0 8
100 0 0
17 0 1 18
94 0 6
8 1 3 12
67 8 25
11 2 0 13
85 15 0
44 3 4 51
86 6 8
6.3
ROLE OF THE NGOS Non-Governmental Organizations play a crucial role when it comes to reaching out to the masses in terms of their role in spreading the massages and making people aware on various issues. Since many of these organizations sometimes have dual role as they provide health services through the health centres operated by them vis--vis working at community level by spreading massages in the course of the IEC activities or being engaged at various platforms by means of Policy/Advocacy, organizing workshops/seminars etc. Thus the Knowledge, Attitude and Practices of NGO/CBOs functionaries essentially makes significant difference in the community level awareness. As more than half of the organizations asserted that one of the major areas of their functioning is TB specific/DOTS programme, when asked where they will recommend a person to go for diagnosis if he is suspected for TB, almost 85% said that they will advise them to visit a Government Hospital. Same is the response for TB Treatment also as 80 % of the respondents suggested government hospital for a patient diagnosed with TB and around 16% specifically said that they will recommend a DOTS/Tb centre for a TB patient. Though when asked for anyone in their family or neighbourhood suffering from TB in last two years only 49% at national level affirmed but regionally huge variations were found when only 25 % in the Western region and 28% in Eastern region said knowing someone in neighbourhood suffering from TB while in Southern and Northern region it is as high as 85 and 75% respectively. The same respondents were then asked as to what advice was given to these TB diseased people and 92% said that they recommended for the Government Hospital.
70
More than half (57%) of the respondents have taken initiatives in one way or other within their community to generate awareness on issues related to TB and DOTS. A range of activities were undertaken by the NGOs for this that includes organizing camps (52%) acting as DOTS service provider (41%), workshops/seminar/conferences (41%) and also street plays and pamphlet distribution in almost 25% cases Table 6.5: Activities done by NGO/ CBO representatives on the addressing TB in their localities
North N Suggested a Place for TB Diagnosis Government Hospital (DMC) Private Hospital DOTS/TB centre Suggested a Place for TB Treatment Government Hospital (DMC) Private Hospital DOTS/TB centre Knows anyone suffer from TB Advice Given to visit Government Hospital Private Hospital Role in creating awareness for DOTS (in the last two years) Activities undertaken Organized camps Organized rallies Organized lectures /Seminars/ Workshops Worked as DOT provider Nukkad Nataks/ Street Plays/Skits Awareness Activies, pamphlet distributing Video Shows Total 3 0 3 3 4 1 0 8 60 0 60 60 80 20 0 5 0 6 3 1 4 1 18 46 0 55 27 9 36 9 0 0 1 3 0 1 0 12 0 0 20 60 0 20 0 7 6 2 3 2 1 0 13 88 75 25 38 25 13 0 15 6 12 12 7 7 1 51 52 21 41 41 24 24 3 5 1 5 83 17 63 5 0 11 100 0 61 3 0 5 100 0 42 10 0 8 91 0 62 23 1 29 92 4 57 7 0 1 6 88 0 13 75 14 2 2 5 78 11 11 28 8 0 4 3 67 0 33 25 12 0 1 11 92 0 8 85 41 2 8 25 80 4 16 49 7 0 1 86 0 14 14 2 2 82 6 12 8 0 4 75 0 25 12 0 1 100 0 0 41 2 8 85 2 13 % N East % West N % South N % Total N %
71
6.4
COMMUNITY PARTICIPATION- NGO/CBOs To understand the level of community participation and the reasons which inhibit community based organizations to work on issues related to Tuberculosis prevention, care and treatment they were inquired on various aspects. Almost half of the organizations were having TB/DOTS programme as one of their thematic areas and were doing a range of activities to address this including educating community partners on its prevention and treatment in 88% cases, providing community based care in 61%, working for reducing stigma and discrimination in 23% and also engaged in many other activities like resettlement of TB patients, imparting training and working as DOTS provider etc. When asked for the involvement, almost half of the NGOs were aware about the RNTCP scheme but the awareness among NGOs/ in Eastern regions was poor where only 33% knew about RNTCP. 41% of the NGOs were collaborating in some way or other in different schemes under RNTCP although the participation by Southern region NGOs was relatively higher (62%). On the question of collaboration for working in the field of Tuberculosis 85% showed their willingness to join hands but they cited many reasons for not aligning with RNTCP. For instances limited or insufficient funds under the scheme is an hindrance for 61% of the organization or for 38% there are not many people suffering from TB within the geographical region of their working. Table 6.6: Community Participation NGO/CBOs (Multiple Response*)
Percentage of NGOs working in Area of Tuberculosis Activities Undertaken by NGOs Spread Awareness on TB Provide community based care Provide Training to TB health care Reduce stigma and discrimination Help Resettlement of TB patient Motivating TB patient to treat DOTS Spread Awareness Worked as a DOTS provider Awareness of RNTCP PPM schemes Involvement in these Scheme Kind of Scheme 3 3 0 2 0 4 3 0 6 2 75 75 0 50 0 100 75 0 75 25 11 7 3 3 1 2 0 0 6 6 92 58 25 25 8 17 0 0 33 33 0 0 0 0 0 1 1 1 6 5 0 0 0 0 0 100 100 100 50 42 9 6 3 1 2 3 2 1 8 8 100 67 33 11 22 33 22 11 62 62 23 16 6 6 3 10 6 2 26 21 89 62 23 23 12 39 23 8 51 41 North N % 4 50 East N % 12 67 West N % 1 8 South N % 9 69 Total N % 26 51
72
North ACSM (Advocacy, Communication & Social Mobilization) SC Scheme (Sputum Collection Center) DMC (Designated Microscopy Centers) LT Scheme CS Scheme Adherence Scheme Willing to collaborate with RNTCP program Total 2 0 0 0 0 0 8 8 100 0 0 0 0 0 100 5 0 0 0 0 1
East 83 0 0 0 0 17 78 18 4 1 1 0 1 0
West 80 20 20 0 20 0 83 12
South 6 1 0 1 0 3 11 13 75 13 0 13 0 38 85
Total 17 2 1 1 1 4 43 51 30 4 2 2 2 8 84
14
10
73
CHAPTER-7 STIGMA AND DISCRIMINATION 7.1 CONCEPTUAL FRAMEWORK Stigma is literally a "mark" or "blemish" upon someone or something. Tuberculosis is often negatively viewed, and social attitudes may be damaging to those infected or suspected of being infected due to its association with HIV. Discrimination is defined more in terms of legal and human rights: when a person loses a job because of the negative connotation, overt discrimination has taken place. Some experts and organizations consider discrimination as an outcome of the process of stigmatization.4
Stigma is an attribute that is deeply discrediting and results in the reduction of a person or group from a whole and usual person to a tainted, discounted one (Goffman, 1963). Thus, the ultimate effect of stigma, as noted by Goffman, is the reduction of the life chances of the stigmatized through discriminatory actions.
In keeping with Goffman, we do not Conceptualize discrimination as separate from stigma, but as the end result of the process of stigmain effect, enacted stigma. We define discrimination (or enacted stigma) as the negative acts that result from stigma and that serve to devalue and reduce the life chances of the stigmatized. A somewhat different definition of the word discrimination may be used by the legal or human rights communities in their work on HIV-related discrimination and relevant laws and policies (Carael et al., 2000).
Stigma and discrimination, but especially the former, are among the most difficult aspects of the epidemic to quantify. It is perhaps for this reason that, while many prevention and care programmes have the reduction of stigma and the fostering of more supportive attitudes as a stated objective, virtually none has developed a reliable way of measuring this most intangible of phenomena. In the first place, no clear definitions exist of stigma or the qualities that characterize it, and if something cannot be clearly defined then it cannot be accurately measured. While some stigmatizing attitudes and discriminatory practices are all too obvious, others remain largely hidden. There is no clear relationship between attitudes and behaviour in this context.
USAID Stigma and Discrimination Indicators Working Group
74
To complicate matters still further, active discrimination is sometimes difficult to discern. It can take highly visible forms such as being fired from a job. But it can also make itself felt in the failure to provide services available to other members of society, or even the absence of compassion and supportive advice from religious or community leaders. It is difficult to collect information about behaviour towards those with TB. It is not clear to what extent hypothetical willingness to care for a sick family member is matched in practice, or, indeed, to what extent it is a useful indicator of social stigma. However, for want of anything better, hypothetical questions about people's attitudes are likely to remain central to attempts to track changes in negative attitudes towards people with TB. 7.2 ASSESSING STIGMA AND DISCRIMINATION AMONG GENERAL POPULATION Drawing from the report of existing studies, we identified following key domains to quantitatively measure stigma and Discrimination Fear of casual Transmission and refusal of contact with TB patients Domains of Stigma & Discrimination
Disclosure (among profession al, peer group)
Enacted Societal Stigma (Discrimination)
Values, shame, blame & Judgment
75
Each domain and the indicator used to measure it are given in the detail Fear of Casual Transmission and Refusal to contact with TB patients The label of this domain reflects both the direct underlying cause of stigma (fear of transmission) and the resulting stigmatizing action (refusal of contact with people suffering from TB). The indicators for this domain measure the actual fears that individuals hold about transmission of TB through non-invasive routes Proportion of people who think that family of TB patients should not be allowed to participate in social function Proportion of People who think that children suffering from TB should not be allowed to go the school Proportion of people who think that children of parent suffering from TB should not be allowed to go to school Proportion of people would not like to share their meals with the TB diseased person
7.3
VALUES - SHAME, BLAME AND JUDGMENT A second, equally important causal domain of S&D for measurement is moral- or value-driven stigma where assumptions and judgments are made about how diseased with TB, which are manifested in stigmatizing attitudes. The indicators used to measure this domain are: Proportion of People felt that TB patients are threat to community Proportion of People felt that TB patients should be left isolated in the community Proportion of people felt that they left their family members suffering from TB isolated
Enacted Stigma The term Enacted Stigma is used to capture a wider set of actions than typically are associated with discrimination. Discrimination often is understood to mean unlawful acts of exclusion, or abuse that occurs in formal institutional settings (such as dismissal from employment or refusal of health care). The broader term used here is meant to include important stigmatizing actions that are not usually captured under the term discrimination, such as gossip, social or physical isolation, or loss of business clientele due to ones TB status. The following indicators were used for measuring this domain:
76
Proportion of people who think that married female TB patients should be sent off to parents house Proportion of people would not like to take female member suffering from TB patient to hospital Proportion of people would not marry their daughter to a boy known to be suffering from TB Proportion of People would not marry their son to a girl knows suffering from TB
Fig 7.1: Fear of casual Transmission and refusal to contact with TB persons among General Population
The graph shows that among the overall general population majority of the respondents do not express their fear of transmission by intermingling with the family of the TB diseased persons. But, people did express their fear that TB can be spread through sharing of food with infected person. As high as 81% of respondents showed their disagreement towards sharing of food with TB diseased person. There was no major difference observed in the zone wise variation except fear of transmission was found to be lowest in southern region. Fig 7.2:Value, Shame, Blame and Judgment The responses among the total general population (n=3823) related to shame, blame and judgement present a mixed picture. While on one hand around 40% of respondents agreed to this statement that TB patients are threat to their community, blaming TB patients for their illness. But they also expressed support to them.
77
Around 70-80% of respondents agreed to the statement that they do not want to isolate their family members suffering from Tuberculosis. Overall the tendency to judge and blame was higher in western region (63%) while it is found to be lowest in the southern region (15%). Fig 7.3: Enacted Stigma (Discrimination) Discrimination against girls or women is a devastating reality. The graph shows that majority of the respondents do not support rejection of female members. Long lasting illness of TB also likely to impact the marriage prospects of those planning to get married. Quite a large number of people agreed to the statement that they would not like to marry their son or daughter to any person known to have suffered from TB. Stigma and Discrimination Experienced by TB patients Indicators used to Measure Stigma and Discrimination experienced by diseased persons Drawing from the report of existing studies, we identified following key domains to quantitatively measure stigma and Discrimination Each domain and the indicator used to measure it are given in the detail Fear of Casual Transmission and Refusal to contact with TB patients The label of this domain reflects both the direct underlying cause of stigma (fear of transmission) and the resulting stigmatizing action (refusal of contact with people suffering from TB). The indicators for this domain measure the actual fears that individuals hold about transmission of TB through non-invasive routes Proportion of people do not want to have meal with you after knowing your disease status Proportion of People refuse to enter your house after knowing your disease status
78
Proportion of People refuse to shake hands with you after knowing your disease status Proportion of people think that TB diseased males get married easily Proportion of people think that TB diseased females get married easily
Enacted Stigma The term Enacted Stigma is used to capture a wider set of actions than typically are associated with discrimination. Discrimination often is understood to mean unlawful acts of exclusion, or abuse that occurs in formal institutional settings (such as dismissal from employment or refusal of health care). The broader term used here is meant to include important stigmatizing actions that are not usually captured under the term discrimination, such as gossip, social or physical isolation, or loss of business clientele due to ones TB status. The following indicators were used for measuring this domain: Proportion of people disclosed their TB status among the employers Proportion of people changed their Job after disclosure of TB status Proportion of people experienced discriminatory change in relationship Proportion of People experienced discriminatory change in friends
Disclosure Disclosure often is considered a proxy measure for S&D, with the assumption that where S&D is low, disclosure will occur more often and among a wider group of individuals. The following indicators were used for measuring this domain: Proportion of people who informed their disease status to the friends Proportion of people who informed their disease status to the family members Proportion of people disclosed their TB status to the employers
The indicators used for defining and measuring Stigma and discrimination indicator have been explained in detail in the above section. This section presents the analysis of findings of the three main domains of Stigma and Discrimination Fig 7.4: Fear of casual Transmission and refusal to contact with TB diseased persons The chart shows that majority of the TB diseased persons have not faced refusal of contact in any form by their friends. However, some of the respondents indicated the stigmatized action by refusal of sharing of mean by their friends.
79
There was no major difference observed in the zone wise variation except fear of transmission was found to be lowest in southern region. But relatively higher proportion of respondents from rural areas expressed their discriminatory attitude of people towards them. Fig 7.5: Enacted Stigma (Discrimination) Abuse and Rejection The responses on the enacted stigma present a mixed picture. Although majority of TB diseased persons had not faced any kind of discrimination abuse and rejection from the family members and friends. But disclosure of the disease status seems to be problem especially with employers. Around 60% of the respondents had not disclosed their TB status. Around 12% had to change their jobs after disclosing their disease status.
Fig7.6: Disclosure Disclosure is considered as a proxy measure for stigma and discrimination with the assumption that where S&D is low, disclosure will occur more often and among a wider group of individuals. In the present study, majority of the TB diseased persons informed that they had disclosed their TB status to the family members while close to 70% had informed among friends. Fig 7.7: Opinion Leaders Perspective on Stigma and Discrimination Disclosure to employer seems to be a problem as nearly two third of the TB diseased persons had not disclosed their status to their employers.
80
The fact that self-disclosure by TB diseased person among their employer is not common is an indication of stigma and discrimination in the area surveyed. The willingness to disclose their disease status was relatively higher among males as compared to females. But disclosure among family members was found to be more or less similar among both males and females. There is no distinct zone wise variation existed in the disclosure status of the TB diseased person. Fig 7.8: Fear of Causal Transmission The fear to get infected with TB instigate many to indulge in such a way which is discriminatory in nature and harm in sharing food with with TB diseased people, while almost half of the respondents refrained in doing so. Though the fear ir clearly evident but when the respondent were asked about their participation in society we found that 64 percent asserted that there should no be any discrimination with daily wage labourers suffering from TB. Similarly on the issue of family with TB patient should allowed to be part of any social function or children diseased with TB should allowed to go to the school 71 percent and 58 percent respectively felt that there should not be any discrimination with diseased people. Fig 7.9: Value, Shame, Blame and Judgement On many occasions people become judgemental with issues which might bring ignominy to their family. It was apparent with the fact that when questioned that whether female suffering from TB face any problems in their marriages more than half of the respondent (54%) confirmed the same.
81
Stigma and discrimination exists irrespective of the gender differences since people said they will not marry their daughter or son with someone who is suffering from TB in 34 and 33 percent cases respectively. Also a matter of grave concerne is that almost a little less than one fourth (22%) believed in isolating their family members if diseased with tuberculosis. As perceived most profounding unit in the society any form of discrimination at family is bound to affect TB patients at social, physical and mental level. Fig 7.10: Enacted Stigma If any civil society stigmatize some of its memebr at any level be it in institution like marriage or at family facade that reflects the cultural and social practices of that society. As opinion leaders are not only instrumental in constructing the views of the society they also echo the sentiments and ideas of the people, expression made by them are critically important to understand attitude and practices of the society. To understand when asked if any female member is suspected for TB, 90 percent said that they will take her to hospital. Similarly when inquired weather feamle accompany their spouses suffering from TB to hospital or DOTS centre 66 percent strongly agreed with that, while only 55 percent husband/In-laws strongly agreed on accompaning female TB patients to the hospital. About married female TB patients, 84 percent felt that they should not be sent to their parents home and stay with there husband/In-laws family.
82
Fig 7.11: Opinion of NGO Representatives on Stigma and Discrimination Fear of Causal Transmission On the issues of Stigma and discrimination surprisng revelation came up in the study. Though it was observed that the knowledge is comparitively high among NGO/CBOs functionaries as compared to other respondents but so is the stigmatization and discrimination against TB diseased people. As shown only 43 percent said that they have no problem in sharing their food with TB diseased people which means more than half of the population is reluctant in sharing their meals with TB patients. Situation is grim when it comes to discrimination against daily wage labourers suffering from TB as only just above half of the respondents (51%) believed that there should not be any inequity against them. The response was not very enthusiastic when asked for family and children as only 69 percent and 67 percent respectively felt that there should not be any discrimination with diseased people. Fig 7.12: Value, Shame, Blame and Judgement Civil Society Organizations are not mere implementing organization engaged in working on various social issues, to some extent they are mirror of the society and represents the sentiments of the society. So on many occasions ideas and views expressed by these organizations are also views of the people in large. On the issue of females suffering from TB facing problems in their marriage 55 percent believed that they do have difficulties in their marriages.
