You might also like
- How To Find Business InformationDocument218 pagesHow To Find Business Informationbibicul1958100% (1)
- Gastrointestinal Anatomy and Physiology: The EssentialsFrom EverandGastrointestinal Anatomy and Physiology: The EssentialsJohn F. ReinusNo ratings yet
- Anorectal DiseaseDocument142 pagesAnorectal DiseaseAb Baby100% (1)
- 9 GitDocument81 pages9 GitAbdurahman Tainy100% (1)
- High Frequency Transformer For Switch-Mode Power SupplyDocument154 pagesHigh Frequency Transformer For Switch-Mode Power Supplybibicul1958No ratings yet
- Learning Activity4.1 (Science Grade 8) : Name: Grade/Score: Year and Section: DateDocument2 pagesLearning Activity4.1 (Science Grade 8) : Name: Grade/Score: Year and Section: DateMa LouNo ratings yet
- APC Computer Magazine Issue 452 March 2018Document116 pagesAPC Computer Magazine Issue 452 March 2018bibicul1958No ratings yet
- Stress UlcerDocument20 pagesStress UlcerTaufik Akbar Faried LubisNo ratings yet
- Nutrition & You - Chapter 3Document30 pagesNutrition & You - Chapter 3Bridget KathleenNo ratings yet
- Gastrointestinal Physiology: By: Zewdu JimaDocument77 pagesGastrointestinal Physiology: By: Zewdu JimaZewdu Jima100% (1)
- Pathophysiology of Chronic ConstipationDocument7 pagesPathophysiology of Chronic Constipationcc vere100% (1)
- Digestive System 2 PhysioDocument108 pagesDigestive System 2 PhysioAbsar AhmedNo ratings yet
- Git Kpbi NisaDocument62 pagesGit Kpbi NisaaristadevyaNo ratings yet
- Git MotilityDocument68 pagesGit MotilityGaurav SinghNo ratings yet
- Control: GIT FunctionsDocument6 pagesControl: GIT FunctionsS ANo ratings yet
- By: Abduljabbar Hamid Jabbar: University of Baghdad-College of Medicine M. B. Ch. BDocument97 pagesBy: Abduljabbar Hamid Jabbar: University of Baghdad-College of Medicine M. B. Ch. BXena XenaNo ratings yet
- 3 Gi Motility (Parts I-Iv) Swallowing & Esophageal MotilityDocument11 pages3 Gi Motility (Parts I-Iv) Swallowing & Esophageal MotilityLinh PhanNo ratings yet
- The GITDocument5 pagesThe GITantoonieNo ratings yet
- GitDocument57 pagesGitbookaccountNo ratings yet
- Anatomy and PhysiologyDocument13 pagesAnatomy and PhysiologyUday Kumar100% (1)
- 2 MotilityDocument37 pages2 MotilityhnavalanNo ratings yet
- Medical Physiology: Gastro-Intestinal SystemDocument192 pagesMedical Physiology: Gastro-Intestinal SystemKamal AhmedNo ratings yet
- Digestive System NotesDocument9 pagesDigestive System NotesLekhana BankiNo ratings yet
- L9-Physiology of Esophagus and Deglutition: Mastication (Chewing)Document4 pagesL9-Physiology of Esophagus and Deglutition: Mastication (Chewing)Boody KhalilNo ratings yet
- Gastrointestinal Hormones Regulating AppetiteDocument23 pagesGastrointestinal Hormones Regulating AppetiteHeba IyadNo ratings yet
- Pendahuluan Gi SystemDocument21 pagesPendahuluan Gi SystemdeasyahNo ratings yet
- Nur Syahirah Binti Mohd Yusri A170291: Nama Dan No. MatrikDocument9 pagesNur Syahirah Binti Mohd Yusri A170291: Nama Dan No. MatrikSyahirah YusriNo ratings yet
- The Cephalic, Oral and Esophageal Phases of The Integrated Response To A MealDocument9 pagesThe Cephalic, Oral and Esophageal Phases of The Integrated Response To A MealpuchioNo ratings yet
- GIDocument47 pagesGIJuliaNo ratings yet
- Lecture 48,49 GIT-Liver Parts 1 and 2Document65 pagesLecture 48,49 GIT-Liver Parts 1 and 2yebadem228No ratings yet
- Git, CVS, Renal&RespirationDocument83 pagesGit, CVS, Renal&Respirationmay noemiNo ratings yet
- Lecture-4 The Small IntestineDocument3 pagesLecture-4 The Small Intestineمرتضى حسين عبدNo ratings yet
- Digestive System: Freshmen Year Program Medical School Universitas Islam Bandung 2011-2012Document125 pagesDigestive System: Freshmen Year Program Medical School Universitas Islam Bandung 2011-2012deasyahNo ratings yet
- Aspects Physiologiques Et Métaboliques de Contrôle de L'ingestion AlimentaireDocument8 pagesAspects Physiologiques Et Métaboliques de Contrôle de L'ingestion Alimentairesoussou.dellacheNo ratings yet
