You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
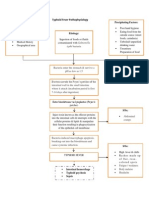
- Typhoid Fever PathophysiologyDocument1 pageTyphoid Fever Pathophysiologynesjyn75% (4)
- Skitchy MicroDocument190 pagesSkitchy MicrohaneenNo ratings yet
- Label KuningDocument2,405 pagesLabel KuningAll Malik Ha100% (4)
- SopDocument11 pagesSopkssehrawat100% (1)
- Kinetics Study of Bioremediation of Industrial Effluents by Pseudomonas Sppandbacillus Sppusing Chemical Oxygen Demand (COD)Document9 pagesKinetics Study of Bioremediation of Industrial Effluents by Pseudomonas Sppandbacillus Sppusing Chemical Oxygen Demand (COD)obaym2002No ratings yet
- Adansonia Digitata (Baobab) Fruit Pulp As Substrate For Bacillus Endoglucanase ProductionDocument7 pagesAdansonia Digitata (Baobab) Fruit Pulp As Substrate For Bacillus Endoglucanase Productionobaym2002No ratings yet
- Production of Itaconic Acid From Jatropha Curcas Seed Cake by Aspergillus TerreusDocument5 pagesProduction of Itaconic Acid From Jatropha Curcas Seed Cake by Aspergillus Terreusobaym2002No ratings yet
- Physicochemical and Ecotoxicological Evaluation of Raw and Biologically-Treated Textile EffluentDocument19 pagesPhysicochemical and Ecotoxicological Evaluation of Raw and Biologically-Treated Textile Effluentobaym2002No ratings yet
- Effect of Centrifugal Pretreatment, PH and Water Activity On The Production of Protease by Pediococcus AcidilacticiDocument5 pagesEffect of Centrifugal Pretreatment, PH and Water Activity On The Production of Protease by Pediococcus Acidilacticiobaym2002No ratings yet
- Bioethanol Production From Mixed Lignocellulosic Substrates Using Cellulolytic Termite Gut Bacteria and YeastDocument1 pageBioethanol Production From Mixed Lignocellulosic Substrates Using Cellulolytic Termite Gut Bacteria and Yeastobaym2002No ratings yet
- HSG PresentationDocument21 pagesHSG Presentationobaym2002No ratings yet
- Chapter 14-15, All Tables and Figures Taken From This ChapterDocument74 pagesChapter 14-15, All Tables and Figures Taken From This ChapterNour MohammedNo ratings yet
- FILARIASISDocument31 pagesFILARIASISArun Shree RNo ratings yet
- Hltinf001 Student Workbook (Word) (c3) .v1.1Document71 pagesHltinf001 Student Workbook (Word) (c3) .v1.1navjot kaur50% (2)
- Detailed Lesson Plan in BiologyDocument7 pagesDetailed Lesson Plan in BiologyElma Grace Sales-DalidaNo ratings yet
- Mumps Lesson PlanDocument6 pagesMumps Lesson PlanRajalakshmi67% (3)
- Apicomplexa (Sporozoa) 5.1general Future and ClassificationDocument10 pagesApicomplexa (Sporozoa) 5.1general Future and Classificationtedela gulumaNo ratings yet
- CD 1Document13 pagesCD 1Don MarcusNo ratings yet
- Polio and PreventionDocument2 pagesPolio and PreventionPintu KumarNo ratings yet
- VILSAN CatalougeDocument97 pagesVILSAN CatalougeSầu VeNo ratings yet
- TorchDocument10 pagesTorchAyen Fajardo-HernalNo ratings yet
- Acute and Chronic PharyngitisDocument10 pagesAcute and Chronic PharyngitisUjjawalShriwastavNo ratings yet
- How To Prevent PhlebitisDocument8 pagesHow To Prevent PhlebitisAffrida Nurlily Chintya WidariNo ratings yet
- Prework QuestionsDocument6 pagesPrework Questionsapi-648757084No ratings yet
- Listanco Abegail Lab Exercise#6Document3 pagesListanco Abegail Lab Exercise#6Abegail ListancoNo ratings yet
- Pyodermas 2014Document41 pagesPyodermas 2014Dudy Humaedi100% (6)
- Unit 1 - Task 1 - Testing My Prior Knowledge - Evaluation Questionnaire (Page 2 of 3)Document3 pagesUnit 1 - Task 1 - Testing My Prior Knowledge - Evaluation Questionnaire (Page 2 of 3)yordy javier saavedra castañedaNo ratings yet
- Capitulo 8 EnterobacteriaceaeDocument6 pagesCapitulo 8 EnterobacteriaceaeLuis RodriguezNo ratings yet
- Course Syllabus - General MicrobiologyDocument3 pagesCourse Syllabus - General MicrobiologyTristan BabaylanNo ratings yet
- Pyricularia Monitoring MethodologyDocument2 pagesPyricularia Monitoring MethodologyDaniel Salazar ParraNo ratings yet
- NO. TGL Nama RM: JANUARI 2014Document481 pagesNO. TGL Nama RM: JANUARI 2014DewieqJunexNo ratings yet
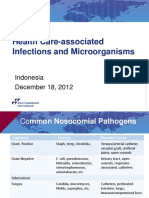
- Microbiology of HAIDocument21 pagesMicrobiology of HAIDevi Pateubih WaosNo ratings yet
- Feline Panleukopenia Virus Infection and Other Viral EnteritidesDocument8 pagesFeline Panleukopenia Virus Infection and Other Viral EnteritidesjohanNo ratings yet
- The Red BookDocument38 pagesThe Red BookPraneel Kumar67% (3)
- Materi DR DR Ari Prayitno SpAK Typhoid Vaccine - Current and New PlatformDocument40 pagesMateri DR DR Ari Prayitno SpAK Typhoid Vaccine - Current and New PlatformMutiara UtiNo ratings yet
- Pneumonia: by DR Randula Samarasinghe Consultant PhysicianDocument34 pagesPneumonia: by DR Randula Samarasinghe Consultant PhysiciansivaNo ratings yet
- Bursa Atrophy at 28 Days Old Caused by Variant Infectious Bursal Disease Virus Has A Negative Economic Impact On Broiler Farms in JapanDocument13 pagesBursa Atrophy at 28 Days Old Caused by Variant Infectious Bursal Disease Virus Has A Negative Economic Impact On Broiler Farms in JapanlalitscNo ratings yet