83
Stigma and discrimination exists irrespective of the gender differences as evident from the fact that people said they will not marry their daughter or son with someone who is suffering from TB in 35 percent cases respectively. Also what was concerning is the fact that a little less than one fourth (22%) believed in isolating their family members if diseased with tuberculosis. Fig 7.13: Enacted Stigma Stigmatization at at any level be it in institution like marriage or at family facade that reflects the cultural and social practices of that society. Opinion made by NGO/CBO leaders is critically important to understand attitude and practices of the society. To understand when asked if any female member is suspected for TB 90 percent said that they will take her to hospital. Similarly when inquired weather feamles accompany their spouses suffering from TB to hospital or DOTS centre 73 percent strongly agreed with that, while only 55 percent husband/In-laws strongly agreed on accompaning female TB patients to the hospital. About married female TB patients 88 percent felt that they should not be sent to their parents home and stay with there husband/In-laws family.
84
ANNEXURE
85
GENERAL POPULATION
Baseline KAP Survey on Tuberculosis- Project- OXYGEN ________________________ ____/_____/2011
QUESTIONNAIRE ID NUMBER DATE OF INTERVIEW STATE: Uttar Pradesh Orissa Kerala TYPE OF SAMPLE 01 06 11 Panjab
02 07 12
Haryana
03
Rajasthan
04 09 14
West Bengal Tamil Nadu Madhya Pradesh
05 10 15
Bihar Andhra Pradesh
Mizoram 08 Karnataka Maharashtr Chhattisgar 13 a h Radom--1
DISTRICT NAME/ ID UMBER_______________________ DISTRICT SPECIFICATION BLOCK Name___________________________ CODE VILLAGE / WARD ___________________________ CODE TYPE OF SETTLEMENT Name of the nearest PHC : Distance from the nearest PHC (kms) GENDER Name of the respondent:
1. TRIBAL
2. NON-TRIBAL
1. RURAL
2. URBAN
1. MALE
2. FEMALE
03/01/11
FIELD CONTROL INFORMATION Interview Yes 1 No 2 By Sign By 2 Sign By 2 Sign Code Code Date of Interview Starting Time of Interview Ending Time of Interview Code AM- 1 PM - 2 AM- 1 PM - 2
Spot / back check Yes 1 No
Scrutiny Yes 1 No
If one or more than one visit made record: Date Time * Status of interview
86
Date of first visit Date of second visit Date of third visit * Refused 1 not available
______________ ______________ ______________ 2
Time:_________ Time:_________ Time:_________
1 1 1
2 2 2 4
3 3 3
4 4 4
Partly Completed 3
Completed
Good morning/evening. I am from GFKMODE, a Social Research Organisation. We conduct surveys on various social issues from time to time. I shall be grateful if you could spare a few minutes and answer a few questions. The reason we want to speak with you is that International Union of Tuberculosis & Lung Disease (The Union) in collaboration with the Government of India TB Programme (RNTCP) is implementing a TB project that is aimed at improving Tuberculosis care and control for the communities. Through this study, we want to get some information on knowledge, attitude & behavior regarding tuberculosis among General Public, so that this information could help design appropriate strategies that will benefit the population. All of your responses will be treated as confidential and will be used only for research purposes and also to help policy makers to understand the bottlenecks in functioning, if any, to streamline the functioning. We shall be thankful for your cooperation. Informed Consent: Your participation in the interview and in every aspect of the study is completely voluntary. If some questions are difficult or make you uncomfortable, we can skip them. You may also ask me to clarify any questions if you do not understand them. You may also decide to stop the interview any time. I would like to assure you that the information provided by you would only be used for the purpose of research and your identity will not be revealed to anyone either in the final report or in any other way. If you have any questions or concerns after we completed the interview, you may ask.
RESPONDENT, KINDLY RESPOND TO HIS/HER SATISFACTION)
Do you have any questions about the survey? (INSTRUCTION TO INVESTIGATOR: IN CASE OF ANY QUESTIONS RAISED BY Would you be willing to participate in this survey? Yes=1 / No=2 Participant:
Name: - ____________________________________ Date: - _____________________________________ Signature or thumbprint: - _____________________
Q. No
SOCIO ECONOMIC & DEMOGRAPHIC CHARACTERISTIC Questions Response
Skip
87
1 2 3 4
What is your Name? ____________________ What is your sex? Male 1 (Observe) Female 2 How old are you? (Age in completed years) What is the last level of education Illiterate 1 that you completed? Literate but no formal education 2 Less than Primary 3 Primary but less than Secondary 4 Secondary but less than Senior Secondary 5 Senior Secondary but not Graduate 6 Graduation & above 7 What is your occupation? Wage laborer 1 Skilled worker 2 Self employed..3 Service (Govt. & Private 4 Business 5 Agriculture/cultivator 6 Unemployed 7 House wife 8 Student / Handicapped/ etc 9 Any other (specify) 10 What is you average household Less than Rs. 2000 1 income per month? Rs. 2001 Rs. 4000 2 Rs. 4001 Rs. 8000 3 Rs. 8001 Rs. 10,000 4 Rs. 10,001 and above 5 DK/CS 6 What is your current marital status? Married 1 Unmarried 2 Divorced 3 Widowed/Widower 4 Separated 5 What is your family type? Single 1 Joint 2 Extended 3 Type of House( By observation) Pucca house 1 Semi-pucca house 2 Kachha house 3 Does your household own this house Yes or any other house? 1 No .2 Does your household have: Yes No Yes No 2 2 L M N A mobile Telephone Any other Type of Phone A computer 1 1 2 2
9a
10
A B
Electricity Mattress
1 1
88
C D E
Pressure cooker Chair A cot or Bed
1 1 1
2 2 2
O P Q
A Refrigerator A Watch or Clock A Bicycle
1 1 1
2 2 2
Q. No F G H I
Questions A table Electric Fan Radio Or Transistor A black Television & white 1 1 1 1 2 2 2 2 R S T U
Response A Motorcycle or Scooter An Animal drawn cart A Car Water Pump (For Agricultural Use) A Thresher (For Agricultural Use)
Skip 1 1 1 1 2 2 2 2
A color Television
K 11
12 13
14 15
A sewing 1 2 W A Tractor(For 1 2 Machine Agricultural Use) What is the main source of drinking Private Tap 1 water for your house? Private Hand Pump 2 (Single code) Public Tap 3 Public Hand Pump 4 Tube Well 5 Supply tanker 6 River/pond/Steam/Waterfalls 7 Rain water 8 Packaged Water 10 Others (Specify_______) 11 Is there a separate Room for Yes 1 cooking? No 2 Type of fuel mostly used for cooking: Electricity 1 Wood 2 Coal/Lignite 3 Kerosene 4 LPG(Gas)/Natural Gas 5 Charcoal 6 Bio-gas 7 Dung Cakes 8 Agriculture Crop Waste 9 Straw/Shrubs/Grass 10 88-Others (Specify____________________) 11 Does your household have a BPL Yes 1 card? No 2 When someone falls sick in your Any Government Health facility (Including family, where do you generally go? PHC/CHC/SC) 1 ASHA 2 Private Clinic / Private Hospital 3
If coded (1) skip to 16
89
Q. No
15 a
16
Response Private Ayurvedic treatment 4 Private Homeopathic treatment 5 Traditional healer/ Quacks 6 Clinic run by NGOs/Trust 7 Any other (Specify)________________________8 Why do you not generally go to Hospital is far from home 1 Government Health facility? Unavailability of doctors 2 (Multiple Response Possible) Unfriendly behavior of health staff 3 4 Long Waiting Hours Lack of Diagnostic facility 5 Lack of Qualified Doctor 6 Lack of Diagnostic Equipments in the facility 7 Unhygienic 8 Private Clinic is nearby 9 Any Other (Specify)_______________________10 Do you suffer from cough of 2 weeks Yes 1 in the last two months? No 2
Questions
Skip
Q17
16 a
If yes, Have you visited any health Yes centre for seeking any treatment or No sputum examination?
1 2
17
KNOWLEDGE AND AWARENESS ABOUT TUBERCULOSIS AND TREATMENT What are the most common diseases TB Mentioned 1 you are aware of? TB Not mentioned 2 If TB is not mentioned, have you heard of TB? If yes, could you mention few symptoms of TB? (Multiple Response Possible) Yes 1 No 2 DK/CS 3 A cough of 2 weeks 1 Pain in the chest 2 Coughing up blood 3 4 Fever Night sweat 5 Weight loss 6 Loss of appetite 7 Any other________________________________8 Dont know 9 Through handshake with infected person 1 Through the air when the infected person cough or sneeze 2 Through sharing food with infected person 3 By sharing bed/clothes with infected person 4 Dont Know 5 Any Other (Specify) 6 Those living in unhygienic condition 1 Poor people 2
18
IF coded (1) then skip to 19 If coded (2) & (3) skip to 44
19
20
Do you know how can a person get infected with TB? (Multiple Response Possible)
21
Who do you think are more prone to get infected with TB? (Multiple Response
90
Q. No Possible)
Questions
22
If a person is suspected with TB, where according to you s/he should go for diagnosis? (SINGLE CODE)
23
If a person is diagnosed with TB, where according to you s/he should go for treatment? (SINGLE CODE)
Response Malnourished 3 Children 4 Women 5 Family members of TB infected person 6 Exposed to cough and cold for long time 7 HIV +ve 8 Smokers 9 Alcoholic 10 Any other 11 DK/CS 12 Government Health Facilities / T.B Hospital 1 Private hospitals/clinics 2 DOTS/TB centers 3 NGOs/ Trust Hospital 4 DK/CS 5 Any other (specify)________________________6 Government Health Facilities / T.B Hospital 1 Private hospitals/clinics 2 DOTS/TB centers 3 NGOs/ Trust Hospital 4 DK/CS 5 Any other (specify)________________________6
Skip
24 25
Do you consider TB as a serious disease? According to you whether TB affected person can be cured?
26
27
27a 28
Yes 1 No 2 Yes, Completely 1 Yes , Partially 2 No 3 DK/CS 4 What is the best treatment for TB? ( Herbal Remedies 1 Single Response Possible) Home Remedies 2 DOTS 3 Other Allopathic medicines/Doctor 4 Ayurvedic 5 Homeopathy 6 Any other (specify)___________________7 Dont Know 8 How long should the treatment be Less than 2 weeks 1 taken to cure TB? 2-4 weeks 2 1-5 months 3 6-8 months 4 More then 8 months (specify) Months_____________________________5 DK/CS 6 IF RESPONSE MORE THAN 8 MONTHS Months _______________________________ THEN SPECIFY THE MONTHS How can TB be diagnosed? Sputum Smear Test 1 (Multiple Response Possible) XRay 2 Mantoux Skin Test 3 4 Any Other (Specify)
Q28
Q28
91
Q. No 29
Questions DK/CS
Response 5 1 2 3 4 5 6 7 8 1 2 3 4 5 6 7 8 1 2 3 1 2
Skip
30
31
32
Are you aware of the place where Government Hospital /T.B Hospital Tuberculosis can be diagnosed? CHC/PHCs (Multiple Response Possible) Private Hospital/Clinic NGO/CBO DOTS CENTRE Designated Microscopic Centre(DMC) Other DK/CS Are you aware of the place where Government Hospital /T.B Hospital one can be treated for Tuberculosis? CHC/PHCs ANM/ASHA/AWW (Multiple Response Possible) Private Hospital/Clinic DOTS CENTRE , DOTS Provider NGO Other DK/CS Is regular and complete treatment for Yes TB important for cure? No DK/CS Have you heard of DOTS? Yes No
If coded 2, then skip to 35
33
34
35
36
37
Are you aware of the place where Government Hospital 1 DOTS is available? CHC/PHCs 2 (Multiple Response Possible) ANM/ASHA/AWW 3 Private Hospital/Clinic 4 DOTS Provider/DOTS Center 5 NGO 6 Other 7 DK/CS 8 Do you know that DOTS is available Yes 1 free of cost? No 2 DK/CS 3 Can you have TB? Yes 1 No 2 DK/CS 3 If no, what are the reasons? I am healthy and strong 1 (Multiple answers) I do not fall sick easily 2 No one in my family has suffered 3 I have not come in contact with a patient 4 I stay away from poor/sick people 5 Others (specify) 6 STIGMA & DISCRIMINATION Now I will make some statements Strongly Somewhat Disagree about People suffering from TB. Agree agree Please let me know how much you agree to these? A family with TB patient should not be allowed to participate in any social 1 2 3 function
Cant Say/Dont Know 4
92
Q. No b c d e f g 38 a b
c d e f
Questions Married female TB patient should be sent off to her parents house Children with TB should not be allowed to go to school Children of parents suffering from TB should not be allowed to go to school Daily wage Laborer, suffering from TB should not be allowed to work TB patient are threat to community TB patients should be left isolated in the community Which of the following you would agree to do? Share a meal with person you know had TB If you suspect one of the female member is suffering from TB, would you take her to hospital Marry your daughter/Sister to a boy knowing had a TB Isolate your family member having TB in the house Marry your son to a girl who you know had TB Send your daughter in law to parents house if she had TB in order to protect other family members from TB
Response 1 1 1 1 1 1 Yes 1 1 1 1 1 2 2 2 2 2 2 No 2 2 2 2 2 3 3 3 3 3 3 DK/CS 3 3 3 3 3
Skip 4 4 4 4 4 4
39 (a)
39 (b)
40
In your community, how is the male Most people reject him 1 suffering from TB usually treated? Friends/Relatives do not accompany him to (Multiple answers) hospital/DOTS centers 2 Face problem in marriage 3 Community support and help him 4 Most people are friendly but they generally try to avoid him 5 His wife accompany him to hospitals /DOTS centre 6 Other_______________________________7 Dont know 8 In your community, how is the Most people reject her 1 female suffering from TB usually Most people are friendly but they generally treated? try to avoid her 2 (Multiple answers) Community support and help her 3 Husbands/in-laws do not accompany her to hospital/DOTS center 4 Husbands accompany her to hospitals /DOTS centre 5 Face problem in marriage 6 Dont know 7 Do you know anyone in your family Yes 1
If coded 2
93
Q. No
Questions /neighborhood suffering from TB No during the last 2 years? DK/CS If yes, have you given any advises to them for treatment? If yes, where have you advised them to go for the treatment?