- Print - Chapter 8. Gastric MotilityDocument17 pagesPrint - Chapter 8. Gastric MotilitybelaginaNo ratings yet
- Gastrointestinal Targets of Appetite Regulation in Humans: ILSI SupplementDocument17 pagesGastrointestinal Targets of Appetite Regulation in Humans: ILSI SupplementasfasdfadsNo ratings yet
- GIT 2020 MBCHBWeek SendDocument344 pagesGIT 2020 MBCHBWeek SendTino MapurisaNo ratings yet
- The Digestive SystemDocument26 pagesThe Digestive SystemJasmin RubioNo ratings yet
- The Digestive System: SphinctersDocument33 pagesThe Digestive System: SphinctersJerome EkohNo ratings yet
- Physio. D. NOOR. L4.GITDocument8 pagesPhysio. D. NOOR. L4.GITزين العابدين محمد عويشNo ratings yet
- Gastric MotilityDocument34 pagesGastric MotilityJames IbrahimNo ratings yet
- Gastrointestinal Physiology: Department of Physiology Faculty of Medicine Hasanuddin University MakassarDocument41 pagesGastrointestinal Physiology: Department of Physiology Faculty of Medicine Hasanuddin University MakassarAjeng FikihNo ratings yet
- Nutrition and You 4Th Edition Blake Solutions Manual Full Chapter PDFDocument29 pagesNutrition and You 4Th Edition Blake Solutions Manual Full Chapter PDFlaura.francis115100% (10)
- Nutrition and You 4th Edition Blake Solutions Manual 1Document36 pagesNutrition and You 4th Edition Blake Solutions Manual 1richardsmithxdqnzoywcb100% (23)
- Secretory Functions of GITDocument24 pagesSecretory Functions of GITDr.Nusrat TariqNo ratings yet
- Gastrointestinal Motility-1Document4 pagesGastrointestinal Motility-1TeeNo ratings yet
- Git Notes in ShortDocument13 pagesGit Notes in ShortNeville212No ratings yet
- BCM Week 6 ModuleDocument22 pagesBCM Week 6 Moduleace danielNo ratings yet
- Alneelian University Faculty of Postgraduate Studies Physiology Master Program GIT Physiology GIT Sphincter Student: Salwa Ahmed OsmanDocument13 pagesAlneelian University Faculty of Postgraduate Studies Physiology Master Program GIT Physiology GIT Sphincter Student: Salwa Ahmed OsmanHebara AhmedNo ratings yet
- Gastrointestinal PhysiologyDocument18 pagesGastrointestinal Physiologyfarwafurqan1No ratings yet
- Gastrointestinalsystem 160329122856Document77 pagesGastrointestinalsystem 160329122856Putti AnnisaNo ratings yet
- Dr. Khairun Nisa, Mkes., AIFO Fakultas Kedokteran Universitas Lampung 2014Document35 pagesDr. Khairun Nisa, Mkes., AIFO Fakultas Kedokteran Universitas Lampung 2014Dhita Dwi NandaNo ratings yet
- GIT Physiology Part II by DR A K GutaDocument11 pagesGIT Physiology Part II by DR A K Gutadr.a.k.gupta6924No ratings yet
- Gastrointestinal Physiology: Food Ingestion Food IngestionDocument10 pagesGastrointestinal Physiology: Food Ingestion Food IngestiondrpnnreddyNo ratings yet
- Gastrointestinal SystemDocument21 pagesGastrointestinal Systemsayan27.sikdarNo ratings yet
- Ahp Ut4Document83 pagesAhp Ut4jeniferNo ratings yet
- The Gastric Phase of The Integrated Response To A MealDocument12 pagesThe Gastric Phase of The Integrated Response To A MealpuchioNo ratings yet
- Bsczo 301Document386 pagesBsczo 301JjelNo ratings yet
- Digestive SystemDocument3 pagesDigestive SystemDarwin CauilanNo ratings yet
- ConstipationDocument30 pagesConstipationBareera NudratNo ratings yet
- The Physiology of The GIT and The Liver QuestionsDocument44 pagesThe Physiology of The GIT and The Liver QuestionsDonkeyManNo ratings yet
- Gastroparesis InfoDocument9 pagesGastroparesis Infoडा. सत्यदेव त्यागी आर्य100% (1)
- ControlDocument12 pagesControlSirVietaNo ratings yet
- 03 Digestive System 1Document9 pages03 Digestive System 1Yasin Haq KhanjadaNo ratings yet
- Unit IV - Digestive and Excretory SystemDocument54 pagesUnit IV - Digestive and Excretory SystemsahilNo ratings yet
- Cases 1Document26 pagesCases 1LALITH SAI KNo ratings yet
- DSC Reporting CodesDocument7 pagesDSC Reporting Codesbibicul1958No ratings yet
