You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- NICE Guidelines 2009 - Borderline Personality Disorder Treatment and ManagementDocument41 pagesNICE Guidelines 2009 - Borderline Personality Disorder Treatment and ManagementbechurinNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Rhinoplasty Dissection ManualDocument185 pagesRhinoplasty Dissection ManualVikas Vats100% (3)
- PaediatricTuina Elisa RossiDocument7 pagesPaediatricTuina Elisa Rossideemoney3100% (1)
- Acute Effects of Radiation InjuryDocument8 pagesAcute Effects of Radiation InjuryVikas VatsNo ratings yet
- Alternative Method For Fabrication of Power ArmDocument2 pagesAlternative Method For Fabrication of Power ArmVikas VatsNo ratings yet
- Evoked PotentialDocument6 pagesEvoked PotentialVikas VatsNo ratings yet
- Facial AnatomyDocument11 pagesFacial AnatomySneha SthaNo ratings yet
- Vestibuloplasty With Skin Grafting and Lowering of The-HandoutDocument6 pagesVestibuloplasty With Skin Grafting and Lowering of The-HandoutVikas VatsNo ratings yet
- Pikos-Mandibluar Block Autografts For Alveolar Ridge AugmentationDocument17 pagesPikos-Mandibluar Block Autografts For Alveolar Ridge AugmentationVikas VatsNo ratings yet
- BJOMS 2011. Technical Note. Use of Methylene Blue For Precise Peripheral Ostectomy of Keratocystic Odontogenic TumourDocument2 pagesBJOMS 2011. Technical Note. Use of Methylene Blue For Precise Peripheral Ostectomy of Keratocystic Odontogenic TumourVikas Vats100% (1)
- HN 03-2011 Submadibular Salivary Gland Transfer PDFDocument7 pagesHN 03-2011 Submadibular Salivary Gland Transfer PDFVikas VatsNo ratings yet
- 1545 1569 (2000) 037 0243:amouof 2.3.co 2Document5 pages1545 1569 (2000) 037 0243:amouof 2.3.co 2Vikas VatsNo ratings yet
- Computer-Assisted Navigational Surgery in Oral and Maxillofacial SurgeryDocument9 pagesComputer-Assisted Navigational Surgery in Oral and Maxillofacial SurgeryVikas VatsNo ratings yet
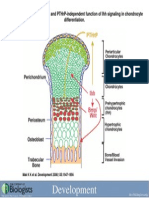
- Development 2008 Jun 135 (11) 1947-56, Fig. 7.Document1 pageDevelopment 2008 Jun 135 (11) 1947-56, Fig. 7.Vikas VatsNo ratings yet
- Drug Development ProcessDocument14 pagesDrug Development Processsnaren76100% (1)
- ABCDEFGHI Systematic Approach To Wound Assessment and ManagementDocument36 pagesABCDEFGHI Systematic Approach To Wound Assessment and ManagementsaerodinNo ratings yet
- q8 Wellness PlanDocument3 pagesq8 Wellness PlanabstabsNo ratings yet
- Draft: The Principles of Infection Prevention and ControlDocument36 pagesDraft: The Principles of Infection Prevention and Controlandrel davidNo ratings yet
- School Health ProgrammeDocument40 pagesSchool Health ProgrammezulfitrieeeNo ratings yet
- Keith R Poskitt - Chronic Ulceration of The LegDocument5 pagesKeith R Poskitt - Chronic Ulceration of The LegKovoor LedchumananNo ratings yet
- r127092130 Gabriel Martinez CUR127092130Document2 pagesr127092130 Gabriel Martinez CUR127092130GabrielNo ratings yet
- SRM Case Studys C05-007Document8 pagesSRM Case Studys C05-007Aqfaq UdeenNo ratings yet
- Wednesday SomersDocument57 pagesWednesday SomersNational Press FoundationNo ratings yet
- Thoracic Radiofrequency AblationDocument2 pagesThoracic Radiofrequency AblationIevgen DanylchukNo ratings yet
- 1n2 OrganicSD-drshakyaDocument26 pages1n2 OrganicSD-drshakyaUMESH KANDELNo ratings yet
- Rules and Guidelines For Mortality and Morbidity CodingDocument5 pagesRules and Guidelines For Mortality and Morbidity Codingzulfikar100% (2)
- PathologyDocument31 pagesPathologyStudy Usmle100% (1)
- CSF Catalogue enDocument76 pagesCSF Catalogue enHarshitShuklaNo ratings yet
- Economic Impact of Medication Nonadherence by Disease Groups: A Systematic ReviewDocument13 pagesEconomic Impact of Medication Nonadherence by Disease Groups: A Systematic ReviewtapsemiNo ratings yet
- Injectable Anesthesia and Analgesia of Birds 5-Aug PDFDocument15 pagesInjectable Anesthesia and Analgesia of Birds 5-Aug PDFYaserAbbasiNo ratings yet
- Drug Study RopivacaineDocument2 pagesDrug Study Ropivacainerica sebabillonesNo ratings yet
- Actinomycetes Staining MethodsDocument14 pagesActinomycetes Staining MethodsvikasNo ratings yet
- Case 1 - Pneumonia (Final)Document4 pagesCase 1 - Pneumonia (Final)Joegie ArioNo ratings yet
- Zoonotic Potentiality of Protozoa: Assignment Subject: ParasitologyDocument7 pagesZoonotic Potentiality of Protozoa: Assignment Subject: ParasitologyArushi PatiyalNo ratings yet
- Review of Antibacterial Medicines For The Treatment of Enteric Fever For The WHO Model List of Essential Medicines 2019 UpdateDocument19 pagesReview of Antibacterial Medicines For The Treatment of Enteric Fever For The WHO Model List of Essential Medicines 2019 UpdateSundas EjazNo ratings yet
- A Clinical Success in The Management of Kotha (Digital Gangrene) by Leech Therapyandpanchtiktaghritaguggulu - A Single Case StudyDocument5 pagesA Clinical Success in The Management of Kotha (Digital Gangrene) by Leech Therapyandpanchtiktaghritaguggulu - A Single Case StudyIJAR JOURNALNo ratings yet
- SIC (Carpio, Kurt Andrew)Document5 pagesSIC (Carpio, Kurt Andrew)Kurt Andrew CarpioNo ratings yet
- Chapter 69Document47 pagesChapter 69Benjamin SchauerteNo ratings yet
- Holding Health Care AccountableDocument37 pagesHolding Health Care AccountableGulalayNo ratings yet
- Oral Probiotic Treatment of Lactobacillus Rhamnosus Lcr35® Prevents Visceral Hypersensitivity To A Colonic Inflammation and An Acute Psychological StressDocument13 pagesOral Probiotic Treatment of Lactobacillus Rhamnosus Lcr35® Prevents Visceral Hypersensitivity To A Colonic Inflammation and An Acute Psychological StressMaria TejedaNo ratings yet
- PlagueDocument31 pagesPlaguelulondon1No ratings yet
- Plan Your DrillDocument4 pagesPlan Your DrillStan BTOB,BTS,TXTNo ratings yet