Response 2 3 1 2 1 2 3 4
Skip & 3 skip to 42
41 (a) 41 (b)
Yes No Government hospital Private hospital DOTS Centre None
Q 42
42
43
Have you ever taken any initiatives towards generating awareness about TB & DOTS within your community? If yes, what are they? (Multiple Response Possible)
Q. No 44
45
46
47
Yes 1 No 2 DK/CS 3 Advised people suffering from cough to go and get checked up 1 Participated in TB awareness 2 rallies/Nautankis/Nataks/Melas etc Worked as DOT provider 3 Other (specify) 4 MEDIA HABIT & PREFERENCES Questions Response Which source of information you are Radio 1 exposed to? (Multiple Response TV 2 Possible- Probe) Newspaper & Magazines 3 Cinema 4 Hoardings/posters/leaflets/Wall painting 5 Melas/ Nukkad Nataks etc 6 Internet/Web advertising 7 Word of mouth (Interpersonal communication) 8 Mobile phone advertising .9 Any Other 10 None 11 IF RESPONDED RADIO IN Q.44, Vividh Bharti 1 Which Station of Radio do you FM( Specify_________________________)2 Community Radio 3 generally listen to? Regional Radio Station_________________4 Other (specify) 5 Which program do you like most on News 1 Radio? Drama / Serial 2 (Single code) Film Songs 3 Folk Songs 4 Discussion on Health 5 Discussion on other any issues 6 Advertisement 7 Other (specify) 8 IF RESPONDED A TV IN Q.44, Which TV Channel watched mostly -----------------------Television channel do you generally TV Channel 2nd most ------------------------------rd watch? (Multiple Response Possible) TV Channel 3 most -----------------------------th TV Channel 4 most --------------------------------Which programs do you like the most News 1
IF coded 2 & 3 skip to 44
Skip Q 45 Q 47
Q 49
48
94
Q. No
49
Questions Response on TV? (Probe for two most liked Drama/Serial programs) Entertainment / reality show Health Related Programs Advertisements Folk music Music Films Sports Other (Specify) Do you read newspaper? Yes No Which language paper generally you English read? Hindi Local language you Newspaper Newspaper Newspaper Have you ever seen/listen any Yes advertisement / information / No DK/CS Message on Tuberculosis or DOTS? If Yes, Where did you see such Radio advertisement or/and information on TV TB/DOTS? (Multiple Response Newspaper & Magazines Possible) Cinema Hoardings/posters/leaflets/Wall painting Melas/ Nukkad Nataks etc Internet/Web advertising Word of mouth (Interpersonal communication) Mobile phone advertising Any Other None What is your most common source of Radio getting health-related information? TV Newspaper & Magazines Cinema Hoardings/posters/leaflets/Wall painting Melas/ Nukkad Nataks etc Internet/Web advertising Word of mouth (Interpersonal communication) Local Health Service providers Mobile phone advertising Any Other None FOR NON AWARE OF TB SKIP TO Q57 From which source have you received Friends any message/Information on TB?( Family MULTI RESPONSE POSSIBLE) Neighbors Colleague Names of the generally read? newspapers
Skip 2 3 4 5 6 7 8 9 10 1 2 1 2 3 1 2 3 1 2 3 1 2 3 4 5 6 7 8 9 10 11 1 2 3 4 5 6 7 8 9 10 11 12 1 2 3 4
If coded 2, skip to Q. 51
50 (a)
50 (b)
51
If coded 2 & 3 , skip to Q. 53
52
53
54
95
Q. No
55 56
Response Teachers 5 Newspaper/Magazines/Leaflets/Wall paint /Bill-boards 6 Posters/Brochures/Other printed materials 7 Radio 8 TV 9 Cinema 10 Local Health Workers/Doctors 11 Internet/Web advertising 12 Interpersonal Communication 13 Others (specify 14 Dont Know 15 Can you recall any message / Yes 1 information on TB? No 2 The message (Record verbatim) If yes, then specify _____________________________________ INFORMATION SOURCES What are your sources of information for awareness on Tuberculosis related issues? (Multiple Response Possible) TV 1 Radio 2 Cinema 3 Newspaper / Magazines 4 Hoarding/Posters/billboards/ Wall writing 5 Internet/ Web Advertising 6 Public service announcements 7 Drama/Skits/Street plays 8 Hospital/doctor 9 Friends & Relatives 10 Teachers/peer educator 11 Health camp 12 Health & related workers 13 DOTS Centre 14 DOTS providers 15 Local Dispensary 16 Dont Know 17 Other (specify) 18 Did anyone visit your Yes 1 house/neighborhood during last two No 2 years to make your DK/CS 3 family/community aware and provide information on TB? If yes, who visited? Government Doctor 1 (Multiple Response Possible) Private Doctor 2 AWW 3 ASHA 4 Any other Health worker 5 Worker from an NGO 6 Health Camp 7 DOTS workers 8 Others_____________________________9 Dont remember 10
Questions
Skip
Q57
57
58
If coded 2 & 3 skip to 61
59
96
Q. No 60
Questions Response Mostly on what specific aspects Symptoms of Tuberculosis 1 information is provided? Prevention from Tuberculosis 2 (Multiple answers) Cure for Tuberculosis 3 DOTS 4 Place of Treatment 5 Information on prevailing myths about TB patients 6 Others_______________________________7 Where from would you prefer to get TV 1 information on TB and related issues? Radio 2 Cinema (Multiple Response Possible) 3 Newspaper / Magazines 4 Hoarding/Posters/billboards/ Wall Painting 5 Public service announcements 6 Drama/Skits/Street plays/Melas 7 Hospital/Doctors 8 Friends & Relatives 9 Local Health workers 10 Inter Personal Communications 11 NGOs 12 None 13 Other (Specify 14 Which source of information, do you TV 1 trust most? Radio 2 Cinema 3 (Single code) Newspaper / Magazines 4 Hoarding/Posters/billboards/ Wall Painting 5 Public service announcements 6 Drama/Skits/Street plays/Melas 7 Hospital/Doctors 8 Friends & Relatives 9 Local Health workers 10 Inter Personal Communications 11 NGOs 12 None 13 Other (Specify 14 THANKS FOR YOUR VALUABLE TIME
Skip
61
62
97
People Infected with TB
Baseline KAP Survey on Tuberculosis Project-Oxygen ________________________ ____/_____/2011 Panjab Bihar 02 07 12 Haryana Mizoram Maharashtra 03 08 13 Rajasthan Karnataka Chhattisgarh 04 09 14 West Bengal Tamil Nadu Madhya Pradesh 05 10 15
QUESTIONNAIRE ID NUMBER DATE OF INTERVIEW STATE Uttar Pradesh Orissa Kerala 01 06
Andhra 11 Pradesh
DISTRICT NAME/ ID NUMBER__________________ DISTRICT SPECIFICATION TYPE OF SAMPLE BLOCK NAME_________________________ CODE VILLAGE /WARD NAME______________________CODE TYPE OF SETTLEMENT Name of the Nearest PHC Distance from the nearest PHC (kms) GENDER TYPE NAME OF THE RESPONDNET : 1. RURAL 2. URBAN 1. TRIBAL 2. NON-TRIBAL RANDOM-1 BOOSTER-2
1. MALE 2. FEMALE Complete treatment in last 12 months-1; Still continuing treatment--2
Date of Interview FIELD CONTROL INFORMATION Interview Yes 1 No 2 By Sign By 2 Sign By 2 Sign Code Code Starting Time of Interview Ending Time of Interview Code AM 1 PM 2 AM 1 PM 2
Spot / back check Yes 1 No Scrutiny Yes 1 No
If one or more than one visit made record: * Status of interview Date of first visit ______________ Time:_________ 1 2 3 4
98
Date of second visit Date of third visit * Refused 1
______________ ______________ not available 2
Time:_________ Time:_________ Partly Completed 3
1 1 Completed
2 2
3 3 4
4 4
Good morning/evening. I am from GFKMODE, a Social Research Organisation. We conduct surveys on various social issues from time to time. I shall be grateful if you could spare a few minutes and answer a few questions. The reason we want to speak with you is that International Union of Tuberculosis & Lung Disease (The Union) in collaboration with the Government of India TB Programme (RNTCP) is implementing a TB project that is aimed at improving Tuberculosis care and control for the communities. Through this study, we want to get some information on knowledge, attitude & behavior regarding tuberculosis among General Public, so that this information could help design appropriate strategies that will benefit the population. All of your responses will be treated as confidential and will be used only for research purposes and also to help policy makers to understand the bottlenecks in functioning, if any, to streamline the functioning. We shall be thankful for your cooperation. Informed Consent: Your participation in the interview and in every aspect of the study is completely voluntary. If some questions are difficult or make you uncomfortable, we can skip them. You may also ask me to clarify any questions if you do not understand them. You may also decide to stop the interview any time. I would like to assure you that the information provided by you would only be used for the purpose of research and your identity will not be revealed to anyone either in the final report or in any other way. If you have any questions or concerns after we completed the interview, you may ask.
RESPONDENT, KINDLY RESPOND TO HIS/HER SATISFACTION)
Do you have any questions about the survey? (INSTRUCTION TO INVESTIGATOR: IN CASE OF ANY QUESTIONS RAISED BY Would you be willing to participate in this survey? Yes=1 / No=2 Participant:
Name: - ____________________________________ Date: - _____________________________________ Signature or thumbprint: - _____________________
99
Q. No 1 2 3 4
9.a 10 A B C D E F
SOCIO ECONOMIC & DEMOGRAPHIC CHARACTERISTIC Questions Response What is your Name? ____________________ What is your sex? Male (Observe) Female How old are you? (Age in completed years) What is the last level of education that Illiterate you completed? Literate but no formal education Less than Primary Primary but less than Secondary Secondary but less than Senior Secondary Senior Secondary but not Graduate Graduation & above What is your occupation? Wage laborer Skilled worker Self employed Service (Govt. & Private) Business Agriculture/cultivator Unemployed House wife Student / Handicapped/ etc Any other (specify What is you average household income Less than Rs. 2000 per month? Rs. 2000 Rs. 4000 Rs. 4001 Rs. 8000 Rs. 8001 Rs. 10,000 Rs. 10,001 and above DK/CS What is your current marital status? Married Unmarried Divorced Widowed Separated What is your family type? Single Joint Extended Type of House Pucca house Semi-pucca house Kachha house Does your household own this house or Yes any other house? No Does your household have: Yes No Electricity 1 2 Mattress 1 2 Pressure cooker 1 2 Chair 1 2 A cot or Bed 1 2 A table 1 2
Skip
1 2
1 2 3 4 5 6 7 1 2 3 4 5 6 7 8 9 10 1 2 3 4 5 6 1 2 3 4 5 1 2 3 1 2 3 1 2
100
G H I J K L M N O P Q R S T U V W 11
12 13
14
Electric Fan 1 2 Radio Or Transistor 1 2 A black & white Television 1 2 A color Television 1 2 A sewing Machine 1 2 A mobile Telephone 1 2 Any other Type of Phone 1 2 A computer 1 2 A Refrigerator 1 2 A Watch or Clock 1 2 A Bicycle 1 2 A Motorcycle or Scooter 1 2 An Animal drawn cart 1 2 A Car 1 2 Water Pump (For agricultural Use) 1 2 A Thresher (For agricultural Use) 1 2 A Tractor(For agricultural Use) 1 2 What is the main source of drinking Private Tap 1 water for your house? Private Hand Pump 2 Public Tap 3 Public Hand Pump 4 Tube well 5 Supply tanker 6 Well/river/pond 7 Packaged Water 8 Rain water 9 Others (Specify_________________________)10 Is there a separate space for cooking? Yes 1 No 2 Type of fuel mostly used for cooking: Electricity 1 Wood 2 Coal/Lignite 3 Kerosene 4 LPG(Gas)/Natural Gas 5 Charcoal 6 Bio-gas 7 Dung Cakes 8 Agriculture Crop Waste 9 Straw/Shrubs/Grass 10 Others(Specify_________________________ _)88 Does your household have a BPL card? Yes 1 No 2
101
Q. No 15
16
17
18 19
20
21
HEALTH SEEKING BEHAVIOR Questions Response When someone falls sick in your family, Government Hospital (Including PHC,CHC 1 where do you generally go? Sub Center/ANM 2 3 Private Clinic /Private Hospital Ayurvedic treatment 4 Homeopathic treatment 5 Traditional healer/ Quacks 6 Clinic run by NGOs 7 Any other (Specify) 8 If not to a Government Health facility? Hospital is far from home 1 Why not? (Multiple answers) Unavailability of doctors 2 Unfriendly behavior 3 Long Waiting Hours 4 Lack of Diagnostic facility 5 Lack of Qualified Doctor 6 Lack of Diagnostic Equipments in the facility 7 Unhygienic 8 Private Clinic is nearby 9 Any Other (Specify) 10 TB DISEASE RELATED QUESTIONS FOR TB PATIENTS Can you tell us what causes TB? Germs/ Microorganisms 1 Others (Specify________________________)2 DK/CS 3 Was this the first time you were Yes 1 diagnosed with TB? No 2 If no, then how many times in the Once 1 past were your diagnosed with TB? Twice 2 Three times or more 3 Where did you take the treatment Government Hospital 1 previously? Private hospital/ clinic 2 Both government and private 3 Clinics run by NGOs 4 Did you complete the treatment each Yes 1 time? No 2 What symptoms did you have for the current episode? ( IN COMPLETED WEEK) (Multiple answers) Cough ( If mention, then for what duration weeks 1 Fever (If mention then for what duration weeks 2 Chest pain (If mention then for what duration weeks 3 Blood in sputum (If mention then for what duration weeks 4 Weight loss (If mention then for what duration weeks 5 Others ______________________________6 CS/DK 7 No 8
Skip If coded (1) skip to 17
If 1, go to Q.22
22
102
Q. No 23
Questions
Response
Skip
24
25
26
27
28
29
How long after the onset of these Less than a week 1 symptoms when did you visit a health 1 week 2 care provider/Facility? 2 weeks 3 3 weeks 4 4 weeks 5 4-6 weeks 6 6-8 weeks 7 8-12 weeks 8 >12 weeks 9 Not Visited 10 Do-not know 11 After how many days after the onset Days ____________________________ of symptoms did you come to know about you are/were suffering from TB? How many Health Care Providers/Doctors did you visit number(s)_________________________ before you diagnosed with TB? After getting these symptoms, whom Knowledgeable person in community 1 all did you consult or go to for Unqualified Healer in locality (quack) 2 treatment before going for diagnosis Faith healer 3 of TB? (multiple answers possible) Other Family Member 4 Spouse 5 Friends/ Relatives/Colleagues/Employer 6 Medicine retail outlet /Chemist 7 Qualified private doctor/clinic 8 Local Health Care Provider 9 Govt. dispensary /health center 10 Any other (specify) _________________________11 Who made a diagnosis that you are At Government Hospital/ Dispensary (Including suffering from TB? PHC,CHC) 1 Government health worker 2 TB hospital /TB diagnostic Centre / DOTS centre/Designated Microscopic Centre 3 Medical college 4 Private Clinic /Private Hospital/ Private Doctor 5 Ayurvedic Doctor/ Homeopathic doctor 6 7 Traditional healer Clinics/ hospitals run by NGOs 8 Any other Specify___________________________9 What organ of your body was said to Lungs 1 be affected by TB? Any other 2 Specify_________________________________ __3 Whether the sputum examination Yes 1 was done? No 2
103
Q. No 30 31 32
Questions Was chest X-Ray done? Was any blood tests done? Did you pay for the investigations?
Response Yes No Yes No Yes No DK/CS Not applicable Rs ___________ (approximately) 1 2 1 2 1 2 3 4 1
Skip
If coded 2,3 & 4 skip to Q. 34
33 34
If yes, then how much did you pay?
After diagnosis, how long did you No of take to start taking medicines? days_________________________________1 Have you heard of free diagnosis and treatment for tuberculosis Yes No 1 2 If coded 2 , then skip to Q.37
35
36
37
38
39
If yes, then from where is it Government health facility 1 available? Private health facility 2 Non-Governmental health facility 3 (Multiple answers) Others (specify) 4 Do not know 5 Not applicable 6 From where are/were you taking From the Government health centers, free of medicines? (DOTS) cost under DOTS 1 From the Government health centers, with payment for medicines 2 From non-government health centers, free of cost 3 From the non government health centers, with 4 payment for medicines DOTS Provider /Worker 5 ANM 6 ASHA 7 Do-not know 8 Not applicable 9 Are you still taking DOTS medicines? Yes 1 If coded 1, No 2 then skip to Q. 40 If no, Then why did you stop taking On the advice of the treating medical DOTS medicines? practitioner/ Completely Cured 1 Stopped by myself 2 Medicine is expensive and I stopped taking it 3 Side effect 4 5 Medicine not available Other__________________________________ __6 Not applicable 7
104
Q. No 40
Questions How many Days/ months of treatment did you take?( single code)
Response Days.1
Skip
41
Months2 Were you taking the medicines Yes regularly without missing any doses? No
1 2
42
43
How long have you been advised to Less than 2 weeks 1 take medicines? 2-4 weeks 2 1-3 months 3 4-5 months 4 6-8 Months 5 More than 8 months-Specify_____________6 Do-not know 7 Not applicable 8 Are you taking the medicines Yes 1 regularly without missing any doses No 2 Not applicable in the last 2 weeks? 3 According to you how do you rate the Completely regular 1 regularity of your drug intake? Somewhat irregular 2 Very irregular 3 Why was there any break or Could not go for medicines 1 irregularity in treatment? Interrupted due to side effects 2 Could not afford to buy medicines anymore 3 Discontinued as symptoms disappeared 4 Forget/ non seriousness 5 DOTS Provider was not available 6 Any other (specify) 7 Are you taking medicines under Under supervision (DOTS) 1 anyones supervision, or Independently 2 independently by yourself? If under supervision, who is/was the ANM from nearest sub-center 1 DOTS provider? Anganwadi Worker 2 ASHA worker 3 NGO volunteer in the community 4 Directly from the health facility 5 Community volunteer 6 Sarpanch /Panchayat Member 7 Neighbor /relatives /friends 8 Any other (specify)______________________9 Not applicable 10 Were you given a choice to select Yes 1 your provider? No 2 Not applicable 3 Are you satisfied with your provider? Yes No Can not say 1 2 3 If coded 1, then skip to 46
44
45
46
If coded 2 skip to Q. 48
47
48
49
105
Q. No 50(a) 50 (b)
Questions How much time does it take to reach for Diagnosis? How much time does it take to reach to your provider for routine check up/ Taking medicine How much does it cost to go to your provider? Is timing of the availability of the health service provider convenient to you? Are you paying for your medicines/ did you pay for your medicines?
Response Minutes____________________________ Minutes___________________________
Skip
51 52
Rs________________________________/Yes No Not applicable Yes No Do-not know Not applicable (in Rupees)_________________________ Yes No 1 2 1 2 3 1 2 3 4
53
54 55
How much does/did it cost per day? Does anybody visit your house and check whether you are taking medicines regularly as prescribed or not? Are there any children aged less than 6 years old in your house?