- DSC Technical Note - Contact ID Codes: ALARMCOM (02) 9564 5812 or 1800 252 960Document2 pagesDSC Technical Note - Contact ID Codes: ALARMCOM (02) 9564 5812 or 1800 252 960bibicul1958No ratings yet
- Canon Fax l120Document58 pagesCanon Fax l120bibicul1958No ratings yet
- Electronics Assembly Electronics Assembly: Surface Surface Mount Mount Technology Technology SMT: SMTDocument24 pagesElectronics Assembly Electronics Assembly: Surface Surface Mount Mount Technology Technology SMT: SMTbibicul1958No ratings yet
- Gastroenterolgy Reference Guide PDFDocument0 pagesGastroenterolgy Reference Guide PDFbibicul1958No ratings yet
- Restoring Factory Hard Drive CapacityDocument73 pagesRestoring Factory Hard Drive Capacitybibicul1958No ratings yet
- Ademco Contact IDDocument5 pagesAdemco Contact IDbibicul1958No ratings yet
- Looking Inside Cells FFFFDocument19 pagesLooking Inside Cells FFFFbibicul1958No ratings yet
- 6 Bit AttenuatorDocument1 page6 Bit Attenuatorbibicul1958No ratings yet
- I. Nursing Care Plan Assessment Diagnosis Planning Intervention EvaluationDocument3 pagesI. Nursing Care Plan Assessment Diagnosis Planning Intervention EvaluationCherubim Lei DC FloresNo ratings yet
- Manguiat, Ncma 111 RomeoDocument4 pagesManguiat, Ncma 111 RomeoCiara ManguiatNo ratings yet
- Study Guide Peg TubeDocument4 pagesStudy Guide Peg TubeDan Dan ManaoisNo ratings yet
- Week 2Document5 pagesWeek 2Maica LectanaNo ratings yet
- 4 5820951304909882278 PDFDocument386 pages4 5820951304909882278 PDFMohamed HamoodNo ratings yet
- Digestive System SummaryDocument2 pagesDigestive System SummaryApple Bottom JeansNo ratings yet
- 2 Biliary Anatomy and EmbrDocument16 pages2 Biliary Anatomy and EmbrShawn GravesNo ratings yet
- BergerDocument8 pagesBergerNeo Rodriguez AlvaradoNo ratings yet
- Lactobacillus SPDocument21 pagesLactobacillus SPمحمد إدريسNo ratings yet
- Case Report of Recurrent Acute Appendicitis in ADocument2 pagesCase Report of Recurrent Acute Appendicitis in Anita alisyahbanaNo ratings yet
- GigiDocument15 pagesGigizulpikarNo ratings yet
- Gastroenterology - DiverticulaDocument1 pageGastroenterology - DiverticulaEugen MNo ratings yet
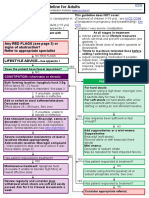
- Laxative Treatment Guideline For AdultsDocument7 pagesLaxative Treatment Guideline For AdultsPurim KTshipNo ratings yet
- Gastrointestinal PhysiologyDocument10 pagesGastrointestinal PhysiologydoreenNo ratings yet
- Tatalaksana Dan Prognosis Tumor PeriampullarDocument16 pagesTatalaksana Dan Prognosis Tumor PeriampullarVerico PratamaNo ratings yet
- Health Teaching Plan Acute Gastroenteritis - Deficient Fluid VolumeDocument4 pagesHealth Teaching Plan Acute Gastroenteritis - Deficient Fluid VolumeAngelica Mateo100% (2)
- SPLANCHONOLOGYDocument5 pagesSPLANCHONOLOGYFadil FadillahNo ratings yet
- Adult Intussusception - A Systematic Review and Meta Analysis 2019Document10 pagesAdult Intussusception - A Systematic Review and Meta Analysis 2019吳醫師No ratings yet
- Esophageal Varices and AtresiaDocument20 pagesEsophageal Varices and Atresiax483xDNo ratings yet
- Nov EB9 E 0809Document1 pageNov EB9 E 0809Moh'dTfailiNo ratings yet
- Peptic Ulcer: By: Therese Jane TimbalopezDocument13 pagesPeptic Ulcer: By: Therese Jane Timbalopezjoyrena ochondraNo ratings yet
- CHOLECYSTOLITHIASISDocument77 pagesCHOLECYSTOLITHIASISMarkie ArqueroNo ratings yet
- Psoas - Ultrasound CasesDocument4 pagesPsoas - Ultrasound CasesMAYNo ratings yet
- Hernia Complications: When To Seek Immediate Medical Attention - Dr. Samrat JankarDocument2 pagesHernia Complications: When To Seek Immediate Medical Attention - Dr. Samrat JankarDr. Samrat JankarNo ratings yet
- Radiology of The Acute Abdomen PDFDocument5 pagesRadiology of The Acute Abdomen PDFAnnisa RahimNo ratings yet
- Diarrhea in AdultsDocument15 pagesDiarrhea in AdultsM.Reza ErlanggaNo ratings yet
- Gastritis and Peptic UlcerDocument30 pagesGastritis and Peptic UlcerKareem DawoodNo ratings yet