56
Yes No
1 2 1 2
If coded 2 skip to 58
57
If yes, are they receiving any Yes medicines for the prevention of T.B? No
IDENTIFICATION OF HEALTH INFORMATION RELATED OPINION LEADERS OR HEALTH PROVIDERS 58 For any health related information, Local Health care generally who does your family provider(ANM/RMP/ASHA/AWW) 1 contact? Neighbor/ Friend /relative 2 Doctor (Allopathic 3 (Multiple Response Possible) Community leader 4 Religious Leader 5 NGO Workers 6 Pharmacist 7 AYUSH Doctors 8 9 DOTS provider Others ______ specify 10 None 11 59 Name of the person who the family contacts for any health related Name: ________________________________1 information? DK/CS 2
106
Q. No 60
Questions
Response
Skip
61
For any health/medical care, mainly Government Hospital -Including PHC,CHC, who does your family contact? District Hospital 1 Sub Center/ANM 2 (Single Response Possible) Private Clinic /Private Hospital/ Private doctor (allopathic) 3 Private Ayurvedic treatment/ Ayurvedic practitioner 4 Private Homeopathic treatment/ Homeopathic practitioner 5 Traditional healer 6 Clinic run by NGOs /TRUST 7 8 Government Medical college Friends/ relatives/ niebougher 9 Any other (Specify)_____________________10 Have you informed your disease Yes 1 status to your household family No 2 members? Not applicable 3
If coded 2 skip to Q. 64 If coded 3 skip to 65
63 64
65
66
67
68
69
70
If yes then how do you rate their Supportive reaction? Not supportive If No, why did you not inform them? Fear Discrimination Others ( specify) Have you informed your disease Yes status to any of your friends? No Do-not want to answer this question Not applicable If Yes, Did you experience any Yes discriminatory difference in their No interaction with you after they knew Do-not want to answer this question that you have TB? Not applicable Did you experience that your friends Yes dont want to have a meal with you? No Do-not want to answer this question Not applicable Did your friends refuse to enter into Yes your house because of your disease No status? Do-not want to answer this question Not applicable Did friends refuse to shake hands Yes with you? No Do-not want to answer this question Not applicable If married, did you see any Yes discriminatory change in the No relationship with your partner? Do-not want to answer Not applicable
1 2 1 2 3 1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4
If coded 2,3 &4 Skip to 70 New Grid
107
Q. No 71
Questions
Response
Skip
72
73
74
75
Q. No 76
77
78
In your community, do you think that Yes 1 if a boy is known to have suffered No 2 from TB, will he get married? Do-not want to answer 3 Not applicable 4 In your community, do you think that Yes 1 if a girl is known to have suffered No 2 from TB, will she get married? Do-not know 3 In your community, who do you think Males 1 suffer more (socially) when they are Females 2 affected by TB? Males or females Both are equally affected 3 Do-not know 4 Not applicable/ No one suffers 5 Have you disclosed your disease Yes 1 If coded 2 2/3/4 Skip status at the place of your No Do-not want to answer 3 to 76 employment? Not applicable 4 Did you have to change your Yes 1 employment because of your disease No 2 status? Do-not want to answer 3 Not applicable 4 MEDIA HABIT & PREFERENCES Questions Response Skip Which source of information you are Radio 1 Q77 exposed to? (Multiple Response TV 2 Q 79 Newspaper & Magazines 3 Possible- Probe) Cinema 4 Hoardings/posters/leaflets/Wall painting 5 Melas/ Nukkad Nataks etc 6 Internet/Web advertising 7 Q81 Word of mouth (Interpersonal communication) 8 Mobile phone advertising 9 Any Other ____________________________10 None 11 IF RESPONDED 1 IN Q. 76, Which Vividh Bharti 1 2 station of Radio do you generally FM (specify) Regional Channel 3 listen to? Community Radio 4 Other (specify) 5 Which program do you like most on News 1 Radio? Drama / Serial 2 Film Songs 3 Folk Songs 4 Health related Discussion 5 Other (specify) 6
108
Q. No 79
Questions Response IF CODED 2 IN Q. 76 Which Television Channel 1.most watched ---------------channel do you generally watch? nd (Multiple Response Possible) Channel 2 most. --------------------------Channel 3 most. ---------------------------Channel 4th most ---------------------------Which programs do you like the most News on TV? (Probe for two most liked Drama/Serial programs) Entertainment / reality show Health Related Programs Advertisements Folk music Music- Other than folk Movie Other (Specify) Do you read newspaper? Yes No DK/CS Which language paper generally you English read? Hindi Any other Local language
rd
Skip
80
81
82
1 2 3 4 5 6 7 8 9 1 2 3 1 2 3
If coded 2 & 3 skip to Q. 84
83 (a)
83(b)
84
85
Names of the newspapers you usually News Paper 1 read? News Paper 2 News Paper 3 Have you ever seen an Yes 1 advertisement/ information on No 2 DK/CS 3 Tuberculosis or DOTS? If Yes, Where did you see such Newspaper & Magazines 1 advertisement or/and information on Radio 2 TB/DOTS? (Multiple Response TV 3 Possible) Hoardings/posters/leaflets 4 Melas/ Nukkad Nataks etc 5 Any Other (specify) 6 What is your most common source of Radio 1 getting health-related message/ TV 2 Information? Newspaper & Magazines 3 Cinema 4 Hoardings/posters/leaflets/Wall painting 5 Melas/ Nukkad Nataks etc 6 Internet/Web advertising 7 Word of mouth (Interpersonal communication) 8 Local Health Service providers 9 Mobile phone advertising 10 Any Other 11 None 12
83 (b)
Q 85
109
Q. No 86
Questions Where have you received message/information on (Multiple answers)
Response 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 1 2
Skip
87 88 89
any TV TB? Radio Cinema Newspaper / Magazines Hoarding/Posters/billboards/ Wall writing /Brochure/other printed material Internet Public service announcements Drama/Skits/Street plays Hospital/doctor Friends & Relatives Teachers/peer educator /colleagues Health camp Health workers DOTS providers Local leaders/ religious leader Sarpanch/ Panchayat Member None of these Other (specify) Can you recall any message on TB? Yes No If yes, then specify. The message (Record verbatim)
Q89
What are your sources of information Friends for awareness on Tuberculosis Family related issues in last one month? Neighbors (Multiple Response Possible) Colleague Teachers Newspaper/Magazines/Leaflets/ Wall paint /Bill-boards
1 2 3 4 5
Posters/Brochures/Other printed materials 7 Radio TV Cinema Local Health Workers/Doctors Internet/Web advertising Interpersonal Communication 8 9 10 11 12 13
Others (specify)______________________14 Dont Know 15
110
Q. No 90
91
Questions Did anyone visit your house/neighborhood during last one year to make your family/community aware and provide information on TB? If yes, who visited? (Multiple Response Possible)
Response Yes No DK/CS
1 2 3
Skip If coded 2 & 3 skip to 93
91
92
93
Government Doctor 1 Private Doctor 2 AWW 3 ASHA 4 Health worker 5 Worker from an NGO 6 Others (specify) 7 Dont remember 8 Mostly on what specific aspects Symptoms of Tuberculosis 1 information is provided? Prevention from Tuberculosis 2 (Multiple answers) Cure for Tuberculosis 3 DOTS 4 5 Place of Treatment Information on prevailing myths/stigma about TB patients 6 7 Others (specify) Where from would you prefer to get TV 1 information on TB and related issues? Radio 2 (Multiple Response Possible) Cinema 3 4 Newspaper / Magazines Hoarding/Posters/billboards/ Wall writing 5 Internet/ Web Advertising 6 Public service announcements 7 Drama/Skits/Street plays 8 Hospital/doctor 9 10 Friends & Relatives Teachers/peer educator 11 Health camp 12 Health & related workers 13 14 DOTS Centre DOTS providers 15 Religious Leader 16 Local Dispensary 17 Dont Know 18 Other (specify) 19 Which source of information, do you Popular leaders/Religious leaders 1 trust more? Government Health Staff 2 Private Health staff 3 Print Media 4 Electronic Media 5 Folk Media 6 Sarpanch / Panchayat Member 7 Friend /relatives 8 Others (specify) 9 None 10
THANKS FOR YOUR VALUABLE TIME
111
HEALTH SERVICE PROVIDERS
Baseline KAP Survey on Tuberculosis QUESIONNAIRE ID NUMBER DATE OF INTERVIEW ____________________________ ____/_____/2011 1. U.P STATE 2. Punjab 3. Haryana 4. Rajasthan 5. Maharashtra 10. Andhra 14. Mizoram
6. Chattisgarh 7. West Bengal 8. Orissa 9. Bihar Pradesh 11. Karnataka 12. Tamil Nadu 13. Kerala 15. Madhya Pradesh
DISTRICT PSU
Name of the Doctor & Address
RESPONDENT CATEGORY
1. Private Practitioner 2. Government Doctor
Date of Interview FIELD CONTROL INFORMATION Starting Time of Interview Ending Time of Interview Interview Yes 1 No 2 By Sign By 2 Sign By 2 Sign Code Code Code AM 1 PM 2
Spot / back check Yes 1 No
Scrutiny Yes 1 No
Good morning/evening. I am from GFKMODE, a Social research organisation. We conduct surveys on various social issues from time to time. I shall be grateful if you could spare a few minutes and answer a few questions.
The reason we want to speak with you is that International Union of Tuberculosis & Lung Disease (The Union) in collaboration with the Government of India TB Programme (RNTCP) is implementing a TB project that is aimed at improving Tuberculosis care and control for the communities. Through this study, we want to get some information on knowledge, attitude & behavior regarding tuberculosis among Health Service Provider, so that this information could help design appropriate strategies that will benefit the population.
112
All of your responses will be treated as confidential and will be used only for research purposes and also to help policy makers to understand the bottlenecks in functioning, if any, to streamline the functioning. We shall be thankful for your cooperation.
Q. No 1 2 3
GENERAL INFORMATION Questions Response What is your Name? What is your Sex? Male (Observation) Female How old are you? (Age in completed years) Address Educational Qualification MBBS BAMS BHMS BUMS Others ____________________
Skip 1 2
4 5
1 2 3 4 5 1 2 3 1 2 1 2 3 If coded 1, Go to Q.10 IF coded 2 & 3, then Terminate
6 7
Experience in years Nature of Practice
8 9
Dispensing GP Prescribing GP Consultant/Specialist KNOWLEDGE, ATTITUDE & BEHAVIOR ON TUBERCULOSIS What are the common diseases you TB Mentioned come across in your practice? TB Not mentioned If TB is not mentioned, Do you come Yes across TB patients in your clinic? No No Response If yes, on an average how many TB patients you come across in a month? How many of them are female TB patients
10 11 12
No of patient(s)
No. of female TB patient(s 1 2 3 4 5 6 7 1 2 3 4 5 1 2 1 2 3 4
13
14 15
What are the different kinds of TB Pulmonary TB (Chest/Lungs) patients that you come across ? Lymph Glands TB Spinal TB Bone TB Abdominal TB Any Other What are the common sy m p to m s A cough of 2 weeks y o u look for while diagnosing the Pain in the chest person with TB? Coughing up Blood (Multiple Response Possible) Fever Any other specify Are you aware of MDR TB? Yes No How do you diagnose a patient as MDR- Based on sputum culture/sensitivity TB? Clinical Examination DST Testing Any other- specify
IF coded 2 skip to Q. 17
113
Q. No 16
Questions What investigations do you advice for confirming diagnosis of Pulmonary TB? (Multiple Response Possible)
17
If you have to advice only one test, which one would you advice for TB patient?
18
What is the reason for selecting the test mentioned above? How frequently do you advice for sputum smear test in pulmonary TB suspect?
19
20
Where do you send your patient for sputum examination?
21
22
23
24
Do you face any problem in getting sputum smear examination done for your TB suspects in a DMC (Designated Microscopic centre)? If yes, what type of problems do you face? Non availability of facility 1 Non availability of staff 2 3 Patient is unable to incurred other costs Poor quality result 4 Any other (specify 5 What do you do after diagnosing Advice to go to the Government Hospital/ T.B pulmonary TB? Hospital 1 Treat on my own 2 Refer to private facility 3 Refer to DOTS provider/Center 4 Refer to NGO 5 Any other 6 What system of medicine do you usually Allopathic 1 follow for treatment for pulmonary TB? Homeopathy 2 Ayurvedic 3 Traditional 4 Other 5
Response Chest X ray 1 Sputum smear examination 2 Mantoux skin Test 3 Culture 4 Any other- specify 5 Chest X ray 1 Sputum smear examination 2 Mantoux skin Test 3 Culture 4 Any Other 5 Reliable 1 Service Available 2 Any other- specify 3 Everyday 1 Once a Week 2 Twice a Week 3 4 Once a Month Twice/Thrice a Month 5 6 As /When Required Never 7 Govt. Hospital with Designated Microscopy 1 Centre (DMC) Private Hospital with Designated Microscopy Centre 2 Private Hospital with out Designated Microscopy Centre 3 Any other 4 Yes 1 No 2
Skip
If coded 2 skip to Q.23
114
Q. No 25
26
27
28
28a
29
30 31
32
33
34
Questions Response What is the average duration of 1-2 weeks 1 treatment? 2-4 weeks 2 1-5 months 3 6-8 months 4 More than 8 months 5 How do you know that Pulmonary TB Improvement in symptoms 1 patient is cured? Positive sputum turned negative 2 Improvement in X Rays 3 Prescribed duration of treatment completed4 5 All the above Do you maintain any separate record Yes 1 (like detailed address, next visit due No 2 etc.) for TB patients at your clinic? In the one year, how many TB patients did you treat? Total Number of patients ________________ How many of them (TB patients) Number of patients completed treatment completed their prescribed duration of ____________________________________ treatment in the last 1 year? What difficulties do you come across People hesitate to come for treatment 1 while treating TB patients? Non availability of anti TB drugs 2 (Multiple Response Possible) No pathology or X ray Lab available in the vicinity 3 People do not reveal previous history of TB easily 4 Any other(specify)_______________________5 None 6 Do you examine other members of Yes 1 No 2 patient family for TB? Do you think treating TB constitutes any Yes 1 risk to your health or health of your No 2 3 other patients? DK/CS What precautions do you take to Maintain distance 1 protect yourself while Wear masks & gloves 2 Wash hands with soap 3 examining/treating TB patients? (Multiple Response Possible) None 4 Any Other (Specify) 5 What precautions do you suggest the Cover your face while coughing 1 TB patient to avoid the spread of Use separate utensils 2 disease? Not to spit anywhere 3 (Multiple Response Possible) Use separate towels/clothes 4 Isolate the patient 5 6 Any other Have you heard of DOTS? Yes 1 No 2 DK/CS 3
Skip
If coded 2 & 3 Skip to Q.39
115
Q. No 35
36
37
38 39
Questions Response Which are two major sources from Television where you came to know about DOTS Radio and related issues? Newspaper / Magazines Pamphlets/Booklets/leaflets/posters etc Awareness workshop, seminar During studies/part of course Internet Medical Journals NGO Any other (specify For treating TB: Do you feel; DOTS is Excellent ( Read out the option) Good Average Bad CS/DK Are you aware of the schemes to Yes involve private practitioners in the No DOTS programme? Are you involved in DOTS programme? Yes (Ask only to Govt. Doctors) No Are there any public health services for TB patients available in your area? (Ask only private practitioners) Do patients of other diseases avoid visiting you because you also treat persons suffering with TB? Yes No DK/CS Yes No DK/CS
Skip 1 2 3 4 5 6 7 8 9 10 1 2 3 4 5 1 2 1 2 1 2 3 1 2 3
40
41
42
43
44
From where do you commonly update Medical journals 1 your knowledge on TB? Colleague 2 (Multiple Response Possible) CME/trainings / Conferences 3 Professional bodies 4 Medical representatives 5 No need 6 Any other 7 According to you what should be the Television 1 best medium to generate awareness Radio 2 amongst the community about Newspaper/Magazine 3 TB?(Single code) Pamphlet/Booklet/ Leaflet/Posters 4 Nukkad Nataks 5 Community meetings 6 IPC (Interpersonal Communication) 7 Any Other 8 Where did your patients get the anti TB Government 1 drugs? NGO 2 Local Chemist 3 Provide on your own 4 Do you have any suggestions to strengthen TB control services? ___________________________________ ___________________________________ _____________________________-___ THANKS FOR YOUR VALUABLE TIME
102
State:
_____________
E (KAP SURVEY ON TUBERCULOSIS)-Project-Oxygen District: ___________ Village/WARD Name_____________ Date of Listing________________ Whether any family Name and age of member suffered from the following diseases in the member who last one year? suffered from tuberculosis? If yes, whether taken treatment for tuberculosis from any health facility? What is the status of treatment for tuberculosis? Mark the Selected Households Interview Status DONE=1 NOT COMPLETED= 2
PSU NO: _____________ Name of the Lister______________________ Detail of the HH
Malaria
Jaundice
Leprosy
Tuberculosis
SL.N o
Name of the head of the household
Address / Name of the Mahlla / Tola / Hamlets / landmark
Number of usual resident in household
Name
Age(yrs)
Completed
continuing
MARK ONE FOR GP AND MARK TWO FOR TB PATIENT
103
NGO/CBO
Baseline KAP Survey on Tuberculosis ____________________________ ____/_____/2011
QUESIONNAIRE ID NUMBER DATE OF INTERVIEW STATE Uttar Pradesh Orissa 01 06 Panjab
02 07 12
Haryana Mizoram Maharashtra
03 08 13
Rajasthan Karnataka Chhattisgarh
04 09 14
West Bengal Tamil Nadu Madhya Pradesh
05 10 15
Bihar Andhra Kerala 11 Pradesh DISTRICT NAME & CODE
Date of Interview FIELD CONTROL INFORMATION Interview Yes 1 No 2 By Sign By 2 Sign By 2 Sign Code Code Starting Time of Interview Ending Time of Interview Code AM 1 PM 2 AM 1 PM 2
Spot / back check Yes 1 No
Scrutiny Yes 1 No
If one or more than one visit made record: * Status of interview 1 2 3 4 1 1 Completed 2 2 4 3 3 4 4
Date of first visit Date of second visit Date of third visit * Refused 1 not available
______________ ______________ ______________ 2
Time:_________ Time:_________ Time:_________
Partly Completed 3
Good morning/evening. I am from GFKMODE, a Social research organisation. We conduct surveys on various social issues from time to time. I shall be grateful if you could spare a few minutes and answer a few questions. The reason we want to speak with you is that International Union of Tuberculosis & Lung Disease (The Union) in collaboration with the Government of India TB Programme (RNTCP) is implementing a TB project that is aimed at improving Tuberculosis care and control for the communities. Through this study, we want to get some information on knowledge, attitude & behavior regarding tuberculosis among Opinion Leaders, so that this information could help design appropriate strategies that will benefit the population. All of your responses will be treated as confidential and will be used only for research purposes and also to help policy makers to understand the bottlenecks in functioning, if any, to streamline the functioning. We shall be thankful for your cooperation.
104
Q. No 1 2 3 4. 5. 6.
7. 8.
9. 10
11
12
GENERAL INFORMATION Questions Response Skip What is your Name? What is your sex? Male 1 (Observe) Female 2 How old are you? (Age in completed years) Address KNOWLEDGE AND AWARENESS ABOUT TUBERCULOSIS AND TREATMENT What are the common diseases in TB Mentioned 1 If coded 1 skip your community? TB Not mentioned 2 to Q.7 If TB is not mentioned, have you Yes 1 If coded 2 & 3 heard of TB? No 2 then DK/CS 3 terminate If yes, do you know the common Yes 1 symptoms of TB? No 2 Q9 If yes, could you mention few symptoms A cough of 2 weeks 1 of TB? Pain in the chest 2 (Multiple Response Possible) Coughing up blood 3 Fever 4 Night sweat 5 Weight loss 6 Loss of appetite 7 Any other (Specify) 8 Dont know 9 Do you think TB is a serious disease in Yes 1 India? No 2 Do you know how can a person get Through handshake with infected person infected with TB? 1 (Multiple Response Possible) Through the air when the infected person 2 cough or sneeze Through sharing food with infected person 3 By sharing bed/clothes with infected 4 person Dont Know 5 Any other (Specify) 6 Who do you think are more prone to get Those living in unhygienic condition 1 infected with TB? Poor People 2 (Multiple Response Possible) Malnourished 3 Children 4 Women 5 Family members of TB infected person 6 Exposed to cough and cold for long time 7 HIV +ve 8 Smokers 9 Alcoholics 10 Any other ( specify) 11 DK/CS 12 According to you whether TB Yes, Fully 1 affected person can be treated? Yes , Partially 2 No 3 DK/CS 4
105
Q. No 13
Questions How can a person infected with TB be cured? (Multiple Response Possible)
14
How long does it take to cure TB?
16
How can TB be diagnosed? (Multiple Response Possible)
17
Are you aware of the place where you can get Tuberculosis diagnosed? (Multiple Response Possible)
18
Are you aware of the place where you can get medicine for Tuberculosis? (Multiple Response Possible)
19
20
Are you aware that a specific treatment is available to treat Tuberculosis? Have you heard of DOTS? Yes No If yes, what for this is used?
Response Herbal Remedies DOTS Other Allopathic medicines Ayurvedic Homeopathy Any other (specify) DK/CS Less than 2 weeks 2-4 weeks 1-5 months 6 -8 months More then 8 months and others DK/CS Sputum smear Test X Ray Mantoux Skin Test Any Other (Specify) DK/CS Government Hospital CHC/PHCs Private Hospital/Clinic NGO DOTS Centre Any Other(Specify) DK/CS Government Hospital CHC/PHCs ANM/ASHA/AWW Private Hospital/Clinic DOTS Provider/ Centre NGO Any Other (Specify) DK/CS Yes No
Skip 1 2 3 4 5 6 7 1 2 3 4 5 6 1 2 3 4 5 1 2 3 4 5 6 7 1 2 3 4 5 6 7 8 1 2 1 2 1 2 3 1 2 3 4 5 6 7 8 If coded 2, then skip to 23
21
22
For treating Tuberculosis For treating other ailments DK/CS Are you aware of the place where Government Hospital you can get DOTS? CHC/PHCs ANM/ASHA/AWW Private Hospital/Clinic DOTS Provider/ Centre NGO Any Other (Specify) DK/CS
106
Q. No 23
24
Questions If DOTS/TB centre is not mentioned, have you heard of DOTS centre/provider? Do you know that Government is providing DOTS free of cost?
Response Yes No DK/CS Yes No DK/CS HEALTH SEEKING BEHAVIOR
Skip 1 2 3 1 2 3 If coded (1 &2) skip to 27
25
26
27
28
When someone falls sick, where will Government Hospital (Including PHC,CHC) you generally refer him /her to go? 1 Sub Center/ANM 2 Private Clinic /Private Hospital 3 Ayurvedic treatment 4 Homeopathic treatment 5 Traditional healer/ Quacks 6 Clinic run by NGOs 7 Any other (Specify 8 If not to a Government Health Hospital is far from home 1 centre? Why? Unavailability of doctors 2 Unfriendly behavior 3 Long Waiting Hours 4 Lack of Diagnostic facility 5 Lack of Qualified Doctor 6 Lack of Diagnostic Equipments in the 7 facility Private Clinic is nearby 8 Unhygienic Condition 9 Any Other (Specify)_____________________10 If a person is suspected with TB, Government Centres /DMC 1 where according to you, he should go Private Hospitals 2 DOTS/TB Centres 3 for diagnosis? Any Other 4 If a person is diagnosed with TB, Government Centres 1 where according to you, he should go Private Hospitals 2 for treatment? DOTS/TB Centres 3 Any Other 4 STIGMA & DISCRIMINATION Now I will make some statements about People suffering from TB. Please let me know how much you agree to these? A family with TB patient should not be allowed to participate in any social function Married female TB patient should be sent off to her parents house Children with TB should not be allowed to go to school Daily ware Laborers suffering from TB should not be allowed to work Strongly Agree 1 Somewhat agree 2 Disagree 3
29
Dont Know/ Cant Say 4
b c d
107
g 30 a b
c d e f
31
32
33
34
35
Husbands/in-laws do not accompany female TB patients to hospital /DOTS centers Female accompany their spouse to hospitals suffering from TB to hospitals /DOTS centre Females suffering from TB face problem in marriage Which of the following you would Yes No DK/CS agree to do? 1 2 3 Share a meal with person you know had TB If you suspect one of the female member is suffering from TB, do you take her to hospital Marry your daughter to a boy knowing had a TB Isolate your family member having TB from the household Marry your son to a girl who you know had TB Send your daughter in law to parents house if she had TB in order to protect other family members from TB In your community, how is the Most people reject him or her 1 person suffering from TB usually Most people are friendly but they generally treated? try to avoid him/her 2 Community mostly support and help him/her 3 Others (specify) 4 Do you know anyone in your family Yes 1 and neighborhood suffering from TB No 2 in the last 2 year DK/CS 3 If yes, have you given any advice to Go to Government Hospital 1 them? Go Private hospital 2 Isolate the family from the community 3 Any other- (specify) 4 None 5 Have you taken any initiative towards Yes 1 generating awareness about TB & No 2 DOTS within your community? If yes, what are they? Organized camps 1 Organized rallies 2 Organized lectures /Seminars/ Workshops 3 Worked as DOT provider 4 Nukkad Nataks/ Street Plays/Skits 5 Any other (Specify) 6
If coded 2 & 3 skip to 34
If coded 2 skip to 36
108
36
37
38
39
MEDIA HABIT & PREFERENCES Which source of information you are Newspaper & Magazines exposed to? Radio (Multiple Response Possible- Probe) TV Hoardings/posters/leaflets/Wall printing/ Bill Boards Internet Melas/ Nukkad Nataks etc Any other (Specify) If responded code 2 in Q.36 Which Vividh Bharti Station do you generally listen to? FM (Specify) Regional Channel Community Radio Any other (specify) Which program do you like most on News Radio? Drama / Serial (Multiple answers) Film songs Folk songs Health discussion Any other (specify) If responded codes 3 in Q.36 Which Television channel do you generally Channel watchs mostly watch? Channel (Multiple Response Possible) Channel Channel Which programs do you like the most News on TV? Drama/Serial (Probe for two most liked programs) Entertainment Health Related Programs Advertisements Folk music Music Films Any other (Specify) Do you read newspaper? Yes No Which language paper generally is English read by you? Hindi Local language Names of the newspapers you usually News Paper read? News Paper News Paper Have you ever seen an Yes advertisement/ information on No Tuberculosis or DOTS? DK/CS
1 2 3 4 5 6 7 1 2 3 4 5 1 2 3 4 5 6 1 2 3 4 1 2 3 4 5 6 7 8 9 1 2 1 2 3 1 2 3 1 2 3
40
41
If coded 2, then skip to Q.43
42(a)
42(b)
43
If coded 2 & 3, then skip to Q.45
109
Q. No 44
Questions
Response 1 2 3 4 5 6
Skip
If Yes, where did you see such Newspaper & Magazines advertisement or/and information on Radio TB/DOTS? TV (Multiple Response Possible) Hoardings/posters/leaflets Melas/ Nukkad Nataks etc Any other
45
INFORMATION SOURCES TV 1 What are your sources of information Radio 2 for awareness on Tuberculosis 3 Cinema related issues? Newspaper / Magazines 4 (Multiple Response Possible) Hoarding/Posters/billboards/ Wall writing 5 Public service announcements 6 Drama/Skits/Street plays 7 Hospital/doctor 8 Friends & Relatives 9 Health & related workers 10 DOTS providers 11 Internet 12 None of these 13 Any other (specify) 14 Yes 1 No 2 DK/CS 3 Government Doctor 1 Private Doctor 2 AWW 3 ASHA 4 Health worker 5 Worker from an NGO 6 Any others 7 Dont remember 8 Mostly on what specific aspects Symptoms of Tuberculosis 1 information is provided? Prevention from Tuberculosis 2 (Multiple Response Possible) Cure for Tuberculosis 3 DOTS 4 Place of Treatment 5 Information on prevailing myths about TB patients 6 7 Any other (Specify) Did anyone visit to make community aware and provide information on TB during last two years? If yes, who visited? (Multiple Response Possible) If coded 2 & 3 skip to 49
46
47
48
110
Q. No 49
Questions
Response 1 2 3 4 5 6 7 8 9 10 11 12
Skip
50
Where from would you prefer to get TV information on TB and related issues? Radio (Multiple Response Possible) Cinema Newspaper / Magazines Hoarding/Posters/billboards/ Wall writing Public service announcements Drama/Skits/Street plays/Melas Hospital Friends & Relatives Health workers NGOs Any other (Specify) According to you what are the two most important issues regarding --------------------------------------------1 tuberculosis which need utmost attention? ---------------------------------------------2 Do you have any suggestions how you /your organization could be more helpful in addressing Tuberculosis related issues?
51
ONLY FOR NGO/CBO 52 53 53a 54 Name of NGO you are working for? For how long this NGO is working? For how long you are working with this NGO? What are the issues taken up by your NGO? (Multiple Response Possible) No. of years: No. of Year(s)
55
TB specific/ DOTS program 1 Rural Development 2 Sanitation 3 Education 4 Other Health & Disease Related issues 5 Income generation 6 Gender issue 7 Domestic violence 8 Any other (specify) 9 If Yes, (code 1 in Q 54) what are Spreading awareness about TB, educating different types of activities being communities on its prevention & treatment addressed by your NGO (Those who 1 are working in the field of TB)? Provide community based care to TB (Multiple Response Possible) patients 2 Training to TB care health workers & volunteer 3 Help in reducing stigma & discrimination from the community on TB 4 Help resettlement of TB patients 5 Motivating TB patients to treat under DOTS programme 6 Spreading awareness about DOTS 7 As a DOTS provider 8 Other (specify) 9
Q56
Skip to Q57
111
Q. No
56
57
58
Questions If not addressing TB related issues, are you interested to work in the TB control area? Are you aware of any schemes under which NGOs can collaborate with RNTCP? If yes, are you also involved in any of the schemes?
Response Yes No DK/CS Yes No Dont Know/Cant say Yes No DK/CS
Skip 1 2 3 1 2 3 1 2 3
If coded 2 & 3 skip to 61
If coded 2 & 3 , Skip to Q. 61
59
If yes, what kind of schemes?
ACSM (Advocacy, Communication & Social Mobilization) 1 SC Scheme (Sputum Collection Center) 2 DMC (Designated Microscopy Centers) 3 LT Scheme 4 CS Scheme 5 Adherence Scheme 6
END
60
If involved in ACSM Scheme, specify the activities. ( Record Verbatim)
61
62
Do you want to collaborate with RNTCP to work in the field of Tuberculosis? If no, what are the reasons? (Multiple Response Possible)
Yes No
1 2
Insufficient grant under the schemes 1 People are not suffering from TB in this area 2 Do not have interest in working for People suffering from TB 3 Other (Specify 4
If coded 1, Close the interview END
THANKS FOR YOUR VALUABLE TIME
112
Opinion Leader
Baseline KAP Survey on Tuberculosis ____________________________ ____/_____/2011
QUESIONNAIRE ID NUMBER DATE OF INTERVIEW STATE Uttar Pradesh Orissa 01 06 Panjab
02 07 12
Haryana Mizoram Maharashtra
03 08 13
Rajasthan Karnataka Chhattisgarh
04 09 14
West Bengal Tamil Nadu
05 10
Bihar Andhra Kerala 11 Pradesh DISTRICT NAME & CODE Respondent Category
Madhya Pradesh 15
1. Village Pradhan 2. Panchayat Member 3. Ward Member 4. Religious Leader 5. ANM 6. AWW 7. Teacher Date of Interview
FIELD CONTROL INFORMATION Interview Yes 1 No 2 By Sign By 2 Sign By 2 Sign
Starting Time of Interview Ending Time of Interview Code
AM 1 PM 2 AM 1 PM 2
Spot / back check Yes 1 No
Code
Scrutiny Yes 1 No
Code
If one or more than one visit made record: * Status of interview 1 2 3 4 1 1 Completed 2 2 4 3 3 4 4
Date of first visit Date of second visit Date of third visit * Refused 1 not available
______________ ______________ ______________ 2
Time:_________ Time:_________ Time:_________
Partly Completed 3
Good morning/evening. I am from GFKMODE, a Social research organisation. We conduct surveys on various social issues from time to time. I shall be grateful if you could spare a few minutes and answer a few questions. The reason we want to speak with you is that International Union of Tuberculosis & Lung Disease (The Union) in collaboration with the Government of India TB Programme (RNTCP) is implementing a TB project that is aimed at improving Tuberculosis care and control for the communities. Through this study, we want to get some information on knowledge, attitude & behavior regarding tuberculosis among Opinion Leaders, so that this information could help design appropriate strategies that will benefit the population. All of your responses will be treated as confidential and will be used only for research purposes and also to help policy makers to understand the bottlenecks in functioning, if any, to streamline the functioning. We shall be thankful for your cooperation.
113
Q. No 1 2 3 4. 5. 6.
7. 8.
9. 10
GENERAL INFORMATION Questions Response What is your Name? What is your sex? Male 1 (Observe) Female 2 How old are you? (Age in completed years) Address KNOWLEDGE AND AWARENESS ABOUT TUBERCULOSIS AND TREATMENT What are the common diseases in TB Mentioned 1 your community? TB Not mentioned 2 If TB is not mentioned, have you Yes 1 heard of TB? No 2 DK/CS 3 If yes, do you know the common Yes 1 symptoms of TB? No 2 If yes, could you mention few symptoms A cough of 2 weeks 1 of TB? Pain in the chest 2 (Multiple Response Possible) Coughing up blood 3 Fever 4 Night sweat 5 Weight loss 6 Loss of appetite 7 Any other (Specify) 8 Dont know 9 Do you think TB is a serious disease in Yes 1 India? No 2 Do you know how can a person get Through handshake with infected infected with TB? person 1 (Multiple Response Possible) Through the air when the infected person 2 cough or sneeze Through sharing food with infected person 3 By sharing bed/clothes with infected 4 person Dont Know 5 Any other (Specify) 6 Who do you think are more prone to get Those living in unhygienic condition 1 infected with TB? Poor People 2 (Multiple Response Possible) Malnourished 3 Children 4 Women 5 Family members of TB infected person 6 Exposed to cough and cold for long time 7 8 HIV +ve Smokers 9 Alcoholics 10 Any other ( specify) 11 DK/CS 12 According to you whether TB Yes, Fully 1 affected person can be treated? Yes , Partially 2 No 3 DK/CS 4
Skip
If coded 1 skip to Q.7 If coded 2 & 3 then terminate Q9
11
12
114
Q. No 13
Questions How can a person infected with TB be cured? (Multiple Response Possible)
14
How long does it take to cure TB?
16
How can TB be diagnosed? (Multiple Response Possible)
17
Are you aware of the place where you can get Tuberculosis diagnosed? (Multiple Response Possible)
18
Are you aware of the place where you can get medicine for Tuberculosis? (Multiple Response Possible)
19
20
Are you aware that a specific treatment is available to treat Tuberculosis? Have you heard of DOTS? Yes No If yes, what for this is used?
Response Herbal Remedies DOTS Other Allopathic medicines Ayurvedic Homeopathy Any other (specify) DK/CS Less than 2 weeks 2-4 weeks 1-5 months 6 -8 months More then 8 months and others DK/CS Sputum smear Test X Ray Mantoux Skin Test Any Other (Specify) DK/CS Government Hospital CHC/PHCs Private Hospital/Clinic NGO DOTS Centre Any Other(Specify) DK/CS Government Hospital CHC/PHCs ANM/ASHA/AWW Private Hospital/Clinic DOTS Provider/ Centre NGO Any Other (Specify) DK/CS Yes No
Skip 1 2 3 4 5 6 7 1 2 3 4 5 6 1 2 3 4 5 1 2 3 4 5 6 7 1 2 3 4 5 6 7 8 1 2 1 2 1 2 3 1 2 3 4 5 6 7 8 If coded 2, then skip to 23
21
22
For treating Tuberculosis For treating other ailments DK/CS Are you aware of the place where Government Hospital you can get DOTS? CHC/PHCs ANM/ASHA/AWW Private Hospital/Clinic DOTS Provider/ Centre NGO Any Other (Specify) DK/CS
115
Q. No 23
24
Questions If DOTS/TB centre is not mentioned, have you heard of DOTS centre/provider? Do you know that Government is providing DOTS free of cost?
Response Yes No DK/CS Yes No DK/CS HEALTH SEEKING BEHAVIOR
Skip 1 2 3 1 2 3 If coded (1 &2) skip to 27
25
26
27
28
When someone falls sick, where will Government Hospital (Including PHC,CHC) you generally refer him /her to go? 1 Sub Center/ANM 2 Private Clinic /Private Hospital 3 Ayurvedic treatment 4 Homeopathic treatment 5 Traditional healer/ Quacks 6 Clinic run by NGOs 7 Any other (Specify) 8 If not to a Government Health Hospital is far from home 1 centre? Why? Unavailability of doctors 2 Unfriendly behavior 3 Long Waiting Hours 4 Lack of Diagnostic facility 5 Lack of Qualified Doctor 6 Lack of Diagnostic Equipments in the facility 7 Private Clinic is nearby 8 Unhygienic Condition 9 Any Other (Specify)_____________________10 If a person is suspected with TB, Government Centres /DMC 1 where according to you, he should go Private Hospitals 2 DOTS/TB Centres 3 for diagnosis? Any Other 4 If a person is diagnosed with TB, Government Centres 1 where according to you, he should go Private Hospitals 2 for treatment? DOTS/TB Centres 3 Any Other 4 STIGMA & DISCRIMINATION Now I will make some statements about People suffering from TB. Please let me know how much you agree to these? A family with TB patient should not be allowed to participate in any social function Married female TB patient should be sent off to her parents house Children with TB should not be allowed to go to school Daily ware Laborers suffering from TB should not be allowed to work Strongly Agree 1 Somewhat agree 2 Disagree 3
29
Dont Know/ Cant Say 4
b c d
116
g 30 a b
c d e f
31
32
33
34
35
Husbands/in-laws do not accompany female TB patients to hospital /DOTS centers Female accompany their spouse to hospitals suffering from TB to hospitals /DOTS centre Females suffering from TB face problem in marriage Which of the following you would Yes No DK/CS agree to do? 1 2 3 Share a meal with person you know had TB If you suspect one of the female member is suffering from TB, do you take her to hospital Marry your daughter to a boy knowing had a TB Isolate your family member having TB from the household Marry your son to a girl who you know had TB Send your daughter in law to parents house if she had TB in order to protect other family members from TB In your community, how is the Most people reject him or her 1 person suffering from TB usually Most people are friendly but they generally 2 treated? try to avoid him/her Community mostly support and help him/her 3 Others (specify) 4 Do you know anyone in your family Yes 1 and neighborhood suffering from TB No 2 in the last 2 year DK/CS 3 If yes, have you given any advice to Go to Government Hospital 1 them? Go Private hospital 2 Isolate the family from the community 3 Any other- (specify) 4 None 5 Have you taken any initiative towards Yes 1 generating awareness about TB & No 2 DOTS within your community? If yes, what are they? Organized camps 1 Organized rallies 2 Organized lectures /Seminars/ Workshops 3 Worked as DOT provider 4 Nukkad Nataks/ Street Plays/Skits 5 Any other (Specify) 6
If coded 2 & 3 skip to 34
If coded 2 skip to 36
117
36
37
38
39
MEDIA HABIT & PREFERENCES Which source of information you are Newspaper & Magazines exposed to? Radio (Multiple Response Possible- Probe) TV Hoardings/posters/leaflets/Wall printing/ Bill Boards Internet Melas/ Nukkad Nataks etc Any other (Specify) If responded code 2 in Q.36 Which Vividh Bharti Station do you generally listen to? FM (Specify) Regional Channel Community Radio Any other (specify) Which program do you like most on News Radio? Drama / Serial Film songs (Multiple answers) Folk songs Health discussion Any other (specify) If responded codes 3 in Q.36 Which Channel watchs mostly Television channel do you generally watch? Channel (Multiple Response Possible) Channel
1 2 3 4 5 6 7 1 2 3 4 5 1 2 3 4 5 6 1 2 3
40
41
Channel 4 Which programs do you like the most News 1 on TV? Drama/Serial 2 (Probe for two most liked programs) Entertainment 3 Health Related Programs 4 Advertisements 5 Folk music 6 Music 7 Films 8 Any other (Specify)-------------------------------------9 Do you read newspaper? Yes 1 No 2 Which language paper generally is English read by you? Hindi Local language Names of the newspapers you usually News Paper read? News Paper News Paper Have you ever seen an Yes advertisement/ information on No Tuberculosis or DOTS? DK/CS 1 2 3 1 2 3 1 2 3
If coded 2, then skip to Q.43
42(a)
42(b)
43
If coded 2 & 3, then skip to Q.45
118
44
If Yes, where did you see such advertisement or/and information on TB/DOTS? (Multiple Response Possible)
Newspaper & Magazines Radio TV Hoardings/posters/leaflets Melas/ Nukkad Nataks etc Any other INFORMATION SOURCES
1 2 3 4 5 6 1 2 3 4 5 6 7 8 9 10 11 12 13 14 1 2 3 1 2 3 4 5 6 7 8 1 2 3 4 5 6 7
45
46
47
48
Q. No 49
TV Radio Cinema Newspaper / Magazines Hoarding/Posters/billboards/ Wall writing Public service announcements Drama/Skits/Street plays Hospital/doctor Friends & Relatives Health & related workers DOTS providers Internet None of these Any other (specify) Did anyone visit to make community Yes aware and provide information on TB No during last two years? DK/CS If yes, who visited? Government Doctor (Multiple Response Possible) Private Doctor AWW ASHA Health worker Worker from an NGO Any others Dont remember Mostly on what specific aspects Symptoms of Tuberculosis information is provided? Prevention from Tuberculosis (Multiple Response Possible) Cure for Tuberculosis DOTS Place of Treatment Information on prevailing myths about TB patients Any other (Specify) Questions Response Where from would you prefer to get TV information on TB and related issues? Radio (Multiple Response Possible) Cinema Newspaper / Magazines Hoarding/Posters/billboards/ Wall writing Public service announcements Drama/Skits/Street plays/Melas Hospital Friends & Relatives Health workers NGOs Any other (Specify)
What are your sources of information for awareness on Tuberculosis related issues? (Multiple Response Possible)
If coded 2 & 3 skip to 49
Skip
1 2 3 4 5 6 7 8 9 10 11 12
119
Q. No 50
Questions According to you what are the two most important issues regarding tuberculosis which need utmost attention? Do you have any suggestions how you /your organization could be more helpful in addressing Tuberculosis related issues?
Response --------------------------------------------1 ---------------------------------------------2
Skip
51
THANKS FOR YOUR VALUABLE TIME
120
121
CHAPTER 1 INTRODUCTION India is the highest TB burden country accounting for nearly one-fifth of the global incidence. Tuberculosis (TB) is an infectious bacterial disease that spreads through the air and most commonly affects the lungs (pulmonary TB). Once infected, a person has only a 10% lifetime risk of developing the disease. The most common symptom of a person with pulmonary TB is cough of two weeks or more. Patients are usually diagnosed by sputum smear examination and once detected is curable with 6-8 months of treatment. The diagnosis (sputum smear examination) and treatment of TB is made available free of cost by Government of Indias Revised National Tuberculosis Control Programme (RNTCP). All TB patients under RNTCP are treated under directly observed therapy (DOT). In order to enhance the reach and visibility of the Programme, one of the major components of the Global Fund Round 9 India TB project aims to strengthen the civil society initiative to improve access to quality DOTS services and strengthen TB care and control, especially for marginalized and vulnerable populations. The project implemented through two civil society partners The Union, South-East Asia Regional Office, New Delhi and the World Vision, India specifically addresses these issues through the project activities on Advocacy, Communication and Social Mobilisation (ACSM) in identified 374 districts of the country. In this regard, in order to provide evidence based guidance to the civil society Principal Recipients in implementing the ACSM activities a baseline Knowledge, Attitude and Practices survey was conducted. The information generated through this survey was expected to be representative of the various demographic and social characteristics of population living in these districts, keeping in view the relationship between these characteristics to tuberculosis control, and the activities visualised under global fund Rd 9 India TB project and also act as a baseline to measure the impact of the project activities. GENERAL PROCEDURES FOR COMPLETING THE QUESTIONNAIRE To collect the information, you must understand how to ask each question, what information the question is attempting to collect, and how to handle problems that might arise during the interview. You must also know how to correctly record the answers the respondent gives and how to follow special instructions in the questionnaire. This part of the training manual is designed to familiarize you with the Questionnaire. A. ASKING QUESTIONS
It is very important that you ask each question exactly as it is written in the questionnaire. When you are asking a question, speak slowly and clearly so that the respondent will have no difficulty hearing or understanding the question. At times you may need to repeat the question to be sure the respondent understands it. In those cases, do not change the wording of the question but repeat it exactly as it is written. If, after you have repeated a question, the respondent still does not understand it, you may have to restate the question. Be very careful when you change the wording, however, that you do not alter the meaning of the original question.
122
In some cases, you may have to ask additional questions to obtain a complete answer from a respondent (we call this probing). If you do this, you must be careful that your probes are neutral and that they do not suggest an answer to the respondent. Probing requires both tact and skill, and it will be one of the most challenging aspects of your work as an interviewer. B. RECORDING RESPONSES In this survey, all interviewers will use pens with blue/black ink to complete all questionnaires. Supervisors will do all their work using pens with red ink. Never use a pencil to complete the survey questionnaire. There are three types of questions in the questionnaire: 1) questions that have pre-coded responses; 2) questions that do not have pre-coded responses, i.e., that are open-ended; and 3) filters. 1. Questions with pre-coded responses For some questions, we can predict the types of answers a respondent will give. The responses to these questions are listed in the questionnaire. To record a respondents answer, you merely circle the number (code) that corresponds to the reply. Make sure that each circle surrounds only a single number. Example: 5 Does your household own any agricultural land? Yes ......1 No..2
In some cases, pre-coded responses will include an Other category. The other code should be circled, When the respondents answer is different from any of the pre-coded responses listed for the question. Before using the other code, you should make sure the answer does not fit in any of the other categories. When you circle the code other for a particular question you must always write the respondents answer verbatim in the space provided. If you need more room, use the margins or the comments section at the end. Example: 2. Recording responses that are not pre-coded The answers to some questions are not pre-coded but require that you fill in write the respondents answer in the space provided. Boxes without preceding codes. Whenever boxes are present without codes in front of them, you must enter information in all of the boxes. Example: Age of a person 1. Marking Skips
While following skipping, the Interviewer shall mark in the question from where the skipping is done so that we are sure that skipping is followed rightly.
123
Example: 1 What are the most common TB Mentioned diseases you are aware of? TB Not mentioned 1 2 IF coded (1) then skip to 19
For filter questions, it is important that you follow the instructions that ask you to check back to an earlier question. Do not rely on your memory. Remember that you do not need to ask the respondent the same question a second time. Check back and mark a in the appropriate box in the lter, then follow the skip instructions. 3. CHECKING COMPLETED QUESTIONNAIRE It is the responsibility of the interviewer to review each questionnaire when the interview is finished. This review should be done before you leave the place so that you can be sure every appropriate question was asked, that all answers are clear and reasonable, and that your handwriting is legible. Also check that you have followed the skip instructions correctly. You may be able to make minor corrections yourself, but any in many cases you will need to talk further with the respondent. Simply explain to the respondent that you made an error and ask the question(s) again. Do not recopy questionnaires. As long as the answers are clear and readable, it is not necessary that the questionnaire itself be neat. Every time you transcribe the answers to a new questionnaire, you increase the chance of an error. For this reason you are not allowed to use work sheets to collect information. Record all information on the questionnaires you have been provided. Anything out of the ordinary should be explained either in the margins near the relevant question or in the comments section at the end. These comments are very helpful to the supervisor and field editor in checking questionnaires. Comments are also read in the office and used to resolve problems encountered during data entry. This instruction manual contains detailed guidelines for canvassing of following six schedules during Baseline Survey:
-
House listing Schedule General Population Schedule TB Affected Schedule Health Functionaries Schedule Opinion Leaders Schedule NGO/CBO Schedule
(Please note that the schedule of Opinion Leaders & NGO CBO is quite similar to General Population, Thus, the detailed description has not provided for these questionnaires)
124
CHAPTER 2 HOUSELISTING SCHEDULE The House list is intended to provide the complete list of houses and households within each house for ensuring complete coverage by serving as the frame for canvassing of TB Affected Schedule within the selected sample unit (Village/Segment of a village in case of rural sample units and Census Enumeration Block in case of an urban sample unit). Besides the identification particulars of the house and the household, the House listing Schedule would record the name of the head of the household, Usual Member of the household, family member suffered from any disease, family member suffered from Tuberculosis and whether taken any treatment or not. 2.1 Identification Particulars of the Household
The identification particulars such as State, District, Sample unit and Village/ward, are to be recorded with names & codes wherever relevant. The following example illustrates the system for allotting the names/codes which have been discussed item by item in details: State Code (Numeric): A two digit code for states is to be followed here. In the above example, the state code '01' belongs to Uttar Pradesh. In total, there will be 15 state code. District Code (Numeric): A two digit code for the districts within a state is to be adopted. In the above example, the district code '04' belongs to Maharajganj Primary Sampling Unit Code (Numeric): A running two digit Code starting from 01-15 has been provided for the sample units within a District of a state Village /ward Name: Name of the selected village/ward is to be written
2.2
Details of the Household
Name of the head of the Household: The Head of the household is a person who is recognized as such by the members of the household and generally has the major say in taking important decisions relating to the household Address of the Household: It includes, Building no and House No. of the household Usual Resident of the Household: The usual resident members of the household are those who usually live together and share a common kitchen Disease Prevalence in family: Whether any family member suffered from any of the disease in the last one year? TB Affected Individuals: Whether family member are affected by Tuberculosis? Treatment for Tuberculosis: Whether any treatment has been taken for Tuberculosis?
125
CHAPTER 3 GENERAL POPULATION SCHEDULE 3.1 General Information
Questionnaire ID Number: A unique ID will be provided at the time of data entry Date of Interview: Interviewer will capture the date of interview State Code: A two digit code for states is to be followed here. In the above example, the state code '01' belongs to Uttar Pradesh. In total, there will be 15 state codes. Name of Respondents & Interviewer: Name of the respondents & interviewer will also be recorded District: Name & code of District District Specification: Tribal or Non-Tribal area Type of Settlement: Urban or Rural Block: Name and Code of Block Village: Name and Code of village
3.2
Informed Consent
The respondents consent for participation in the survey must be obtained before you begin the Interview. Read the informed consent statement exactly as it is written. This statement explains the purpose of the survey. It assures that respondent participation in this survey is completely voluntary and that s/he can refuse to answer any questions or stop the interview at any point. It will also need to clarify that this information will kept completely confidential. It will be used for research purpose only. 3.3 Questionnaire
Q.1 Name of the Respondent: Q.2 Gender: Male or Female. Please asks the name of respondent interviewed for the study. Q.3 Age: This is one of the most important questions in the interview, since almost all analysis of the survey data depends on the respondents age. Please ask how old you were in your last birthday. Q.4 Literacy: The term school means formal schooling, which includes primary, secondary, and postsecondary schooling and any other intermediate levels of schooling in the formal school system. However, it does include technical or vocational training beyond the primary-school level, such as longterm courses in mechanics or secretarial work or ITI course. Q.5 Occupation: The nature of occupation of a worker or activity status of a non-worker as the case may be is to be recorded here. These occupations/activity have been explained, in brief, along with their code structure for better understanding.
126
Item Wage laborer Skilled worker Self employed
Description A manual worker who works for wages in kind or cash in agriculture and non-agriculture activities. Persons who got certain skills like carpenter, Tailor, shoemaker etc Persons who are engaged in their own enterprises or are engaged independently in a profession or trade on own account or with one or a few partners. The regular employees working in others enterprises (Government and Private) and getting in return salary or wages on a regular basis Person who is doing their own business A person who is engaged in cultivation of land owned or leased in from government or from private person(s) or institution for payment in money, kind or share. Cultivation also includes effective supervision or direction in cultivation. Did not work but was seeking and/or available for work Attending routine domestic chores, etc. Attending educational institutions / Not able to work due to disability Beggars, Pensioners, Too old to work etc
Code 1 2 3
Service (Govt. & Private)
Business Agriculture/cultivator
5 6
Unemployed House wife Student / Handicapped/ etc Any other (specify)
7 8 9 10
Q.6 Household Income: This question refers to average income earned by the all the members of the household. Please encircle the response explained in the questionnaire Q.7 Marital Status: This question refers to the marital status as on the date of survey Item Currently Married Unmarried Divorced Widow/Widower Separated Description If the person is married and living together with current spouse. If the person is not married If the person is divorced If the person was married but his/her spouse is died. Code
1
2 3 4
If the person was married, but has legally obtained a divorce 5 from his/her spouse.
Q.8 : Type of Family : This question asks the type of family, whether it is single, Joint or extended type Q. 9 Type of House: This is an observation question. See the responses and circle accordingly on: Pucca House: Flooring, roof & walls should be cemented/Concrete etc. Semi-Pucca House: Temporary roofs could be with cemented floor & wall or any one of it. Kachha House: Thatched roofs, mud walls with no floorings
127
Q. 9 (a) Ownership of House: Ask whether anyone in your family owns a house whether it is the house where you are residing or any Other house and circle on respective code. Q. 10 Household Items: The answers to these questions on ownership of certain items will be used as a rough measure of the Socio economic status of the household. Read out each item and circle the answer given after each item. Do not leave the codes for any item(s) blank. It does not matter who in the household owns the item; only that the item is owned by the household or one of its usual members. Code 1 YES even if the household has illegal electricity connection, Q.11 Source of Water: The purpose of this question is to assess the cleanliness of the households drinking water by asking about the households main source of water. If drinking water is obtained from several sources, probe to determine the source from which the household obtains the majority of its drinking water. If the source varies by season, record the main source used at the time of interview. Item Private Tap Description Pipe connected with in-house plumbing to one or more taps, e.g. in the Kitchen and bathroom. Sometimes called a house connection. In-house pipes connected to a public or private water distribution system. Pipe connected to a tap outside the house in the yard or plot (and the Water is coming from a public or private water distribution system).Sometimes called a yard connection. Private hand pump which may be inside the house and may be used to pull the water from ground through hand pump. Public water point from which community members may collect water (and the water is coming from a public or private water distribution system). A standpipe may also be known as a public fountain or public tap. Public standpipes can have one or more taps and are often made of brickwork, masonry or concrete. Public hand pump which will be outside and community members may collect water. People have to pull the water from ground through hand pump. A deep hole that has been driven, bored or drilled with the purpose ofreaching ground water supplies. Water is delivered from a tubewell orborehole through a pump which may be human, animal, wind, electric, diesel or solar-powered. Water is obtained from a provider who uses a truck to transport water into the community. Typically the provider sells the water to households. Water located above ground and includes rivers, dam Rain that is collected or harvested from surfaces by roof or ground catchment and stored in a container, tank or cistern. s, lakes, well, ponds, streams, canals, and irrigation channels Water located above ground and includes rivers, dams, lakes, well, ponds, streams, canals, and irrigation channels Bottled water: Water that is bottled and sold to the household in bottles. Code 1
Private Hand Pump Public Tap
2 3
Public Hand Pump
Tube Well
Supply tanker
River/pond/Steam/Waterfalls
Rain water Packaged Water
8 9
128
Q. 12
Separate Room for Cooking
If the cooking is done in the house, the respondent is asked whether there is a separate room that is used as a kitchen. This question provides additional information on the hygiene and air quality status of the household. Q.13 Below Poverty Card (BPL Card)
The BPL card is a card given to households below the poverty line. We are interested about currently how many households have BPL cards that can be used to avail benefits. Q. 14 Type of Fuel
This question capture the response on the type of fuel used by the respondent for cooking purpose. Please encircle the correct response. It is a single coded response.
Q, 15 & 15 (a) Health Seeking Behavior This question captures the health seeking behavior of people. If somebody falls ill, the place where people generally go for treatment for any kind of illness. The next question is in continuation of this question; the reason for not going to Government hospitals. Q. 16 & 16 (a) TB Treatment seeking Behaviors This question is asked to know the TB treatment behavior of people. If anyone suffers from cough of 2 weeks, would they visited health centre for sputum examination or not Q. 17 & 18 Knowledge & Awareness of TB & Its treatment Ask the respondents about the common diseases they are aware of; if TB mentioned or not. If TB is not mentioned then ask whether they heard of it. Q. 19 -Q.21 Symptoms and Cause of Tuberculosis This question pertains to awareness on symptoms and cause of Tuberculosis. The persons who are more prone to get infection of TB. All three questions are multiple response questions.
Q. 22 & 23: Source of TB Treatment Ask the respondents, if anybody is suspected to be affected from the disease, where they should go for checking and if anybody is diagnosed with the disease, the place where they should go for the treatment. Both of the questions are single coded. Q.24 29: Seriousness of TB and its Treatment This question record the response of individual on the seriousness of the TB disease and whether there is any cure of this disease or not. Further, the best treatment for the disease and duration of treatment.
129
Q. 28 Diagnosis of TB This question asks about the techniques which are used to diagnose whether the person suffers from TB or not Item Sputum Smear Test XRay Mantoux Skin Test Description It is a laboratory test that looks for fungus in sputum sample Chest X ray can be done to diagnose Tuberculosis. In active pulmonary TB cavities are often seen in the upper lungs The Mantoux skin test is given by using a needle and syringe to inject 0.1 ml of 5 tuberculin units of liquid tuberculin between the layers of the skin, usually on the forearm If person has performed any other test for TB diagnosis Dont know or Cant say Code 1 2 3
Any Other (Specify) DK/CS
4 5
Q.29 & 30 Awareness of source of Treatment This question records the awareness of the places where diagnosis of TB can be done and places where treatment of TB can be done. This is a multiple response question. This question is asked to find the peoples awareness on DOTS centre.
Q. 32 35 Awareness of DOTS This question captures the awareness regarding DOTS, place where DOTS is available and DOTS treatment is free of cost. Q. 31 & 36 General Perception of TB This question collects the General Perception of TB specifically, Is it possible that anyone can suffer from TB. If they dont think, what are the reasons for this? Another question asks whether there is complete cure for TB or not. Q. 37 39 Stigma & Discrimination Stigma is a process of producing and reproducing inequitable power relations, where negative attitudes towards a group of people, on the basis of particular attributes such as their TB status, HIV status, gender, sexuality or behavior, are created and sustained to legitimatized dominant groups in society. Discrimination is a manifestation of stigma. Discrimination is any form of arbitrary distinction, exclusion or restriction, whether by action or omission, based on a stigmatized attribute. These questions collect the information on stigma and discrimination mainly social stigma and Self stigma and Gender Discrimination associated with the Tuberculosis. Q. 40 43 Self Initiative to Control TB
This question asks the respondents, if they know anybody who is suffering from the disease, If the response is Yes, whether they had given any advice for treatment, and taken any initiative to generate awareness about TB and DOTS in the community.
130
Q.44 Media Habit & Preferences This question record the media habit and source of information people are exposed to. Q. 45 46 Radio listening This is a continuation of question 44, if people report Radio as their source of information, then which radio station they generally listen. Please record the other regional radio channel also. The next question record the programs generally liked by people on radio. This question will help in assessing the peoples interest on health related programs. Q. 47 48 TV Preference This is a continuation of question 44, if people report TV as their source of information, then which TV channel they like the most. Please record four most watched TV channel. The next question record the programs generally liked by people on radio. This question will help in assessing the peoples interest on health related programs. Q.49-50 Newspaper Preference This question asks the newspaper reading habit of persons. If respondents read newspaper, then its preferred language and its names. Q.51-56 Source of TB related Information This question is very much similar to earlier questions. This question asks if respondents have seen or heard of TB related information. If respondent gives code Yes, then its source of information. Q.53 & 54 asks the respondents of their preferential source of Health related information and TB related information. Q.55 asks whether respondents can recall any message on TB. If coded Yes then record its verbatim. Q. 57 62 Governments Initiative on Tuberculosis This question is to be asked from those people who are non aware about Tuberculosis. If anyone visited their house to provide information on TB. If respondents coded Yes, then who visited and provided information on specific aspect.
131
TB AFFECTED PERSONS SCHEDULE 4.1 General Information
Questionnaire ID Number: A unique ID will be provided at the time of data entry Date of Interview: Interviewer will capture the date of interview State Code: A two digit code for states is to be followed here. In the above example, the state code '01' belongs to Uttar Pradesh. In total, there will be 15 state codes. Name of Respondents & Interviewer: Name of the respondents & interviewer will also be recorded District: Name & code of District District Specification: Tribal or Non-Tribal area Type of Sample : Random or Booster Type of Settlement: Urban or Rural Block: Name and Code of Block Village: Name and Code of village
4.2
Informed Consent
The respondents consent for participation in the survey must be obtained before you begin the Interview. Read the informed consent statement exactly as it is written. This statement explains the purpose of the survey. It assures that respondent participation in this survey is completely voluntary and that s/he can refuse to answer any questions or stop the interview at any point. It will also need to clarify that this information will kept completely confidential. It will be used for research purpose only. 4.3 Questionnaire
Q.1 Name of the Respondent: Q.2 Gender: Male or Female. Please asks the name of respondent interviewed for the study. Q.3 Age: This is one of the most important questions in the interview, since almost all analysis of the survey data depends on the respondents age. Please ask how old you were in your last birthday. Q.4 Literacy: The term school means formal schooling, which includes primary, secondary, and postsecondary schooling and any other intermediate levels of schooling in the formal school system. However, it does include technical or vocational training beyond the primary-school level, such as longterm courses in mechanics or secretarial work or ITI course. Q.5 Occupation: The nature of occupation of a worker or activity status of a non-worker as the case may be is to be recorded here. These occupations/activity have been explained, in brief, along with their code structure for better understanding.
132
Item Wage laborer Skilled worker Self employed
Description A manual worker who works for wages in kind or cash in agriculture and non-agriculture activities. Persons who got certain skills like carpenter, Tailor, shoemaker etc Persons who are engaged in their own enterprises or are engaged independently in a profession or trade on own account or with one or a few partners. The regular employees working in others enterprises (Government and Private) and getting in return salary or wages on a regular basis Person who is doing their own business A person who is engaged in cultivation of land owned or leased in from government or from private person(s) or institution for payment in money, kind or share. Cultivation also includes effective supervision or direction in cultivation. Did not work but was seeking and/or available for work Attending routine domestic chores, etc. Attending educational institutions / Not able to work due to disability Beggars, Pensioners, Too old to work etc
Code 1 2 3
Service (Govt. & Private)
Business Agriculture/cultivator
5 6
Unemployed House wife Student / Handicapped/ etc Any other (specify)
7 8 9 10
Q.6 Household Income: This question refers to average income earned by the all the members of the household Q.7 Marital Status: This question refers to the marital status as on the date of survey Item Currently Married Unmarried Divorced Widow/Widower Separated Description If the person is married and living together with current spouse. If the person is not married If the person is divorced If the person was married but his/her spouse is died. Code 1 2 3 4
If the person was married, but has legally obtained a divorce 5 from his/her spouse.
Q.8 : Type of Family : This question asks the type of family, whether it is single, Joint or extended type Q. 9 Type of House: This is an observation question. See the responses and circle accordingly on: Pucca House: Flooring, roof & walls should be cemented/Concrete etc. Semi-Pucca House: Temporary roofs could be with cemented floor & wall or any one of it. Kachha House: Thatched roofs, mud walls with no floorings
133
Q. 9 (a) Ownership of House: Ask whether anyone in your family owns a house whether it is the house where you are residing or any Other house and circle on respective code. Q. 10 Household Items: The answers to these questions on ownership of certain items will be used as a rough measure of the Socio economic status of the household. Read out each item and circle the answer given after each item. Do not leave the codes for any item(s) blank. It does not matter who in the household owns the item; only that the item is owned by the household or one of its usual members. Code 1 YES even if the household has illegal electricity connection, Q.11 Source of Water: The purpose of this question is to assess the cleanliness of the households drinking water by asking about the households main source of water. If drinking water is obtained from several sources, probe to determine the source from which the household obtains the majority of its drinking water. If the source varies by season, record the main source used at the time of interview. Item Private Tap Description Pipe connected with in-house plumbing to one or more taps, e.g. in the Kitchen and bathroom. Sometimes called a house connection. Inhouse pipes connected to a public or private water distribution system. Pipe connected to a tap outside the house in the yard or plot (and the Water is coming from a public or private water distribution system). Sometimes called a yard connection. Private hand pump which may be inside the house and may be used to pull the water from ground through hand pump. Public water point from which community members may collect water (and the water is coming from a public or private water distribution system). A standpipe may also be known as a public fountain or public tap. Public standpipes can have one or more taps and are often made of brickwork, masonry or concrete. Public hand pump which will be outside and community members may collect water. People have to pull the water from ground through hand pump. A deep hole that has been driven, bored or drilled with the purpose of reaching ground water supplies. Water is delivered from a tubewell or borehole through a pump which may be human, animal, wind, electric, diesel or solar-powered. Water is obtained from a provider who uses a truck to transport water into the community. Typically the provider sells the water to households. Water located above ground and includes rivers, dam Rain that is collected or harvested from surfaces by roof or ground catchment and stored in a container, tank or cistern, lakes, well, ponds, streams, canals, and irrigation channels Water located above ground and includes rivers, dams, lakes, well, ponds, streams, canals, and irrigation channels Bottled water;Water that is bottled and sold to the household in bottles. Code 1
Private Hand Pump Public Tap
2 3
Public Hand Pump
Tube Well
Supply tanker
River/pond/Steam/Wate rfalls Rain water Packaged Water
8 9
134
Q. 12 Separate Room for Cooking If the cooking is done in the house, the respondent is asked whether there is a separate room that is used as a kitchen. This question provides additional information on the hygiene and air quality status of the household. Q.13 Type of Fuel This question capture the response on the type of fuel used by the respondent for cooking purpose This is a single response question
Q . 14 Below Poverty Card (BPL Card) The BPL card is a card given to households below the poverty line. We are interested about currently how many households have BPL cards that can be used to avail benefits.
Q, 15 & 16 Health Seeking Behavior This question captures the health seeking behavior of people. If somebody falls ill, where they generally go for treatment for any kind of illness? The next question is in continuation of this question; the reason for not going to Government hospitals. Q. 17 Q. 21 Cause of TB & Its treatment Ask the respondents about the cause of TB and the number of times they were diagnosed in the past for Tuberculosis. Q 21 also asks the place where respondent visited for treatment and whether they had completed the TB related treatment or not. Q. 22 Q.26 Symptoms & Treatment of Tuberculosis This question pertains to symptoms that had affected TB patients. The other question asked the respondents when did they visit health facility after the onset of symptoms. After how many days of onset of symptom, respondents found that they are suffering from tuberculosis. Q. 25 asks the number of health providers visited before the diagnosis of Tuberculosis Q. 26 34 Diagnosis of Tuberculosis These question asks the respondents about the diagnosis of tuberculosis, then place where TB diagnosis is being done, affected organ, whether sputum examination, chest X ray or any other blood test is being done or not. If the respondents paid for the diagnosis of tuberculosis. If coded Yes, then how much money are being paid by the respondents. Q.35 49 Treatment of Tuberculosis These question investigate the treatment availed by the respondents. This question captures the awareness regarding DOTS, place where DOTS is available and DOTS treatment is free of cost, duration of treatment, regularity of medicine, type of service provider and satisfaction with the service provider
135
Q. 50 54 Time & Cost incurred for TB Treatment These questions capture the information on the time and cost incurred for taking treatment of tuberculosis. Cost of treatment per day for travelling as well as on medicines. Q. 55 57 Governments Initiative for TB Treatment These questions ask the respondents whether anybody visit their house to check the regularity of medicine. If there is any child less than 6 yrs. If coded Yes then ask whether these children receiving any medicine for prevention of TB or not Q. 58 60 Identification of Personnels involved in Providing Health Related Information This question pertains to identification of Opinion leaders or other health provider involved in providing health related information to the TB affected persons. Q . 59 asks the name of the people visited their house to provide health related information. In Q. 60, ask the health care facility contacted for illness Q. 61 - 75 Stigma and Discrimination These questions capture the information on stigma and discrimination faced by TB affected persons at various levels. Some of the questions are based on their experiences, feelings and opinion as to how people with Tb feel and how they are treated. Q.61 65 asks the respondents of their disclosure status with family, friends and spouse. Q. 66 75 record the discriminatory practices with respect to gender and professional field Q.76 Media Habit & Preferences This question record the media habit and source of information people are exposed to. Q. 77-78 Radio listening This is a continuation of question 44, if people report Radio as their source of information, then which radio station they generally listen. Please record the other regional radio channel also. The next question record the programs generally liked by people on radio. This question will help in assessing the peoples interest on health related programs. Q. 79-80 TV Preference This is a continuation of question 44, if people report TV as their source of information, then which TV channel they like the most. Please record four most watched TV channel. The next question record the programs generally liked by people on radio. This question will help in assessing the peoples interest on health related programs. Q.81-83 Newspaper Preference This question asks the newspaper reading habit of persons. If respondents can read newspaper, then its preferred language and its names.
136
Q.84 86 Source of TB related Information This question is very much similar to earlier questions. This question asks if respondents have seen or heard of TB related information. If respondent gives code Yes, then its source of information. Q.87 89 asks whether respondents can recall any message on TB. If coded Yes then record its verbatim. Q. 90 93 Governments Initiative on Tuberculosis This question is to be asked from those people who are non aware about Tuberculosis. If anyone visited in their house to provide information on TB. If respondents coded Yes, then who visited and provided information on specific aspect.
137
CHAPTER - 4 HEALTH SERVICE PROVIDER
5.1
General Information
Questionnaire ID Number: A unique ID will be provided at the time of data entry Date of Interview: Interviewer will capture the date of interview State Code: A two digit code for states is to be followed here. In the above example, the state code '01' belongs to Uttar Pradesh. In total, there will be 15 state codes. District: Name & code of District PSU : Name & code of PSU Name of Doctor & Address: Name of the respondents & its address will also be recorded Respondents Category : Private Practitioner or Government Doctors
5.2
Questionnaire
Q.1 Name of the Respondent: Please ask the name of respondent interviewed for the study. Q.2 Gender: Male or Female. Q.3 Age: This is one of the most important questions in the interview, since almost all analysis of the survey data depends on the respondents age. Please ask how old you were in your last birthday. Q.4 Address: Please ask the record the complete address of the respondents Q.5 Educational Qualification: The highest level of education attained by the doctors. Q. 6 Year of Experience: Ask the respondents their number of year of experience Q.7 Nature of Practice: Item Dispensing GP Description Dispensing General Practitioner are those who can prescribe as well as dispense drugs to the patients Prescribing GP Prescribing General Practitioner are those who can only prescribe the drugs to the patients Consultant/Specialist Consultant/Specialist are those who specialize in particular area 3 2 Code 1
138
Q. 8 - 11 Awareness of TB Ask the respondents about the common diseases they are aware of; if TB mentioned or not. If TB is not mentioned then ask whether they heard of it. Q. 10 pertains to footfall of TB patients in their health facility, average number of people visit to health facility and its gender wise representation Q.12 Types of Tuberculosis This question asks the respondents about their knowledge on the type of tuberculosis or organs affected by tuberculosis.
Item Pulmonary TB (Chest/Lungs) Lymph TB Glands TB Spinal TB Bone TB Abdominal TB Any other
Description If lung/chest is affected by Tuberculosis, then it is considered as Pulmonary TB If lymph or lymph nodes is affected by Tuberculosis, then it is considered as Lymph TB Any of the Glands is affected by TB Spinal Cord is affected by TB If part of bone is affected by TB Abdomen is affected by TB Any other body part
Code 1 2 3 4 5 6 7
Q. 13 Symptoms of Tuberculosis This question pertains to common symptoms of Tuberculosis observed by doctors while checking TB patients. It is a multiple response question Q. 14 & 15 Awareness and Diagnosis of MDR TB This question asks the respondent on their knowledge on MDR TB. Multidrug resistant TB is defined as TB that is resistant to the two most powerful anti TB drug. If respondent coded Yes, then its diagnosis by the respondents.
Q. 16 & 17 Diagnosis of Pulmonary TB This question asks about the investigation advised by doctors to the patients. The next question asks about the most preferential test for diagnosis of TB and the reasons for selecting the test Item Description Code Sputum Smear Test XRay Mantoux Skin Test It is a laboratory test that looks for fungus in sputum sample Chest X ray can be done to diagnose Tuberculosis. In active pulmonary TB cavities are often seen in the upper lungs The Mantoux skin test is given by using a needle and syringe to inject 0.1 ml of 5 tuberculin units of liquid tuberculin between the layers of the skin, usually on the forearm Culture the sputum for diagnosis If person has performed any other test for TB diagnosis 1 2 3
Culture Any Other (Specify)
4 5
139
Q. 18 22 Details of Sputum Smear Examination These questions investigate the frequency of sending the patients for sputum smear examination, place for sending the patients for sputum smear examination. The next question asks whether Doctors faced any problem in getting sputum smear examination done for TB suspects in Designated Microscopy centre. If coded Yes then ask for reasons.
Q. 23 26 Treatment of Tuberculosis These questions pertains to the treatment of tuberculosis with special reference to place for treatment, system of medicine, average duration of treatment, and knowledge on cure of Tuberculosis Q.26 28 Records of Tuberculosis Patients These questions ask the respondents about maintaining of records for TB patients, Number of TB patients treated by Doctors per year and number of patients completing their TB treatment. Q.29 31 Difficulties in Treating TB patients These questions ask the main problems faced by Doctors in treating TB patients. Whether, they examine family members of other patients also. Doctors opinion on the treatment of TB. Q.32 Precautions while treating TB patients This question asks the precautions taken by Doctors while treating or examining the patients.
Item
Description
Code
Maintain distance
Maintain Distance from the TB patients while examining or treating them
Wear masks & gloves
Wear Masks on their face and gloves on their hands
Wash hands with soap
Wash their hands with soap after examining or treating TB patients
None
Do nothing
Any Other (Specify)
If they have used any other measure of precaution
140
Q.33 Suggest Precautions to TB Patients These questions asks the respondents about the precautionary measures suggested to TB patients Item Cover your face while coughing Use separate utensils Not to spit anywhere Use separate towels/clothes Isolate the patient Any other Description Cover their face with handkerchief or any other clothes while coughing in public Use separate utensil for eating purpose Do not spit in any places Use of separate clothes & towels. Do not share their clothes Isolate the patients If suggested, any other precautionary measures Code 1 2 3 4 5 6
Q. 34 40 Details of DOTS These questions ask the respondents whether they had heard of DOTS. If coded Yes, their main source of information for DOTS. Perception about DOTS treatment and involvement in DOTS program run by the government. Q.37 & 39 is to be asked from only Private practitioners. Whether, they are aware of any schemes of involvement of private practitioners in DOTS program. Q. 40 This question investigates the stigma attached with the disease. Whether people avoid visiting to the doctors by knowing they treat TB patients. Q.41- 42 Source of Information These questions ask the respondents the source of information for TB related knowledge. According to respondents, their best medium to generate TB awareness among community Q. 43 Place for Getting Anti TB Drugs Item Government NGO Local Chemist On your own Description PHC,CHC, District Hospital , DOTS centre etc Non - governmental Organizations Hospitals Local Chemist who provide medicines Provide medicine on their own Code 1 2 3 4
Q. 44 Suggestions This is an open ended question where Doctors are asked to provide their suggestion to strengthen TB control services
141
CALCULATION OF STANDARD OF LIVING INDEX Scores HOUSEHOLD CHARACTERISTIC 1 2 3 House type Separate room for cooking Ownership of house - pucca =4 - yes=1 - yes=1 - electricity, liquid petroleum gas or biogas=2 - pipe, hand pump, well in residence/ yard/ plot=2 - yes=4 - yes=3 - yes=4 -Yes = 3 -Yes = 3 -Yes = 3 - yes=3 - yes=3 - yes=3 - yes=2 - yes=2 - yes=2 - yes=2 - yes=2 - yes=1 - semi pucca=2 - no=0 - no=0 - coal, charcoal or kerosene=1 - kachha=0
Main fuel for cooking
- other fuel=0
Source of drinking water
- public tap, hand pump or well=1 - no=0 - no=0 - no=0 - no =0 - no =0 - no =0 - no=0 - no=0 - no=0 - no=0 - no=0 - no=0 - no=0 - no=0 - no=0
- other water source=0
6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Car Moped or scooter Tractor Computer Telephone Mobile phone Refrigerator Colour TV Black and white TV Bicycle Electric fan Radio or Transistor Sewing machine Mattress Pressure cooker
142
Scores HOUSEHOLD CHARACTERISTIC 21 22 23 24 25 26 27 Chair Cot or bed Table Clock or watch Water pump Bullock cart Thresher - yes=1 - yes=1 - yes=1 - yes=1 - yes=2 - yes=2 - yes=2 - no=0 - no=0 - no=0 - no=0 - no=0 - no=0 - no=0
Low SLI = 0 14 (Low) Medium SLI = 15-24 (Medium) High SLI = 25 60 (High)
143
STATE & DISTRICT CODE State Uttar Pradesh Uttar Pradesh Uttar Pradesh Uttar Pradesh Punjab Haryana Haryana Rajasthan West Bengal Orissa Orissa Bihar Bihar Bihar Bihar Mizoram Karnataka Tamil Nadu Tami Nadu Tamil Nadu Kerala Kerala Andhra Pradesh Maharashtra Chhatisgarh State Code 01 01 01 01 02 03 03 04 05 06 06 07 07 07 07 08 09 10 10 10 11 11 12 13 14 District Agra Banda ** Faizabad Maharajganj** Hoshiarpur Panipat Sirsa Jhunjhunun Uttar Dinajpur Bhubaneshwar Corp Koraput Lakhisarai ** Nalanda ** Purnia ** Saran ** Aizwal Bijapur Erode Vellore Nagapattinam Thiruvananthapuram Kollam Medak Mumbai Kanker * CODE 01 02 03 04 05 06 07 08 09 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
144
State Madhya Pradesh Madhya Pradesh Madhya Pradesh Madhya Pradesh Madhya Pradesh
State Code 15 15 15 15 15
District Bhopal Hoshangabad ** Sehore ** Sagar ** Barwani
CODE 26 27 28 29 30
You might also like
- 2013 StreetsDocument95 pages2013 StreetsBalu KateNo ratings yet
- MagatismDocument22 pagesMagatismJames MasomeNo ratings yet
- Tugas B.inggris Writing Simple ReportDocument11 pagesTugas B.inggris Writing Simple ReportNazwa Aulia Bahtiar PutriNo ratings yet
- Final Research 2Document43 pagesFinal Research 2Ma Leslie BuhanghangNo ratings yet
- 2015 Role of Community Health Workers in Disease Surveillance in IndiaDocument30 pages2015 Role of Community Health Workers in Disease Surveillance in IndiaKiran KumbharNo ratings yet
- Community Based Rehabilitation Part IDocument46 pagesCommunity Based Rehabilitation Part INabil Abd El-tawabNo ratings yet
- Final Doc1Document57 pagesFinal Doc1saisreeknsNo ratings yet
- Atlas of Multiple SclerosisDocument56 pagesAtlas of Multiple SclerosishmarcalNo ratings yet
- HIV Sentinel Surveillance 2012-13 Technical BriefDocument54 pagesHIV Sentinel Surveillance 2012-13 Technical BriefvemalNo ratings yet
- Sociology Project Work (1785& 1812)Document61 pagesSociology Project Work (1785& 1812)Ritik DocumentsNo ratings yet
- PDFDocument46 pagesPDFEnrico_LariosNo ratings yet
- Tutor Hari 1Document11 pagesTutor Hari 1wina winaNo ratings yet
- Final RP Jolly - Doc1Document6 pagesFinal RP Jolly - Doc1HAKIZIMANA PierreNo ratings yet
- Final ProposalDocument5 pagesFinal ProposalKs ZaraNo ratings yet
- Manual PM 1-08Document369 pagesManual PM 1-08pastizal123456No ratings yet
- SERIOUS ILLNESS COMMUNICATION PROJECT - ProtocolDocument142 pagesSERIOUS ILLNESS COMMUNICATION PROJECT - ProtocolcharmyshkuNo ratings yet
- 2021 Mpoc NBDocument32 pages2021 Mpoc NBKatie LevasseurNo ratings yet
- MSF-H Assessment ManualDocument131 pagesMSF-H Assessment Manualapi-3731030100% (2)
- Ekitela David Project ProposalDocument25 pagesEkitela David Project ProposalDavid EkitelaNo ratings yet
- LugobaDocument8 pagesLugobagabrielNo ratings yet
- Community Participation Final DraftDocument85 pagesCommunity Participation Final DraftMPHO RAPELANGNo ratings yet
- Compendium FinalDocument100 pagesCompendium Finalkhuzwayononjabulo0No ratings yet
- Accelerated Action Plan On HTS 2019Document55 pagesAccelerated Action Plan On HTS 2019PatrickLnanduNo ratings yet
- ViewDocument68 pagesViewMOKSHITA SHARMANo ratings yet
- Pantawid Pamilyang PilipinoDocument59 pagesPantawid Pamilyang PilipinoRinaNo ratings yet
- RESEARCH TOPIC EuniceDocument38 pagesRESEARCH TOPIC EuniceShariff Oluoch OdiwuorNo ratings yet
- Covid-19 Pandemic Inida: Analysis Report ON " " 2019-2020 Submitted byDocument36 pagesCovid-19 Pandemic Inida: Analysis Report ON " " 2019-2020 Submitted byshital shermaleNo ratings yet
- LWS Operational GuidelinesDocument94 pagesLWS Operational GuidelinesNidhi DubeyNo ratings yet
- Charo ProposalDocument29 pagesCharo ProposalMercy NdungeNo ratings yet
- CARE OFDA COVID 19 Response End Line Survey Report Dec 2020 FinalDocument17 pagesCARE OFDA COVID 19 Response End Line Survey Report Dec 2020 FinalBiniyam YitbarekNo ratings yet
- Heart Disease Prediction Final ReportDocument31 pagesHeart Disease Prediction Final ReportMUSIC BY LOSTNo ratings yet
- Social Determinants of NCD and Other Publlic Health Issues in Seychelles Who Published 2013Document141 pagesSocial Determinants of NCD and Other Publlic Health Issues in Seychelles Who Published 2013neniNo ratings yet
- TB ResistantDocument64 pagesTB ResistantAmelia AlresnaNo ratings yet
- FUTURE DIAGNOSTIC OF HIV TESTING-7 FixDocument24 pagesFUTURE DIAGNOSTIC OF HIV TESTING-7 FixActysya virsha aurra phianda cahyadj putriNo ratings yet
- Gaza Projections ReportDocument57 pagesGaza Projections ReportDavide FalcioniNo ratings yet
- Kenboi C. Kenneth ResearchDocument31 pagesKenboi C. Kenneth ResearchRodgers KirwaNo ratings yet
- Buku Pegangan Konselor Hiv-Aids PDFDocument306 pagesBuku Pegangan Konselor Hiv-Aids PDFDewi Ratna SariNo ratings yet
- Syndromic Surveillance Implementation Guide Release 1 4Document127 pagesSyndromic Surveillance Implementation Guide Release 1 4WASI MIRZANo ratings yet
- QMP Practical InstructionDocument47 pagesQMP Practical InstructionJerome PrattNo ratings yet
- LFE ReportDocument10 pagesLFE ReportPranto AhmedNo ratings yet
- Mobile Healthcare App Using AndroidDocument34 pagesMobile Healthcare App Using Androida4athira100% (2)
- Crowdsourced Geographic Information Use in GovernmentFrom EverandCrowdsourced Geographic Information Use in GovernmentNo ratings yet
- Debre Markos University College of Medicine and Health ScienceDocument29 pagesDebre Markos University College of Medicine and Health ScienceYitbarek GuadieNo ratings yet
- HIV Outcome Evaluation - Final - ReportDocument75 pagesHIV Outcome Evaluation - Final - ReportAbel Gebrehiwot AyeleNo ratings yet
- 2009 Outcome Monitoring Survey: USAID/Madagascar Programs (USAID/2009)Document49 pages2009 Outcome Monitoring Survey: USAID/Madagascar Programs (USAID/2009)HayZara MadagascarNo ratings yet
- Report On Community Health DiagnosisDocument118 pagesReport On Community Health DiagnosisRubina Pulami100% (15)
- TB Caravan GuideDocument22 pagesTB Caravan GuideMajo Napata100% (1)
- NCD Surveillance in Public Health: Participant GuideDocument22 pagesNCD Surveillance in Public Health: Participant GuideRafikarsNo ratings yet
- Heart Disease Prediction SynopsisDocument36 pagesHeart Disease Prediction SynopsisMUSIC BY LOSTNo ratings yet
- NSP Draft 20.02.2017 1 PDFDocument109 pagesNSP Draft 20.02.2017 1 PDFTanmay KulkarniNo ratings yet
- MSF Manual Assessment of Health and Hum. Emergencies (2002)Document110 pagesMSF Manual Assessment of Health and Hum. Emergencies (2002)AwashNo ratings yet
- MAAVN001 Final KAP Report DF CC 0611Document35 pagesMAAVN001 Final KAP Report DF CC 0611Baleegh Al-sharabyNo ratings yet
- Paper PDFDocument66 pagesPaper PDFAbiy SeyoumNo ratings yet
- Research Report Prevalence and Associated Factors of Hypertension Among Young AdultDocument33 pagesResearch Report Prevalence and Associated Factors of Hypertension Among Young AdultPitambar PoudelNo ratings yet
- Unique Identifier Codes: Guidelines For Use With Key PopulationsDocument36 pagesUnique Identifier Codes: Guidelines For Use With Key PopulationsGarvit GargNo ratings yet
- Global Burden Disease Influenza ENGDocument22 pagesGlobal Burden Disease Influenza ENGjeanNo ratings yet
- Su 6103Document44 pagesSu 6103Yulisa Prahasti Dewa AyuNo ratings yet
- FNP Led Mobile Health Services For The Homeless PopulationDocument88 pagesFNP Led Mobile Health Services For The Homeless PopulationslyvesterNo ratings yet
- Public Health and the Environment - Second Edition: Uncovering Key Social, Ecological, and Economic ConnectionsFrom EverandPublic Health and the Environment - Second Edition: Uncovering Key Social, Ecological, and Economic ConnectionsNo ratings yet
- SanchezDocument10 pagesSanchezYet Barreda BasbasNo ratings yet
- Nogales V CMCDocument4 pagesNogales V CMCYet Barreda BasbasNo ratings yet
- 16pf Oen FactsheetDocument3 pages16pf Oen FactsheetYet Barreda BasbasNo ratings yet
- Tos CoursespecsDocument4 pagesTos CoursespecsYet Barreda BasbasNo ratings yet
- LiuDocument14 pagesLiuYet Barreda BasbasNo ratings yet
- Hagglund, Et Al.Document8 pagesHagglund, Et Al.Yet Barreda BasbasNo ratings yet
- Attention-Deficit/Hyperactivity (ADHD) Symptom Checklist: ImpulsivityDocument1 pageAttention-Deficit/Hyperactivity (ADHD) Symptom Checklist: ImpulsivityYet Barreda BasbasNo ratings yet
- Diagnostic Parent Rating Scale 1Document3 pagesDiagnostic Parent Rating Scale 1Yet Barreda Basbas100% (2)
- Adhd Checklist 01Document1 pageAdhd Checklist 01melodyfathi100% (1)
- CaddraGuidelines2011 ToolkitDocument48 pagesCaddraGuidelines2011 ToolkitYet Barreda BasbasNo ratings yet
- Ganatra, Zafar, Qidwai & RoziDocument9 pagesGanatra, Zafar, Qidwai & RoziYet Barreda BasbasNo ratings yet
- Cad DR A Guidelines 2011 Adhd ChecklistDocument1 pageCad DR A Guidelines 2011 Adhd ChecklistYet Barreda BasbasNo ratings yet
- Prevalence of Depression Among Vietnamese Elderly: An Exploratory StudyDocument7 pagesPrevalence of Depression Among Vietnamese Elderly: An Exploratory StudyYet Barreda BasbasNo ratings yet
- Al Shammari & Al SubaieDocument11 pagesAl Shammari & Al SubaieYet Barreda BasbasNo ratings yet
- 1616Document40 pages1616cristinaNo ratings yet
- OgenaDocument32 pagesOgenaYet Barreda BasbasNo ratings yet
- Yunus, Et Al.Document7 pagesYunus, Et Al.Yet Barreda BasbasNo ratings yet
- Teixeira, Et Al.Document13 pagesTeixeira, Et Al.Yet Barreda BasbasNo ratings yet
- Ko & YounDocument9 pagesKo & YounYet Barreda BasbasNo ratings yet
- AcharyyaDocument14 pagesAcharyyaYet Barreda BasbasNo ratings yet
- Choulagai, Sharma & ChoulagaiDocument7 pagesChoulagai, Sharma & ChoulagaiYet Barreda BasbasNo ratings yet
- Sidik, Zulkefli & MustaqimDocument6 pagesSidik, Zulkefli & MustaqimYet Barreda BasbasNo ratings yet
- Fukunaga, Et Al.Document8 pagesFukunaga, Et Al.Yet Barreda BasbasNo ratings yet
- Ko & YounDocument9 pagesKo & YounYet Barreda BasbasNo ratings yet
- AcharyyaDocument14 pagesAcharyyaYet Barreda BasbasNo ratings yet
- Correlates of Depression Among The Soviet Jewish Immigrant ElderlyDocument14 pagesCorrelates of Depression Among The Soviet Jewish Immigrant ElderlyYet Barreda BasbasNo ratings yet
- Ahmed, Siwar, IdrisDocument5 pagesAhmed, Siwar, IdrisYet Barreda BasbasNo ratings yet
- Trejos and BarbozaDocument17 pagesTrejos and BarbozaYet Barreda BasbasNo ratings yet
- Olorunda and AdediranDocument9 pagesOlorunda and AdediranYet Barreda BasbasNo ratings yet
- Journalism Cover Letter TemplateDocument6 pagesJournalism Cover Letter Templateafaydebwo100% (2)
- RODECaster Pro II - DataSheet - V01 - 4Document1 pageRODECaster Pro II - DataSheet - V01 - 4lazlosNo ratings yet
- Pradhan Mantri Gramin Digital Saksharta Abhiyan (PMGDISHA) Digital Literacy Programme For Rural CitizensDocument2 pagesPradhan Mantri Gramin Digital Saksharta Abhiyan (PMGDISHA) Digital Literacy Programme For Rural Citizenssairam namakkalNo ratings yet
- I5386-Bulk SigmaDocument1 pageI5386-Bulk SigmaCleaver BrightNo ratings yet
- Pie in The Sky 3Document5 pagesPie in The Sky 3arsi_yaarNo ratings yet
- DC0002A Lhires III Assembling Procedure EnglishDocument17 pagesDC0002A Lhires III Assembling Procedure EnglishНикола ЉубичићNo ratings yet
- Theories of Economic Growth ReportDocument5 pagesTheories of Economic Growth ReportAubry BautistaNo ratings yet
- Tan Vs GumbaDocument2 pagesTan Vs GumbakjsitjarNo ratings yet
- Actus Reus and Mens Rea New MergedDocument4 pagesActus Reus and Mens Rea New MergedHoorNo ratings yet
- Immovable Sale-Purchase (Land) ContractDocument6 pagesImmovable Sale-Purchase (Land) ContractMeta GoNo ratings yet
- Sewing Machins Operations ManualDocument243 pagesSewing Machins Operations ManualjemalNo ratings yet
- Drug Study TemplateDocument2 pagesDrug Study TemplateKistlerzane CABALLERONo ratings yet
- Volvo B13R Data SheetDocument2 pagesVolvo B13R Data Sheetarunkdevassy100% (1)
- Grace Strux Beton PDFDocument33 pagesGrace Strux Beton PDFmpilgirNo ratings yet
- Fortigate Fortiwifi 40F Series: Data SheetDocument6 pagesFortigate Fortiwifi 40F Series: Data SheetDiego Carrasco DíazNo ratings yet
- BSL-3 Training-1Document22 pagesBSL-3 Training-1Dayanandhi ElangovanNo ratings yet
- Inspection and Test Plan Piling: 1. Document ReviewDocument3 pagesInspection and Test Plan Piling: 1. Document ReviewZara BhaiNo ratings yet
- Chapter 1.4Document11 pagesChapter 1.4Gie AndalNo ratings yet
- Irrig in AfricaDocument64 pagesIrrig in Africaer viNo ratings yet
- Solutions To Questions - Chapter 6 Mortgages: Additional Concepts, Analysis, and Applications Question 6-1Document16 pagesSolutions To Questions - Chapter 6 Mortgages: Additional Concepts, Analysis, and Applications Question 6-1--bolabolaNo ratings yet
- Toshiba Satellite L200 M200 M203 M206 KBTIDocument59 pagesToshiba Satellite L200 M200 M203 M206 KBTIYakub LismaNo ratings yet
- MMMDocument6 pagesMMMReet KanjilalNo ratings yet
- Chapter 123 RevisedDocument23 pagesChapter 123 RevisedCristy Ann BallanNo ratings yet
- 6mm Superlite 70 40t Clear +16as+6mm ClearDocument1 page6mm Superlite 70 40t Clear +16as+6mm ClearNav JavNo ratings yet
- Bs en 1991-1-5 2003 + 2009 Thermal Actions (Unsecured)Document52 pagesBs en 1991-1-5 2003 + 2009 Thermal Actions (Unsecured)Tan Gui SongNo ratings yet
- จัดตารางสอบกลางภาคภาคต้น53Document332 pagesจัดตารางสอบกลางภาคภาคต้น53Yuwarath SuktrakoonNo ratings yet
- NCR Minimum WageDocument2 pagesNCR Minimum WageJohnBataraNo ratings yet
- Types of Electrical Protection Relays or Protective RelaysDocument7 pagesTypes of Electrical Protection Relays or Protective RelaysTushar SinghNo ratings yet
- Project 1. RockCrawlingDocument2 pagesProject 1. RockCrawlingHằng MinhNo ratings yet
- Ss1169 - Telecom Frameworx l1TMFDocument65 pagesSs1169 - Telecom Frameworx l1TMFPrince SinghNo ratings yet